
Abstract
Background
Radiofrequency ablation (RFA) is accepted as a minimally invasive treatment of renal cell carcinoma (RCC). However, RFA is not fully evaluated for treating RCC in patients with von Hippel Lindau (VHL) disease who cannot undergo surgery due to serious postoperative morbidity or mortality.
Purpose
To evaluate the role of RFA of RCC in patients with VHL disease previously undergoing renal surgery.
Material and Methods
Percutaneous RFA was performed for treating 14 RCCs in six patients who had undergone radical nephrectomy (n = 3) or repeated nephron-sparing surgery (n = 3). Treatment feasibility, complications, outcome, and the change of renal function were evaluated.
Results
To completely ablate 14 RCCs, 23 ablations during 12 sessions were necessary. Of 14 RCCs, nine were in proximity (<5 mm) to one or more following organs: bowel (n = 4), ureteropelvic junction or pelvis (n = 2), psoas muscle (n = 2), vascular pedicle (n = 1), and pancreas (n = 1). Of 12 sessions, one major complication (pneumothorax) developed in one session (8%). No residual or recurrent tumors were identified at the ablation areas. However, new three solid tumors less than 1 cm in diameter developed during the follow-up period but ablation was withheld until these tumors had grown to more than 1 cm in size. The mean level of serum creatinine increased with 6.4% and the mean estimated glomerular filtration rate decreased by 12.8% after the last ablation compared to those before the initial ablation (P < 0.05).
Conclusion
Despite technical difficulties, percutaneous RFA is a promising treatment for VHL patients who cannot undergo surgery because of excellent treatment outcome and minimal change of renal function.
Keywords
Radical nephrectomy has been considered as gold standard in the treatment of renal cell carcinoma (RCC). However, patients undergoing this treatment may have renal function gradually impaired (1, 2). Recently, nephron-sparing surgery (NSS) has become a treatment of choice for small RCCs to preserve renal function since there is no difference between radical nephrectomy and NSS regarding the long-term outcome (3).
However, even NSS can be of limited value for treating patients with von Hippel Lindau (VHL) disease that is characterized by multifocal, bilateral, and recurrent RCCs. Once a surgical procedure is performed, repeated surgery is complicated due to postoperative fibrosis and subsequent postsurgical morbidity and/or mortality. In addition, even partial nephrectomy can cause significant reduction of the renal function following treatment of small RCC (4). Therefore, percutaneous radiofrequency ablation (RFA) is widely used for treating hereditary RCC in patients with VHL disease as well as a sporadic RCC in selected patients with co-existing medical problems.
Previous reports about RFA of hereditary renal tumors had some limitations (5, 6). These tumors were small (<3 cm) in size, percutaneously accessible, and safely treatable. Thus, lesions in proximity to bowel or great vessels were excluded for RFA treatment (5). Otherwise, laparoscopic approach was performed to these inaccessible lesions although being more invasive than a percutaneous approach (6). However, percutaneous RFA has been improved technically so that RCC's in proximity to critical organs can be treated regardless of tumor location (7).
There are few reports describing the technical aspects or the outcome of percutaneous RFA in treating RCC in patients with VHL disease who previously had undergone radical nephrectomy or repeated NSS (8). These patients have a potential to have increased renal failure due to renal tissue loss if their recurrent renal tumors should be surgically re-treated. The purpose of our study was to evaluate the technical feasibility, complications, outcome of RFA and change of renal function in treating RCC in VHL patients who were not able to undergo any surgical procedure due to serious postoperative morbidity or mortality.
Material and Methods
Subjects
Between October 2005 and July 2010, data were retrospectively gathered from seven consecutive patients with VHL disease. Of these patients, four had undergone unilateral radical nephrectomy and three, repeated NSS including two partial bilateral nephrectomies (n = 1), one partial nephrectomy and seven bilateral enucleation (n = 1), and one partial nephrectomy and six bilateral enucleation (n = 1), respectively. VHL disease was clinically diagnosed (9, 10). One of these patients was excluded from our study because she had pulmonary metastases before the scheduled RFA sessions for multiple renal tumors.
