
Abstract
Background
Primary breast sarcoma is very rare. Most reports regarding sarcoma of the breast are clinical observations or pathological series and provide either no or inconstant radiological information. Radiological publications consist predominantly of isolated case reports or small series.
Purpose
To determine the prevalence, clinical signs, and radiological features of primary breast sarcoma.
Material and Methods
This is a retrospective review of 21 patients with breast sarcoma. All patients were female and their median age was 66 years (range 27–86). In all patients the diagnosis was confirmed histopathologically.
Results
The prevalence of breast sarcoma was 0.1% of all identified cases with breast malignancies. Clinically, all patients presented with solitary painless breast lumps. There was no uni- or bilateral axillary lymphadenopathy. On mammography (n = 19), two mammographic patterns could be identified: breast masses (68%), and architectural distortion (32%). On ultrasound (n = 8), most lesions were homogeneously hypoechoic, lobular or oval in shape with microlobulated or indistinct margins. On magnetic resonance imaging (n = 3), marked inhomogeneous contrast enhancement was seen in all investigated cases.
Conclusion
The imaging findings of primary breast sarcoma are not pathognomonic. However, they should be taken into consideration in the differential diagnosis of breast lesions.
Ductal and lobular carcinomas are the most frequent malignant tumors of the breast. Breast sarcoma is very rare (1). According to the literature, the true prevalence of primary breast sarcoma (PBS) is difficult to ascertain (1–3). Most reports regarding PBS are clinical observations or pathological series and provide either no or inconstant radiological information (1–4). Radiological publications consist predominantly of isolated case reports or small series (5–7).
Therefore, the aim of this study was to determine the prevalence of PBS and to analyze its radiological characteristics.
Material and Methods
Patients and images
This retrospective study has been approved by the Institutional Ethics Committee.
Four patients with PBS were retrospectively identified in the pathological and radiological databases of the Martin-Luther-University Halle and 17 in the databases of four neighbouring hospitals in the time interval from 1997 to 2009 (search for key words in the reports). All 21 identified patients were women (Table 1), and their median age was 66 years (range 27–86 years).
Patient characteristics with primary breast sarcoma
In our institution 2896 patients with breast carcinoma were treated in the investigated time period. The number of the respective patient numbers of the neighbouring hospitals was not available.
Mammography was performed in 19 patients. Several dedicated mammographic units were used. Standard medio-lateral oblique and cranio-caudal mammograms were made with additional views if necessary. Supplementary ultrasound images were available in eight patients. In three patients magnetic resonance imaging (MRI) of the breast was performed additionally using a dedicated receive-only breast coil on a 1.0 T scanner (Impact Expert, Siemens, Erlangen, Germany).
All available images were interpreted by two radiologists (AS and KR with 7 and 11 years’ experience, respectively). Consensus of the investigators was obtained on the following features of the identified breast lesions: number, shape, localization, size, margin, attenuation, homogeneity, and contrast enhancement patterns.
All breast findings were classified according to the American College of Radiology Breast Imaging Reporting and Data Systems (BI-RADS) lexicon (8–10). Lesion size was determined by measuring the maximum diameter.
Case histories were reviewed retrospectively to determine clinical signs at presentation.
Histological findings
In all patients the diagnosis of PBS was confirmed histopathologically. Biopsy specimens were evaluated by one pathologist (HJH, 37 years experience). All available histological materials (sections stained by hematoxylin/eosin or by immunohistochemistry) were analyzed.
Statistics
For statistical analysis the SPSS statistical software package was used (SPSS 17.0, SPSS Inc., Chicago, IL, USA). Collected data were evaluated by means of descriptive statistics (absolute and relative frequencies).
Results
Prevalence, localization, and clinical signs
The prevalence of PBS in our institution (four patients) was 0.1% of all cases with breast malignancies. The left breast was involved in 10 patients (48%) and the right breast in 11 (52%). Clinically, all patients presented with solitary painless breast lumps. There was no uni- or bilateral axillary lymphadenopathy. Skin edema was seen in two patients (10%).
Radiological features
Mammographic findings
The following two mammographic patterns could be identified: breast masses and architectural distortion (Table 2).
Mammographic characteristic of PBS presenting as intramammary masses
Intramammary masses were the most common mammographic appearance of PBS (n = 13, 68%). Most of them were lobular or round in shape with microlobulated or indistinct margins (Fig. 1). The median size of the lesions was 25 mm (range 10–110 mm).
