
Abstract
Background
Pulmonary aspergillosis in immunocompetent patients has been described as a saprophytic infection with pre-existing lung lesions showing an air-meniscus sign on chest radiograph or CT scans. There have been rare articles dealing with pulmonary aspergillosis in immunocompetent patients without pre-existing lung lesions.
Purpose
To evaluate the CT findings of pulmonary aspergillosis in immunocompetent patients without air-meniscus and underlying lung disease and to correlate the CT findings and pathologic features of pulmonary aspergillosis in these patients.
Material and Methods
A total of seven surgically proven pulmonary aspergillosis found in immunocompetent patients without an air-meniscus and underlying lung disease (M:F = 1:6; mean age 63.4 years) were included. On CT, the lesion shape, margin, type, location, diameter, presence of satellite nodules, presence of CT halo sign or hypodense sign, and interval growth were evaluated. Histopathologic features of each lesion were classified as one of the following; primary aspergilloma, chronic necrotizing pulmonary aspergillosis, or invasive pulmonary aspergillosis. Correlation between CT findings and pathological features was performed.
Results
All lesions presented as a nodule or mass unable to differentiate from malignancy. Most lesions had well-defined margins (n = 4), appeared as solid lesions (n = 7), and were located in the upper lobe (n = 5). Mean diameter of lesions was 2.3 cm. Satellite nodules (n = 2), CT halo sign (n = 1), and hypodense sign (n = 4) were found. Only one lesion increased in size during follow-up. Lesions were pathologically classified as primary aspergilloma (n = 3) and chronic necrotizing pulmonary aspergillosis (n = 4). The hypodense sign on CT was pathologically proved as dense fungal hyphae filled in bronchus and CT halo sign as parenchymal hemorrhage.
Conclusion
Pulmonary aspergillosis predominantly presented as a nodule or mass mimicking malignancy in the upper lobes on CT scan in elderly without underlying lung disease and immunosuppressive conditions except for age, and was histopathologically revealed to be either primary aspergilloma or chronic necrotizing pulmonary aspergillosis.
Pulmonary aspergillosis in immunocompetent patients, which has been described in previous articles, is a saprophytic infection in a pre-existing cavity or ectatic bronchus showing the typical air-meniscus sign on chest radiograph or chest CT scan (1–3). Pre-existing pulmonary lesions such as bronchiectasis, cavity, or bullae have been known to always accompany pulmonary aspergillosis in immunocompetent patients. However, Kang et al. reported another form of pulmonary aspergillosis in immunocompetent patients without pre-existing lung lesions which presented as a single nodule or mass with or without an air-meniscus sign or localized consolidation (4). These lesions could not be differentiated from malignant neoplasm or other chronic infections on chest radiograph or CT scans, especially in case of a nodule or mass without an air-meniscus sign. They found that all pulmonary aspergillosis were endobronchial saprophytic aspergillosis and there was no definite evidence of underlying bronchiectasis. They designated the lesions as primary noninvasive pulmonary aspergillosis, identical to primary aspergilloma. However, thereafter there have been only a few articles dealing with pulmonary aspergillosis in immunocompetent patients without pre-existing lung lesions and the question as to its existence remains unclear (5).
Therefore, the purpose of our study was to evaluate the CT findings of pulmonary aspergillosis without an air-meniscus sign in immunocompetent patients who did not have any underlying lung disease and to correlate the CT findings and pathologic features of pulmonary aspergillosis in these patients.
Material and Methods
Approval for this study was obtained from the Institutional Review Board of our institution and a waiver of informed consent was obtained. This study was supported by grant no 04-2008-0700 from the Seoul National University Hospital Research Fund.