The remaining six patients (M:F ratio = 4:2, age range 23–51 years, mean ± standard deviation 36.3 ± 10.4 years) underwent percutaneous RFA of altogether 14 renal tumors (size range 1–4.2 cm, 2.0 ± 0.9 cm) that were detected on follow-up CT images after primary surgery. The inclusion criteria for ablating renal tumors were (a) 1 cm or larger renal tumors and (b) a non-fatty solid tumor that was enhanced by 20 HU or more after intravenous contrast material administration, or (c) a Bosniak category III or IV cystic tumor. Of the 14 masses, 12 were solid (1.0–2.3 cm, 1.7 ± 0.4 cm) and two were Bosniak category IV cysts (3.4–4.2 cm, 3.8 ± 0.6 cm). There were 13 masses in five patients and a single mass in one patient. Seven masses were located in the right kidney and seven in the left.
The follow-up period after ablation ranged from 7 to 53 months (26.5 ± 17.0 months): three patients were followed for less than 2 years (7–19 months, 13 ± 6 months) and three patients for 2 years or more (30–53 months; 40 ± 11.7 months). Follow-up imaging studies were unenhanced and contrast-enhanced CT examination, which were performed at 1, 6, and 12 months during the first year, every 6 months during the second year, and every 12 months from the third year after RFA was completed (11).
RFA procedure
Percutaneous RFA was performed by two radiologists under CT guidance using a Lightspeed QX/I (GE Healthcare, Milwaukee, WI, USA) or Aquilion 64 (Toshiba, Otawara, Japan). A cool-tip RF system (Covidien, Mansfield, MA, USA) was used for ablation. In most cases, unenhanced CT was performed during ablation but contrast-enhanced CT was done for localization of the tumors. Ablation duration was determined depending on the tumor size or delivered power (12) and ranged from 1–12 minutes (7.6 ± 3.6 minutes). The ablation procedures were not performed under general anesthesia but conscious sedation using penthidine HCI alone before 2008 or both of fentanyl and midazolam after 2008.
Data analysis
Data were analyzed to evaluate (a) technical feasibility of RFA, (b) complications, (c) change of renal function before and after ablation, and (d) short-term outcome.
Prior to ablation, organs located less than 5 mm away from a RCC were identified as they were regarded susceptible to thermal injury during the ablation (13). What measures that were taken to prevent thermal injury to the adjacent organs were also recorded.
Complications occurring during or following the ablation and if it required a specific treatment (major complication) or conservative treatment (minor complication) were determined as well (7). Mean serum creatinine (sCr) and estimated glomerular filtration rate (eGFR) were also recorded. Both sCr and eGFR were measured within one month prior and at six months after the ablation.
Whether there was a residual or recurrent tumor following the ablation was determined by follow-up (11). When a new solid tumor or a cystic tumor of Bosniak category III or IV was detected at the follow-up CT examination, tumors <1 cm were observed until they reached 1 cm or more, and tumors ≥1 cm were re-treated with RFA.
Statistical analysis
Statistical analyses were performed using commercially available software (PASW Statistics, version 17, Chicago, IL, USA). Wilcoxon matched-pairs signed-rank test was used to compare the mean sCr level and eGFR before and after ablation. A P value of <0.05 was considered statistically significant.
Results
Of 14 renal masses, nine were <5 mm away from one or more adjacent organs including the ascending colon (n = 2), small bowel (n = 2, including duodenum and jejunum), ureteropelvic junction (UPJ) or kidney pelvis (n = 2), psoas muscle (n = 2), pancreas (n = 1), and the vascular pedicle (n = 1) (Table 1). The remaining five renal masses were surrounded by renal parenchyma (n = 4) or perirenal fatty tissue (n = 1).
Percutaneous RFA of 14 RCCs in six VHL patients with a history of renal surgery
*Distance of less than 5 mm between RCC and adjacent organs
To avoid injury to adjacent organs, one or more the following prevention methods were performed: patient's position change (n = 6), levering electrode (n = 2), hydrodissection (n = 1), and retrograde catheterization (n = 1). Changing patient's position alone separated the ascending colon or psoas muscle sufficiently away from the adjacent renal tumor (n = 2). One renal tumor was not displaced from the psoas muscle by position change alone and a levering electrode was added to prevent thermal injury.
One renal tumor was displaced from both the duodenum and ascending colon by hydrodissection because position change and levering electrode was not considered sufficient (Fig. 1). Two renal masses were not displaced from the jejunum and pancreas by position change alone. However, a small amount of peri-tumoral hemorrhage occurred during tumor targeting and it separated jejunum or pancreas >5 mm from the RCC. Without requiring hydrodissection, ablation was safely performed and no active bleeding was confirmed on post-ablation contrast-enhanced CT images.
