
Abstract
Portopulmonary venous anastomosis (PPVA), which has been rarely reported in conventional CT and MR studies, is an unusual collateral pathway in patients with portal hypertension. It has clinical implications related to right-to-left shunt that are different from the clinical implications related to other more usual portosystemic shunts in portal hypertensive patients. Here, we report the dynamic CT and MRA findings of a case of PPVA in a patient with portal hypertension, directly demonstrating the shunt flow from the paraesophageal varix to the left atrium via the right inferior pulmonary vein.
Portopulmonary venous anastomosis (PPVA) is a potential, but exceptional, collateral pathway rarely detected in patients with portal hypertension. Unlike other portosystemic pathways in portal hypertension patients, PPVA leads to a right-to-left shunt and thus has clinical implications dissimilar to those of a portosystemic shunt. The reported complications of a portopulmonary shunt via PPVA include cardiac failure and systemic arterial embolism (1, 2). Therefore, radiologists should be aware of this unusual collateral pathway. There have been only a few cases describing the identification of PPVA using conventional CT and MRI (3, 4). We report herein the dynamic CT and MRA findings of PPVA in a patient with portal hypertension.
Case report
A 57-year-old man with liver cirrhosis was admitted to our hospital for liver transplantation. During the initial examination, a suspicious finding of a right paraspinal soft tissue opacity was noted on the chest radiograph (Fig. 1). Contrast-enhanced chest CT was performed using a 64-channel multidetector CT scanner (Somatom Sensation 64; Siemens Medical Solutions, Erlangen, Germany) after intravenous injection of 100 mL of a non-ionic contrast agent (Ultravist 300, Bayer Schering Pharma AG, Berlin, Germany) at a rate of 2.5 mL/s with a 59-s scan delay, using the following parameters: 120 kVp, 130 mAs, collimation = 64 × 0.6 mm, pitch = 1.2, and rotation time = 0.5 s. The CT scan revealed a markedly engorged paraesophageal varix which directly communicated with the right inferior pulmonary vein (Fig. 2).
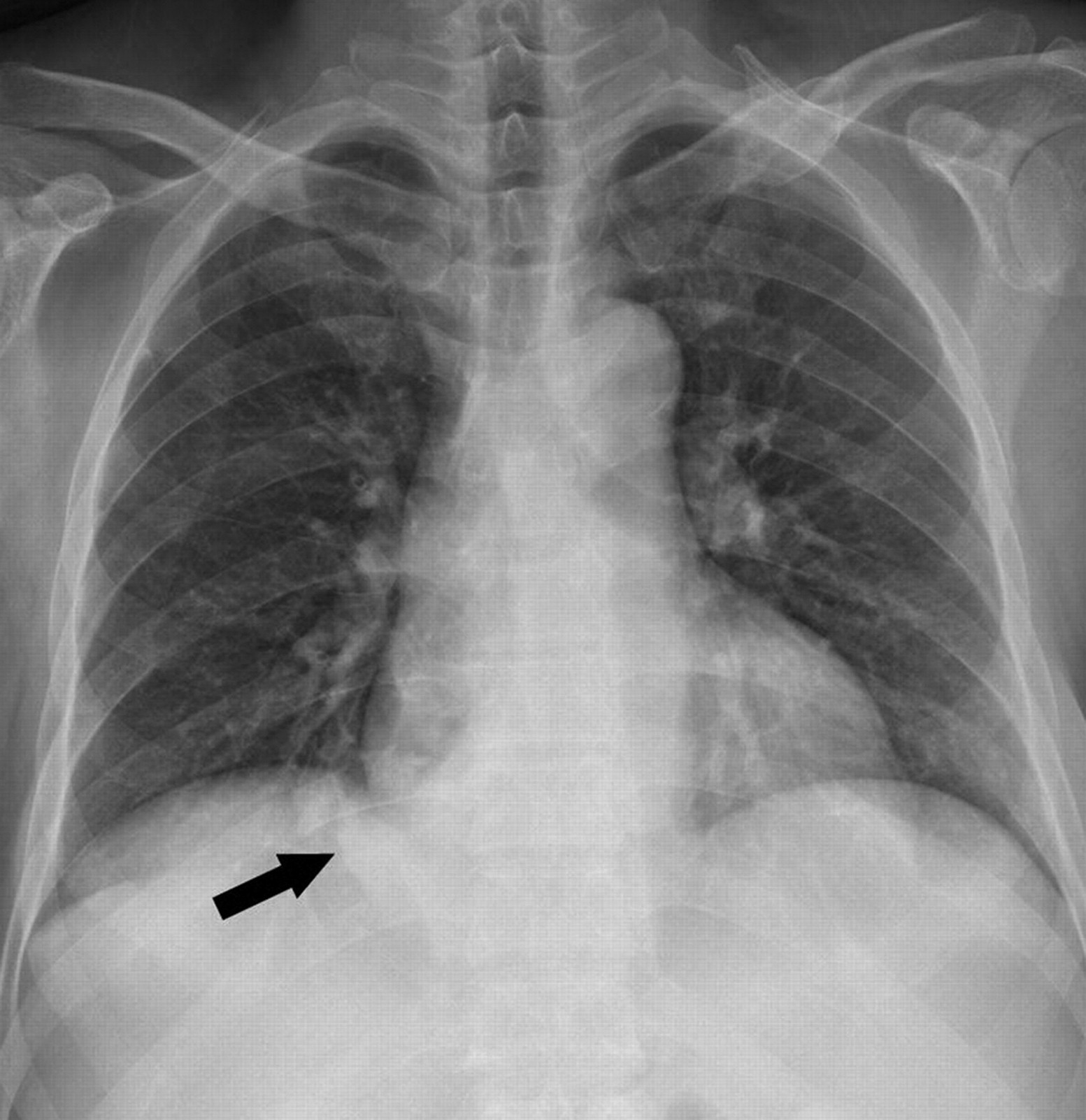
Chest PA radiograph shows an abnormal right paraspinal soft tissue opacity (arrow)

Contrast-enhanced chest CT reveals that the markedly engorged paraesophageal varix is in direct communication with the right inferior pulmonary vein. Note the lobulated contour of the hepatic dome suggesting liver cirrhosis with minimal ascites
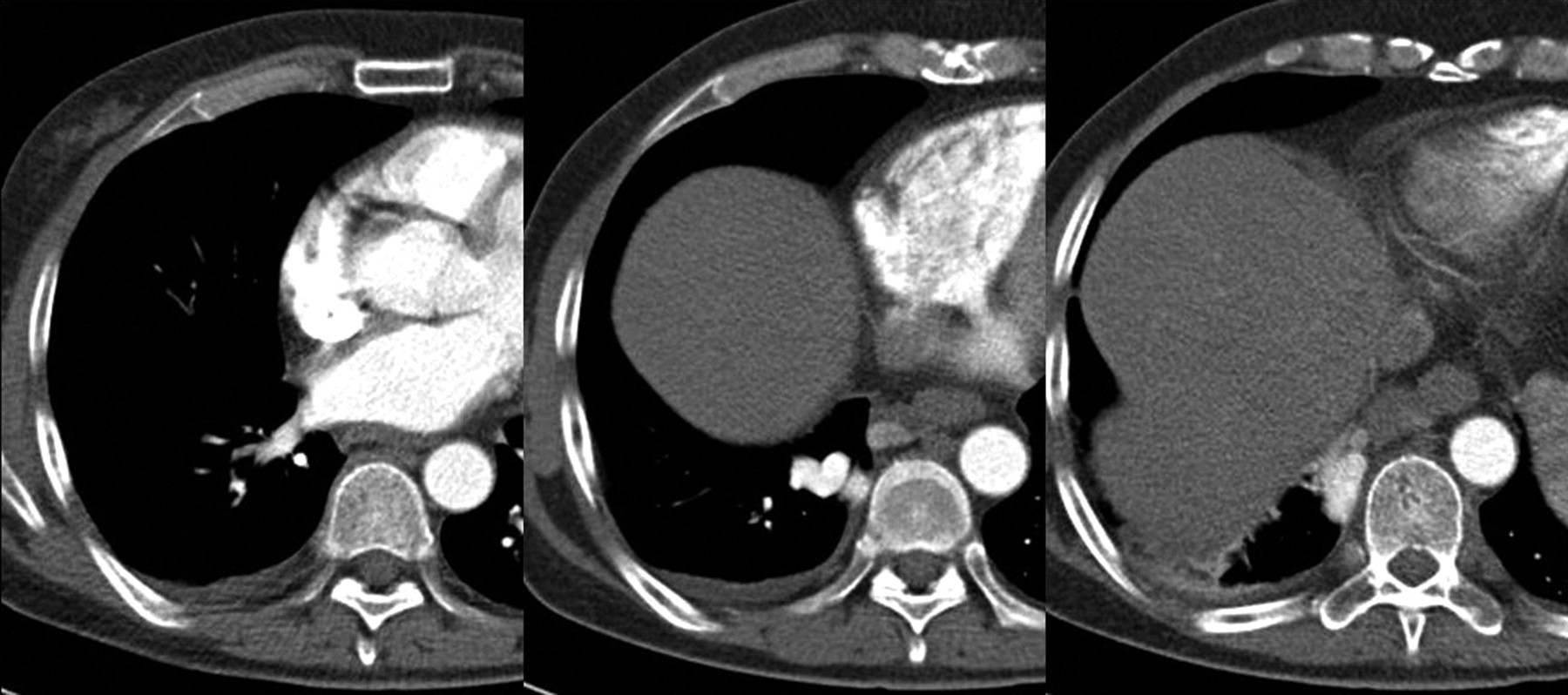
Liver dynamic CT and MRA of the abdomen, which were routine imaging studies before liver transplantation, also showed this abnormal portopulmonary collateral. The liver dynamic CT scan was performed with a 64-channel multidetector CT scanner (Somatom Sensation 64; Siemens Medical Solutions, Erlangen, Germany) after intravenous injection of 110 mL of a non-ionic contrast agent (Ultravist 300, Bayer Schering