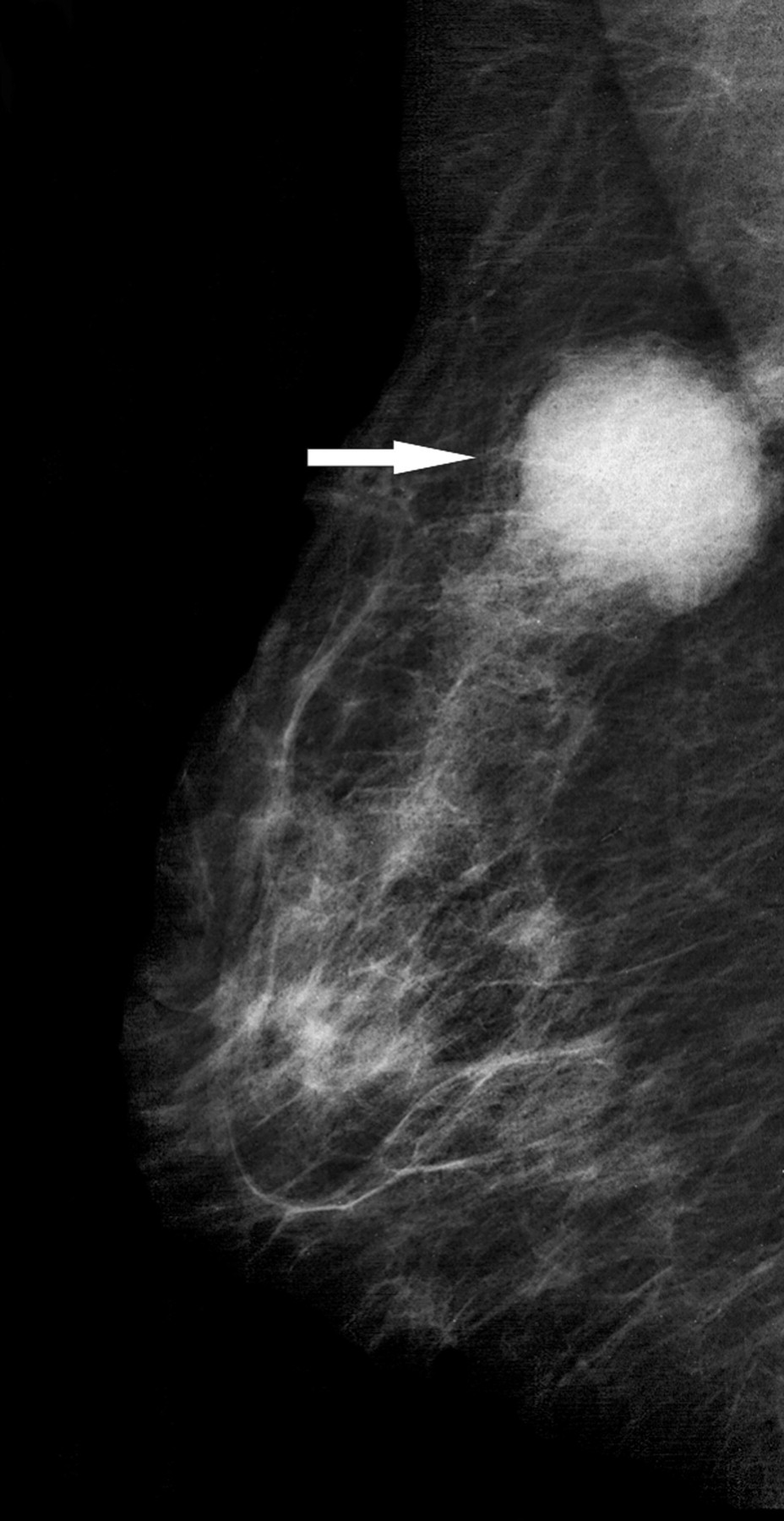
Radiological findings in a 66-year-old patient with primary angiosarcoma of the right breast. Medio-lateral oblique mammogramm of the right breast showing a round dense mass with microlobulated margins in the upper quadrant (arrow)
Architectural distortion occurred in six patients (32%). In three cases PBS manifested as diffuse density with architectural distortion and in three patients as isolated distortion (Fig. 2).

Radiological findings in a 59-year-old patient with fibrosarcoma of the breast. (a) Medio-lateral oblique mammogramm of the right breast after marker placement showing an architectural distortion (arrow) in the upper quadrant suspicious for a breast carcinoma. (b) Specimen radiograph after surgical resection of the lesion
Most mammographic findings were hyperdense. Micro- or macrocalcifications were present in three cases (16%). In one patient (5%) the mammographic findings were categorized as BI RADS 3, in seven (37%) as BI RADS 4, and in 11 (58%) as BI RADS 5.