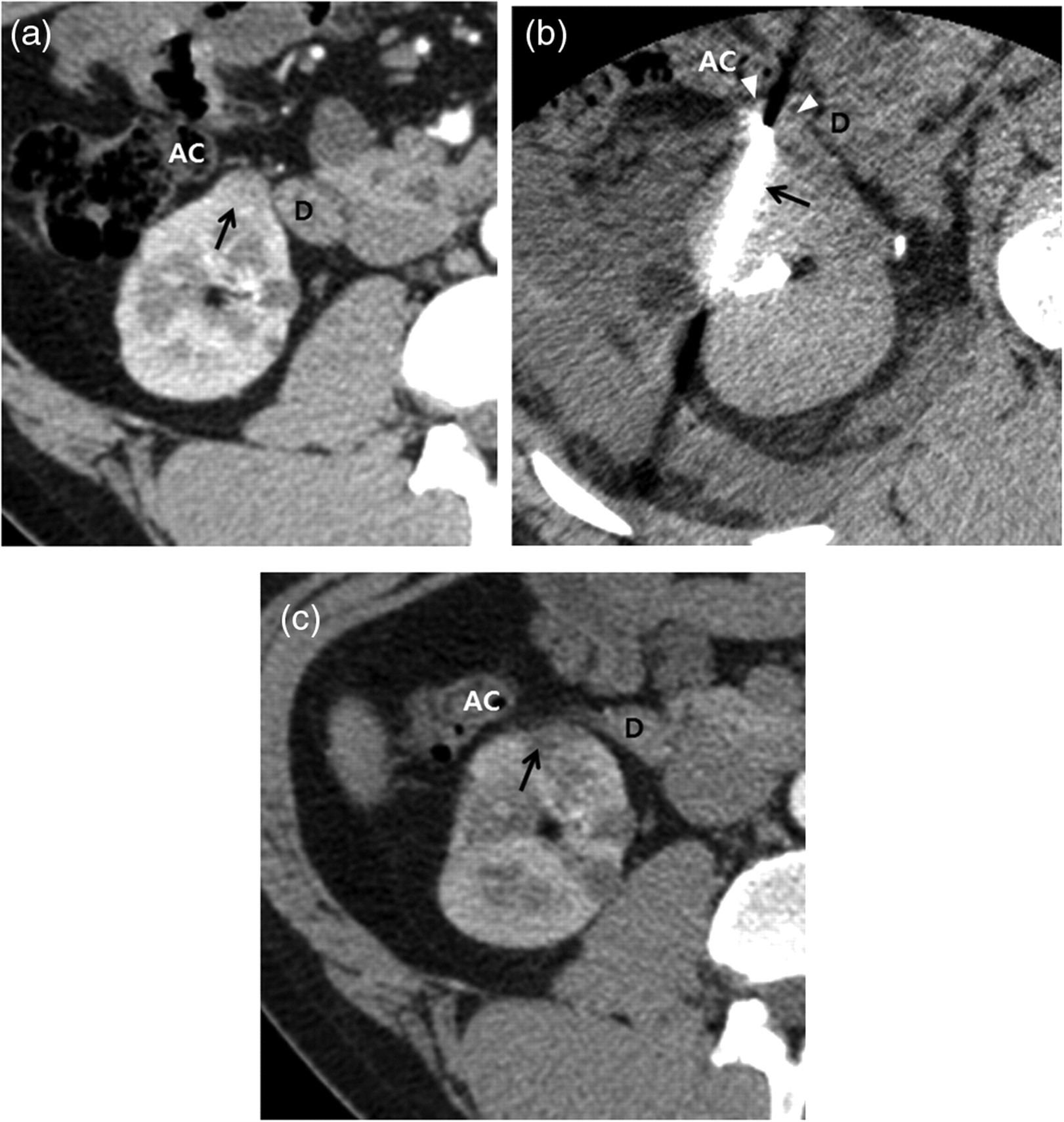
Hydrodissection preventing bowel injury in a 27-year-old man (patient 2). (a) Contrast-enhanced axial CT image shows a solid RCC (arrow) that is <5 mm away from both the duodenum (D) and ascending colon (AC). (b) Unenhanced axial CT image shows both the duodenum and ascending colon are displaced by hydrodissection (arrowheads). The RCC is targeted by an RF electrode (arrow). (c) Contrast-enhanced axial CT image 15 months following ablation shows the reduced RCC (arrow). Both the duodenum and ascending colon are intact
One renal tumor in proximity to UPJ was safely ablated by retrograde catheterization alone using a stent (Fig. 2). One renal tumor less than 5 mm from the renal pelvis but more than 5 mm from the UPJ, and one renal tumor touching the vascular pedicle was also safely treated without use of any prevention method.