Pharma AG, Berlin, Germany) at a rate of 3.5 mL/s with the following parameters: 120 kVp, 140 mAs, collimation = 64 × 0.6 mm, pitch = 0.7, and rotation time = 0.5 s. The timing of the arterial phase was determined with real-time bolus tracking in the abdominal aorta at the level of the diaphragm, with a detection threshold of 120 Hounsfield units (HU). Arterial phase imaging was started with a 12-s delay after contrast infusion, and the delay times for the portal venous phase and delayed phase were 48 and 93 second after initiation of contrast infusion, respectively. On images of the arterial phase of the CT scan, a non-enhancing low-density area was noted within the contrast-filled right inferior pulmonary vein and the left atrium (Fig. 3). We considered this low-density area to be non-opacified blood originating from the paraesophageal varix via a portopulmonary shunt. The findings of the arterial phase dynamic subtraction MRA of the abdomen, which was performed using 3.0T system (Magnetom Verio; Siemens Medical Solutions, Erlangen, Germany) after intravenous injection of 10 mL of gadobutrol (Gadovist, Bayer Schering Pharma AG, Berlin, Germany) at a rate of 1 mL/s and imaged with a 3D-FLASH sequence (TR/TE = 2.8/1.0 ms, flip angle = 24 degrees), were identical to those of the dynamic CT. Interestingly, on the portal and delayed phase dynamic subtraction MRA, this shunt flow presented as a jet-flow of high signal intensity within the dark blood-filled left atrium (Fig. 4).