Patients
Between January 2001 and February 2007, 161 pulmonary lesions were pathologically confirmed as pulmonary aspergillosis at Seoul National University Hospital. One board-certified chest radiologist with 10 years of experience in chest imaging (HJL) and one senior radiology resident (SHY) reviewed the chest CT scans, medical records, surgical records, and pathologic reports. Pulmonary aspergillosis in immunocompetent patients without underlying lung disease were selected using the following criteria: (a) lesions pathologically confirmed by surgical resection; (b) lesions without the presence of the air-meniscus sign on chest radiograph and CT scan; (c) lesions found in immunocompetent patients who did not have uncontrolled diabetes mellitus, alcoholism, or chronic debilitating diseases, steroid medication, HIV infection and hematologic diseases; (d) lesions found in patients whose CT scans showed normal lung parenchyma without having other underlying lung parenchymal diseases such as bronchiectasis, sequelae of pulmonary tuberculosis, or emphysema. Finally, a total of seven lesions from seven consecutive patients (mean age 63.4 years, age range 59–75 years, M:F= 1:6) were included in this study.
In these seven patients, respiratory symptoms at presentation were blood-tinged sputum (n = 4), hemoptysis (n = 2) and cough (n = 1). One patient also had low-grade fever. None of the patients were smokers. One patient (case 4) had well-controlled diabetes mellitus with oral antihypoglycemic therapy. On laboratory examinations, two patients had an elevation of absolute neutrophil count and C-reactive protein. Bronchoscopy was done in all patients and no abnormal findings were revealed by gross inspection or bronchoalveolar lavage. All patients had normal preoperative pulmonary function tests. One patient (case 4) underwent preoperative positron emission tomography (PET) scan. All patients were surgically treated by lobectomy. The clinical profiles of these patients are summarized in Table 1.
Clinical features of pulmonary aspergillosis in immunocompetent patients without underlying lung diseases
Image acquisition
The mean interval between last CT imaging and pathological confirmation was 16.0 days (range 6 ∼ 23 days). In all individuals, scanning was performed at end inspiration following hyperventilation. CT imaging was performed with one of four scanners (Genesis Hispeed and LightSpeed Ultra; GE Healthcare, Milwaukee, WI, USA; Somatom Plus-4 and Sensation-16; Siemens Medical Systems, Erlangen, Germany). Scanning parameters were as follows: detector collimation 5.0–8.0 mm; beam pitch 1.0-2.0; reconstruction thickness 1.0–2.5 mm; reconstruction interval 5.0-8.0 mm; rotation time 0.5–1.0 s; tube voltage 120 kVp; tube current 150–200 mA, and reconstruction kernel, high frequency algorithm. Contrast-enhanced chest CT was performed using a total of 70–90 mL of a non-ionic contrast material, iopromide (Ultravist 370; Bayer Schering Pharma, Berlin, Germany) at a rate of 3.0–4.0 mL/s using a power injector.
CT analysis
One board-certified chest radiologist (HJL) and one radiology resident (SHY) reviewed the chest CT scans in consensus. Both mediastinal (width 400 HU; level 50HU) and lung (width 1500 HU; level –700HU) window settings were evaluated. The shape of the lesion was categorized into nodule (<3 cm) or mass (≥3 cm), consolidation, or linear opacity. The margin was classified into well-defined versus irregular margin. The presence of satellite nodules was evaluated. The size of the lesions was evaluated as the longest dimension on axial CT scans. When the lesion appeared as a nodule or mass, they were classified as solid, mixed, or pure ground-glass nodule types. A solid nodule was defined as a nodule that completely obscures the entire lung parenchyma within it whereas a ground-glass nodule does not. Ground-glass nodules can be further classified as either a mixed ground-glass nodule (in the case of a nodule with patches of parenchyma that are completely obscured) or a pure ground-glass nodule (in the case of a nodule with no such areas). The presence of CT halo sign and hypodense sign were also evaluated. The CT halo sign was defined as an area of ground-glass opacity (GGO) surrounding a nodule (6). The hypodense sign was defined as central low attenuation in the lesion on contrast-enhanced CT (7). The location of the lesions was evaluated. The interval change during the follow-up period was also evaluated in each patient.