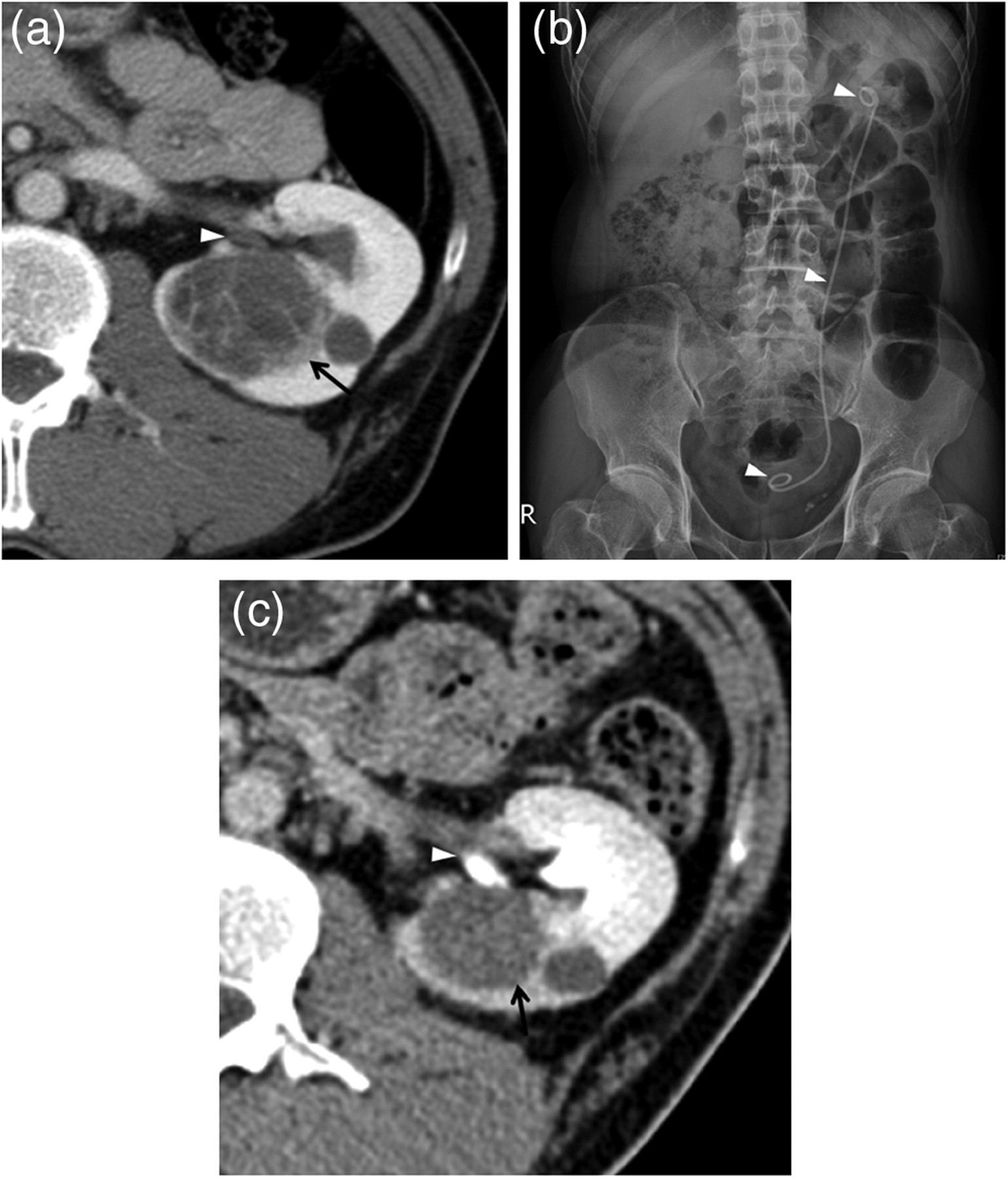
Retrograde catheterization preventing ureter injury in a 42-year-old man (patient 6). (a) Contrast-enhanced axial CT image shows a Bosniak IV cystic tumor (arrow) that is <5 mm away from ureteropelvic junction (arrowhead). (b) Simple radiograph shows a ureter stent (arrowheads) that is indwelled by retrograde catheterization prior to ablation. (c) Contrast-enhanced axial CT image 13 months following ablation shows a completely ablated RCC and an intact ureteropelvic junction
Of the 12 sessions, one (8%) had a major complication developing after ablation of an upper polar RCC. An intentional pneumothorax was made to target the tumor because an oblique direction of the RF electrode could injure other organs such as the renal sinus or spleen. This complication reduced the oxygen saturation less than 90%. Thus, approximately 500 cc of air was aspirated using an 18-gauge needle and oxygen saturation increased to more than 99%.