The early arterial phase of the liver dynamic CT demonstrates non-enhancing low density (arrows) within the contrast-filled right inferior pulmonary vein and the left atrium, which represents the non-opacified blood originating from the paraesophageal varix via the portopulmonary shunt

Coronal image of the portal phase dynamic subtraction MRA of the abdomen (a) and axial re-formatted images at the level of the inferior pulmonary vein (b) reveal the portopulmonary shunt (arrows) as a jet-flow of high signal intensity within the dark blood-filled left atrium. Note the very large tortuous coronary vein (arrowheads) communicating with the engorged paraesophageal varix (long thin arrows) on the coronal image
The patient had no symptoms or laboratory findings related to a right-to-left shunt. The patient underwent living donor liver transplantation. In the operating field, a much engorged coronary vein and paraesophageal varix were detected, but the existence of PPVA was not identified because only the intra-abdominal approach was done. Ligation of the coronary vein was not performed. An abdominal CT taken 3 months after liver transplantation showed a significant regression of the previously engorged right inferior pulmonary vein (Fig. 5).
Contrast-enhanced CT after liver transplantation shows significant regression of the previously engorged right inferior pulmonary vein
Discussion
Portopulmonary venous anastomosis has been recognized as one of the hepatofugal collaterals observed in patients with portal hypertension. In 1957, Calabresi et al. (5) demonstrated the existence of PPVA using postmortem angiography on 10 human cadavers with advanced liver cirrhosis. In two of these cases, gross anastomoses between the portalvenous system and the pulmonary venous system were detected. Sano et al. demonstrated PPVA in five of 15 patients with liver cirrhosis or chronic hepatitis in their study using cineportography and contrast echocardiography in 1984 (6). Khaliq et al., in their pathologic study of PPVA using experimentally induced cirrhosis in five rats, reported that PPVA was present in all five rats if microscopic shunts were included (7). These results suggest that subclinical PPVA may exist in humans as well.
In contrast to other portosystemic collateral pathways in portal hypertension patients, PPVA leads to a right-to-left shunt. Blackburn reported a case of the development of a large portal-pulmonary venous anastomosis after partial esophagogastrostomy in a patient with portal hypertension; this anastomosis played a significant role in the patient's death from cardiac failure (1). Additionally, PPVA is a potentially dangerous channel that can result in systemic arterial embolism. Ellman et al. reported two cases in which particles of Gelfoam used to embolize the coronary and short gastric veins passed into the systemic arterial circulation through a portopulmonary anastomosis and embolized in the brain, spleen and heart (2).
Although the observation of PPVA in subjects with portal hypertension is not very rare in postmortem and animal studies and even in contrast echocardiographic examinations (5–7), there have been only two cases in which CT findings and one case in which MRI findings identified portopulmonary anastomoses in portal hypertensive patients (3, 4). The present case demonstrated direct visualization of the shunt blood flow into the left atrium from the paraesophageal varix through the pulmonary vein using dynamic CT and MRA.
When the presence of an engorged pulmonary vein connected to a paraesophageal varix is noted on contrast-enhanced CT images, the presence of PPVA can be easily confirmed. In patients with PPVA, the early arterial phases of dynamic CT and MRA show intravascular low density or a low signal within the contrast-enhanced inferior pulmonary vein or the left atrium due to non-enhancing blood from the paraesophageal varix. Moreover, as in the present case, this shunt flow can be demonstrated as a jet-flow of high signal intensity within the dark blood-filled left atrium on the portal and delayed phase dynamic subtraction MRA, resulting from the contrast-filled blood originating from the paraesophageal varix, which emanates from the right inferior pulmonary vein into the left atrium.
Generally, CTA may demonstrate more detailed anatomy than MRA. Therefore, the diagnostic performance of MRA may be inferior for the detection of small PPVA. However, Lee et al. recently reported that both CTA and MRA can provide a complete evaluation of the hepatic vascular anatomy in living donor candidates (8). The continuing technological development of MRA, such as increased gradient strength, surface coils with better sensitivity, and parallel imaging, may provide improved diagnostic value with the benefit of flow directional information and no radiation exposure.
Although portopulmonary shunt via PPVA has been rarely reported in CT and MR studies, it has clinical implications related to right-to-left shunt that are different from the clinical implications related to other portosystemic shunts. Therefore, the existence of PPVA should be determined during the interpretation of routine CT and MR images in patients with liver cirrhosis or portal hypertension.