Pathologic analysis and radiologic-pathologic correlation
In seven lesions obtained at lobectomy, the specimens were stained with hematoxylin and eosin as well as periodic acid and Gomori methenamine silver. The main location of pulmonary aspergillosis was classified into either bronchial tree or lung parenchyma location. The presence of parenchymal or vascular invasion by fungal hyphae, necrosis, and granulomatous inflammation were also analyzed. Next, the histopathologic feature of each lesion was classified as one of the following as described in earlier articles (4, 8, 9); primary aspergilloma, chronic necrotizing pulmonary aspergillosis, or invasive pulmonary aspergillosis. Acid-fast stains were used to exclude the possibility of pulmonary tuberculosis. Correlation between CT findings and pathological findings was performed.
Results
CT findings
CT findings of each nodule are summarized in Table 2. All lesions presented as a nodule or mass unable to be differentiated from malignancy by CT. The margin of the lesions was well-defined in four and irregular in three lesions. Two lesions were accompanied with small satellite nodules. The mean diameter of the lesions was 2.3 cm and ranged from 1.4 cm to 3.1 cm. All lesions were solid. The CT halo sign was noted in one lesion and the hypodense sign was found in four lesions. Three lesions were located in the right upper lobe, two in the left upper lobe and two in the right lower lobe. The mean preoperative follow-up period was 2.5 months (1–9 months). Among them, one lesion showed interval growth during the nine-month follow-up period from 1.7 cm to 2.7 cm in diameter. PET scan showed a maximum standardized uptake value (SUV) of the lesion of 3.4 in case 4.
CT findings of pulmonary aspergillosis in immunocompetent patients without underlying lung diseases
Pathologic findings and radiologic-pathologic correlation
None of the patients had complications related to the surgical procedures. During the postoperative follow-up period (mean follow-up 23.0 months; follow-up range 4–57 months), all had been free of disease. The pathological findings are summarized in Table 3. The main location was the bronchial tree in six lesions and lung parenchyma in one lesion. Parenchymal invasion was found in four lesions, vascular invasion was not found in any lesion. Intralesional necrosis was found in one lesion and granulomatous inflammation in three lesions. Three lesions were classified as primary aspergilloma because no vascular or parenchymal invasion and no underlying lung disease could be found. Four lesions were categorized as chronic necrotizing pulmonary aspergillosis.