Ultrasound findings
Ultrasound (US) images were available for eight patients. 5(63%) of the identified lesions were homogeneously hypoechoic, and in three (37%) cases heterogeneously mixed hypo- to hyperechoic (Fig. 3). Four (50%) intramammary masses were lobular, three (37%) oval, and one (13%) round in shape. Six (80%) lesions had microlobulated margins and two (20%) had indistinct margins. No posterior acoustic phenomenon was detected in four (50%) cases. Posterior acoustic enhancement was shown in four (50%) lesions. US findings were categorized as BI RADS 4 in five (63%) and BI RADS 5 in three cases (37%).
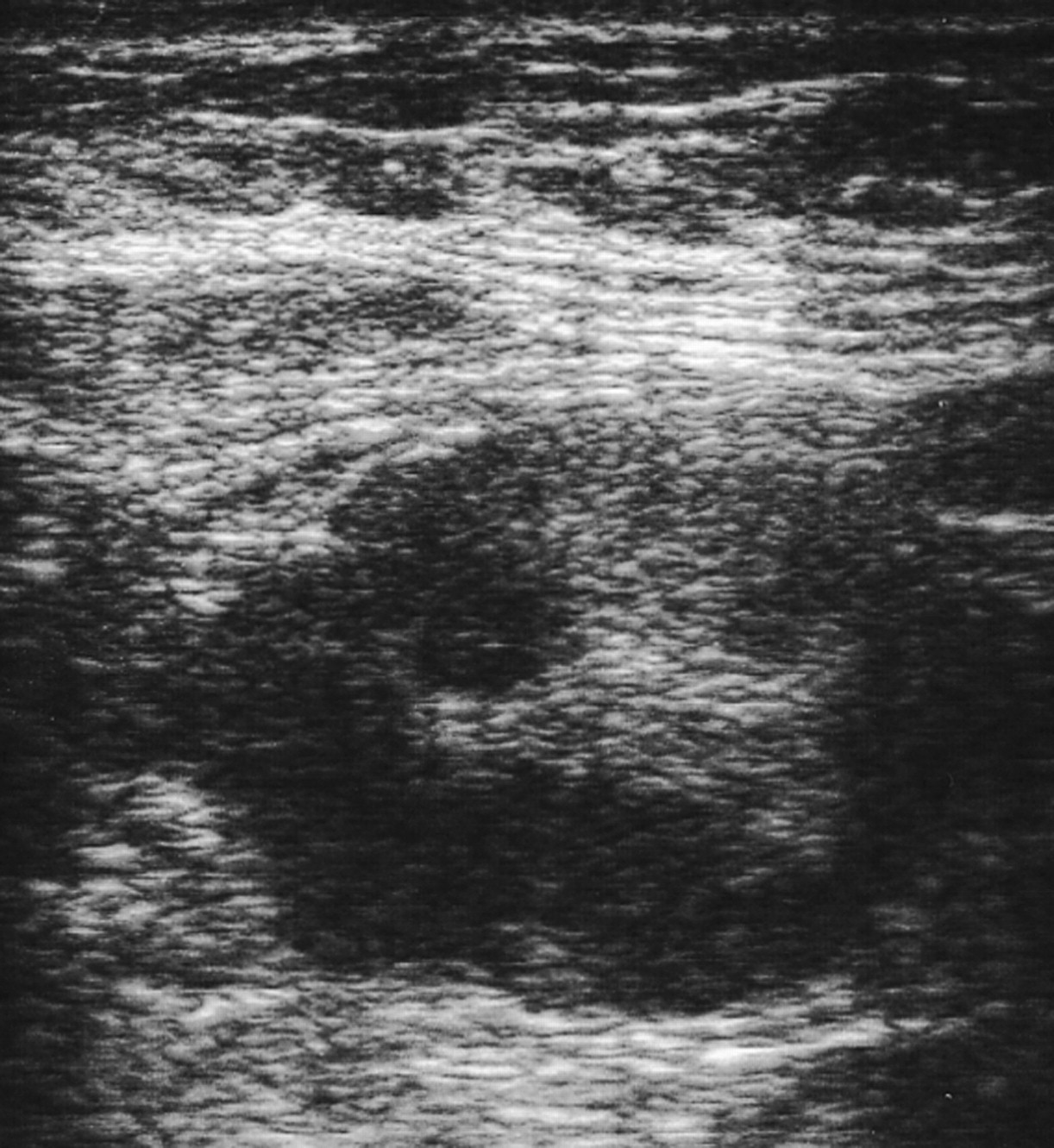
Ultrasound finding in a 57-year-old patient with spindle cell sarcoma of the left breast. The image shows an oval hypoechoic (but with heterogeneous contents) mass with microlobulated margins
MR findings
In three patients MRI was performed additionally. The identified lesions showed a minimally hyperintense signal compared with normal breast parenchyma on T2-weighted (T2W) images. They were hypointense in comparison to fat (Fig. 4). After intravenous administration of contrast medium a marked inhomogeneous contrast enhancement was seen in all cases. All MR findings were classified as BI RADS 5.