Of 12 sessions, seven (58%) had one or more minor complications: perirenal hematoma in four, segmental infarction in three, transient hematuria in two, and subcapsular hematoma in one. None of these minor complications required any specific treatment but was observed.
The levels of sCr before the initial ablation and after the last ablation ranged 0.78–1.28 mg/dl (1.11 ± 0.18 mg/dl) and 0.83–1.39 mg/dl (1.18 ± 0.19 mg/dl), respectively. It increased 4.6–9.0% (6.4 ± 1.9%) (P < 0.05) (Table 2).
Comparison of serum creatinine (sCr) and estimated glomerular filtration rate (eGFR) before initial ablation and after last ablation
*Difference, percentage of the last sCr or eGFR minus the initial sCr or eGFR
The eGFR before the initial ablation and after the last ablation ranged 62–97 mL/min (77 ± 13 mL/min) and 56–92 mL/min (67 ± 13 mL/min), respectively. It decreased 5.1–20.7% (12.8 ± 5.6%) (P < 0.05).
A total of 23 ablations during 12 sessions were necessary to completely ablate 14 tumors. After the scheduled sessions were completed, no residual or recurrent tumors occurred at the ablation areas for 7–53 months (mean 26.5 ± 17.0 months). Of 14 tumors, seven were completely ablated after a single ablation, six after two ablations, and one after four ablations. However, three new solid tumors were detected at another renal parenchyma in two patients. These tumors were detected at 6-, 32-, and 45-month CT examinations after the final ablation. These nodules were 7.0 mm, 9.1 mm, and 9.3 mm. The patients were placed under observation and scheduled for RFA if the new tumors increased to 1 cm or more.
Discussion
Surgical removal of RCC in patients with VHL disease with previous renal surgery is difficult due to several clinical or technical considerations. First, urologists are reluctant to perform NSS due to postoperative fibrosis and adhesion. Second, patients may have renal failure even if the tumor is treated with NSS. Third, hereditary RCC is frequently multifocal and recurrent over the patient's life, in contrast to sporadic RCC. Therefore, the best approach for managing these tumors is not only to remove as many tumors as possible, but also to preserve as much renal tissue as possible, even if microscopic cancerous foci remain (14). Therefore, percutaneous RFA is considered the most suitable treatment that can overcome those surgical limitations (8).
Percutaneous RFA may cause thermal injury to organs that are <5 mm away from the RCC (13). The bowel should be the primary concern during ablation. A thermally injured bowel may develop wall thickening, adhesion, or perforation, requiring emergency surgery to prevent abscess formation and sepsis (7, 13, 15, 16). Hydrodissection is a useful method to prevent thermal injury to the bowel (3, 7, 16). However, this prevention method requires not only additional invasive procedures, but also increases radiation exposure if CT-guided RFA procedures are used. Non-invasive methods such as changing the patient's position and/or use of levering electrodes are as effective as hydrodissection in separating the bowel from the RCC (7, 17).
The UPJ is also susceptible to thermal injury during ablation of RCC, which is arising from the inferior-medial aspect of kidney. This can complicate ureteral stricture requiring a permanent nephrostomy or nephrectomy. If ureteral injury is possible, retrograde catheterization should be performed before ablation and cool fluid should be infused during ablation via catheter (18, 19). The mechanism of this prevention method is a heat sink effect with cool fluid removing the heat energy delivered to the ureter during ablation. In our case, however, internal catheterization and indwelling for four weeks was sufficient to avoid ureteral injury in without internal cooling. In addition, contrast-enhanced CT was used to scan for lesion localization in the central tumors. Iodine contrast material can promote urine excretion, also leading to a heat-sink effect. In this way, unnecessary heat delivered to the ureter can be reduced during ablation procedures. However, our prevention method requires additional proof of its efficacy in protecting the ureter from thermal injury.