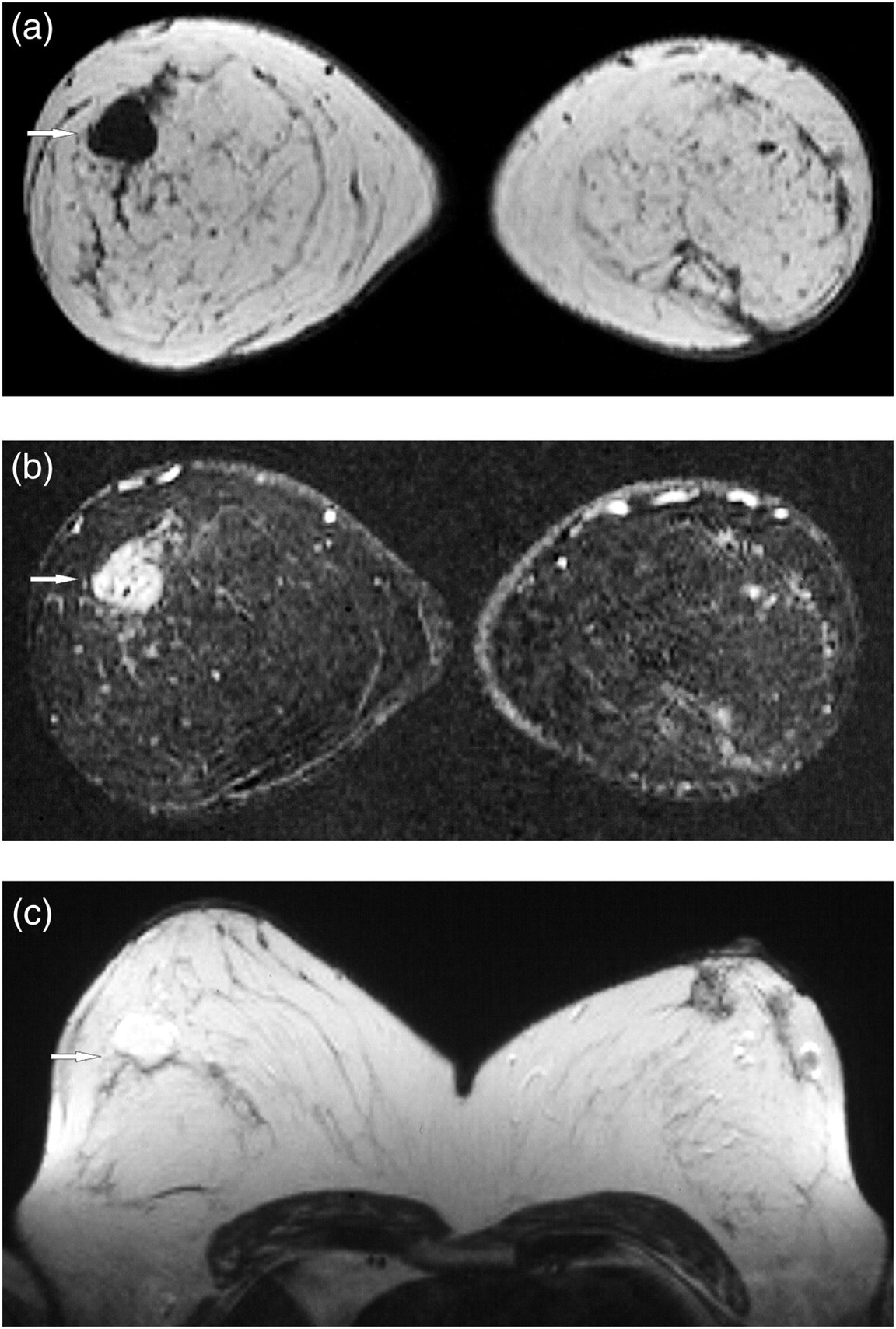
Magnetic resonance imaging of the breasts in a 27-year-old woman with primary angiosarcoma. (a) T1-weighted image before contrast administration confirmed an isointense mass in the right breast (arrow). (b) Subtracted images demonstrated marked inhomogeneous enhancement of the lesion (arrow). (c) On T2-weighted images the lesion is hyperintense (arrow)
Treatment and outcome
In all of the identified cases the diagnosis was proven histopathologically. US-guided biopsy was performed in all cases. Mastectomy was performed in 19 patients (90%). In one patient (5%) tumor resection was done. Local recurrence occurred in one patient here. In one case (5%) metastasized PBS was diagnosed and local radiation and chemotherapy was performed.
Discussion
The development of some sarcomas is a recognized complication of radiation therapy. Post-radiation breast sarcoma is not rare (11). Primary sarcoma of the breast, however, is an unusual diagnosis (2–4). According to the literature, the true prevalence of PBS is difficult to determine (12, 13). It varies from 0.5% to 3% of malignant tumors of the breast (14). In the study of Adem et al., however, it was 0.0006% (1).
In our institution the prevalence of PBS was 0.1% of cases with breast malignancies. Clinically and radiologically PBS show no specific signs.
Clinically, the most common presenting symptom was painless breast mass (1–4). Pain has been reported to occur in 7–21% of patients (1, 15, 16). However, in the study of Yang et al., 12% of breast sarcomas were clinically asymptomatic when identified incidentally on screening mammograms (15). In our series all patients presented with painless solitary breast lumps. No side predominance of PBS localization was seen. There was no bilateral involvement.
Radiological studies describe a relatively small number of the cases with PBS, ranging from five to 11 (14–16). Furthermore, most of them focus on angiosarcoma of the breast (15, 16). According to the literature, on mammography, most lesions are round or oval masses with a well-circumscribed margin (1). Typically, no masses had spiculated margins or calcifications (14–16). However, according to Liberman et al., calcification occurs in 10% of PBS (16). In 31% focal asymmetry was described as mammographic manifestations of breast sarcoma (15). In the series of Yang et al. 19% of patients with breast sarcoma, however, showed no abnormalities on mammography (15). In our study two mammographic patterns could be identified: breast masses and architectural distortion. Intramammary masses were the most common mammographic appearance of PBS (68%). Most of them were lobular or oval in shape with microlobulated or indistinct margins. In 16% of cases breast sarcoma presented on mammography as architectural distortion. This feature is typically seen in breast carcinoma and has not been described previously in PBS. Furthermore, 16% of PBS cases in our study manifested as diffuse density with architectural distortion. Interestingly, micro- or macrocalcifications were present in 16%.
On ultrasound, breast sarcoma manifests usually as hypoechoic round or oval lesions without posterior attenuation (15). Hyperechoic masses have been also described (15, 16). Concordant with previous reports, in our study most lesions were hypoechoic, lobular or oval in shape with microlobulated or indistinct margins.
MRI features of PBS have been reported only sporadically in the literature. According to the previous reports, breast sarcomas are heterogeneously hypointense on T1-weighted images and hyperintense on T2-weighted images with intense enhancement after administration of contrast medium (15). In our series with three tumors we identified similar findings. Type 2 kinetics with a rapid initial increase in signal intensity followed by a flattening of the enhancement curve were present in all cases (17).
Histologically, several PBS have been described in the literature (Table 3). In our study, most PBS were angiosarcomas and fibrosarcomas. However, other types of breast sarcoma, such as osteosarcoma, liposarcoma, chondrosarcoma, leiomyosarcoma, malignant histiocytoma, and Kaposi sarcoma have been also reported (18–21).
Classification of PBS of the breast*
*In accordance with the WHO classification
Treatment of PBS is the same as for sarcoma involving other locations and is based on radical surgery, chemotherapy and/or radiotherapy (1–4). In the study by Adem et al., tumor resection/enucleation was successfully performed in most cases (1). In the series by Yang et al., however, most patients underwent mastectomy (15). In our study, mastectomy was performed in 90% of the cases. In 5% tumor resection was done. Local recurrence occurred in one patient here. In 5% metastasized PBS was diagnosed and local radiation and chemotherapy was performed.
In conclusion, our study shows that the imaging findings of primary breast sarcoma are not pathognomonic and can mimic those of breast carcinoma. However, they should be taken into consideration in the differential diagnosis of breast lesions.