Peritumoral hemorrhage is not a rare complication during biopsy or ablation of RCC. This complication may widen the distance between the RCC and neighboring organs. In our study, unexpected peritumoral hemorrhage was helpful for safe ablation of RCC without requiring hydrodissection. Interventional radiologists should strive to prevent this complication, however, if it separates the RCC from the neighboring organs by >5 mm, hydrodissection may not be necessary for safe ablation. Infusing fluid into anterior pararenal space is not technically simple. Targeting a RCC is also difficult because the skin-to-tumor distance is farther than before hydrodissection (16). Despite peritumoral hemorrhage, cancer seeding is known to be extremely rare (20, 21).
Prevention methods were not performed in our study in cases in which the ablating RCCs abutting the vascular pedicle or renal pelvis. Large vessels (>3 mm) were not injured because of a heat-sink effect (22). Blood flowing within the large vessels removed heat delivered during ablation to the vessel wall. Thus, RFA of RCC abutting the large vessels is not likely to cause injury to vessel walls, but to the residual RCC. For the same reason, RFA of RCC abutting the renal pelvis seldom causes stricture, in contrast to ablation of an RCC abutting the ureter, although this requires more investigation.
Our results showed that the only major complication occurred due to intentional pneumothorax. This complication was easily corrected with a simple aspiration. Most intentional pneumothorax requires conservative treatment such as bed rest and nasal oxygen supply instead of additional interventional treatment (23, 24). However, great care should be taken in case that an intentional or accidental injury is made to emphysema, which can cause tension pneumothorax requiring emergency treatment (24).
Renal function is reduced after ablation because neighboring normal tissue as well as the RCC must be ablated to prevent residual or recurrent tumors. However, RFA reduces renal function less than extirpative treatment (25). The mean eGFR may decrease approximately 9% after RFA and 30% after partial nephrectomy (4, 8). Therefore, RFA is of great importance for treating RCC in patients with marginal renal function who have a history of a radical nephrectomy or repeated NSS. Weisbrod et al. reported that percutaneous cryoablation may also cause minimal loss of renal function of RCCs following treatment of renal masses in a solitary kidney (26). However, the tumors in their study were not hereditary, but sporadic RCCs. No reports have shown that cryoablation is an effective treatment for multifocal, recurrent, hereditary RCCs.
The RFA treatment of a small renal tumor <1 cm was postponed until the lesion grew to 1 cm or larger for the following reasons. First, characterizing a mass <1 cm as solid and enhancing is often difficult, despite the state-of-the-art imaging techniques of CT and MRI (27). Second, if a renal tumor is <1 cm, it is difficult to target. Third, even if a renal tumor <1 cm is an RCC, it seldom metastasizes (28). Finally, if a renal tumor is <1 cm, the possibility of benign diagnosis is very high (29). Simple observation is considered the management choice for small tumors (28).
Our study had some limitations. First, it was performed retrospectively and thus may have been affected by selection bias. Second, a small number of cases were included. Hereditary renal cancer is so rare that it is not appropriate for a prospective study or a retrospective study with a large sample. Thus, our study used a Wilcoxon signed rank test for statistical analysis since the study population was small, and the data could not be analyzed by probability distribution. Third, the renal tumors in our study were not histologically confirmed. In cases of a small, solid renal tumor (≤3 cm), the possibility of a benign tumor is higher than a larger tumor (>3 cm). Generally, renal mass biopsy should be performed prior to ablation or surgery since it is cost-effective. However, RCCs arising from VHL disease are characterized as multifocal and recurrent tumors. In cases where multiple renal solid tumors are detected in patients with VHL disease, image-guided biopsy is not necessary to confirm pathologic diagnosis of all tumors. If all lesions have same imaging features, sampling one is satisfactory (30). If cystic masses are detected, they were evaluated according to Bosniak Classification. When cystic renal masses were categorized as Bosniak III or IV category, ablation therapy or surgery was performed regardless of positive or negative biopsy results. We had strict inclusion criteria because of the absence of pathologic proof. RFA was performed only when all tumors were newly detected after surgery, and were solid or Bosniak III or IV cystic masses.
In conclusion, even though percutaneous RFA requires special techniques in some cases to prevent organ injury, this minimally invasive treatment can safely ablate all RCCs in VHL patients with a history of radical nephrectomy or repeated NSS. Therefore, percutaneous RFA will be a promising treatment for patients who cannot undergo surgical procedures, for not only treating as many RCCs as possible, but also preserving renal function as much as possible.