Pathologic findings of pulmonary aspergillosis in immunocompetent patients without underlying lung diseases
In three primary aspergillomas, the hypodense sign was noted in two lesions by CT. The hypodense sign was pathologically proven to represent dense fungal hyphae filled in the bronchial tree. Two lesions confirmed as primary aspergilloma had irregular margins and one had a well-defined margin. The irregular margin in two lesions was due to prominent chronic inflammatory cell infiltration. (Fig. 1)
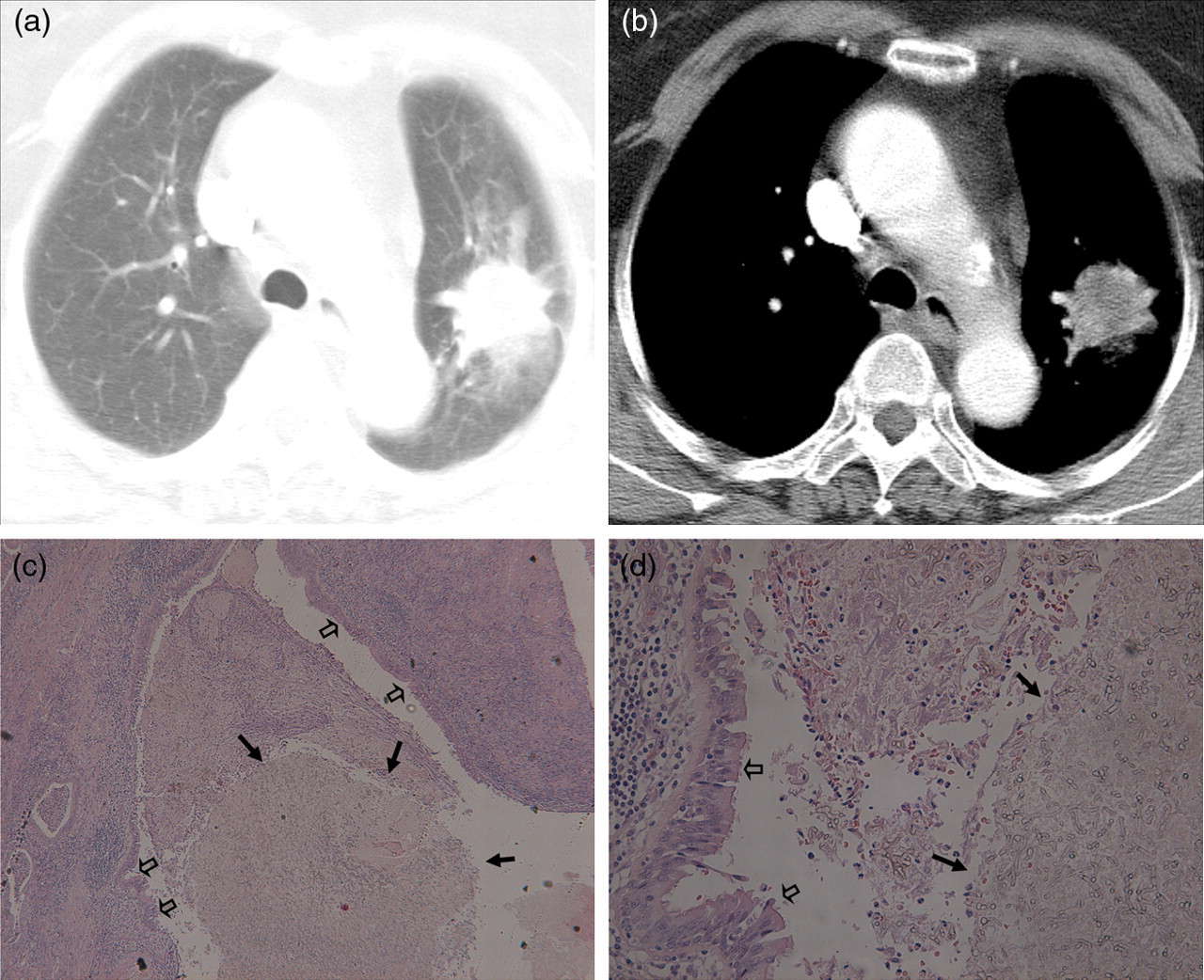
Axial CT image of the chest of a 75-year-old woman presented with blood-tinged sputum. The mass was confirmed as primary aspergilloma. (a) Lung window setting of chest CT scan shows a 3.1 cm solid mass with irregular margin in the left upper lobe. (b) Mediastinal window setting shows a central low attenuation suggesting the hypodense sign in the mass. (c) Photomicrograph of the surgical specimen shows a mass-like collection of fungal hyphae (arrows). The lining bronchial epithelium is seen (open arrows) (H & E, ×40). (d) Photomicrograph shows an intrabronchial collection of fungal hyphae (arrows) and the lining bronchial epithelium (open arrows) are seen (H & E, ×400). In this lesion, parenchymal or vascular invasion of fungal hyphae was not found
In four cases with chronic necrotizing pulmonary aspergillosis, the hypodense sign was noted in two lesions and the CT halo sign in one lesion. The hypodense sign in two cases with chronic necrotizing pulmonary aspergillosis also proved to be dense fungal hyphae filled in the bronchial tree. CT halo sign was pathologically proven to represent parenchymal hemorrhage. Three lesions had well-defined margins and one had an irregular margin. The irregular margin in one lesion was due to parenchymal invasion of aspergillus and granulomatous inflammation surrounding the bronchial tree (Fig. 2). The well-defined margin in three lesions was due to minimal microscopic parenchymal invasion.
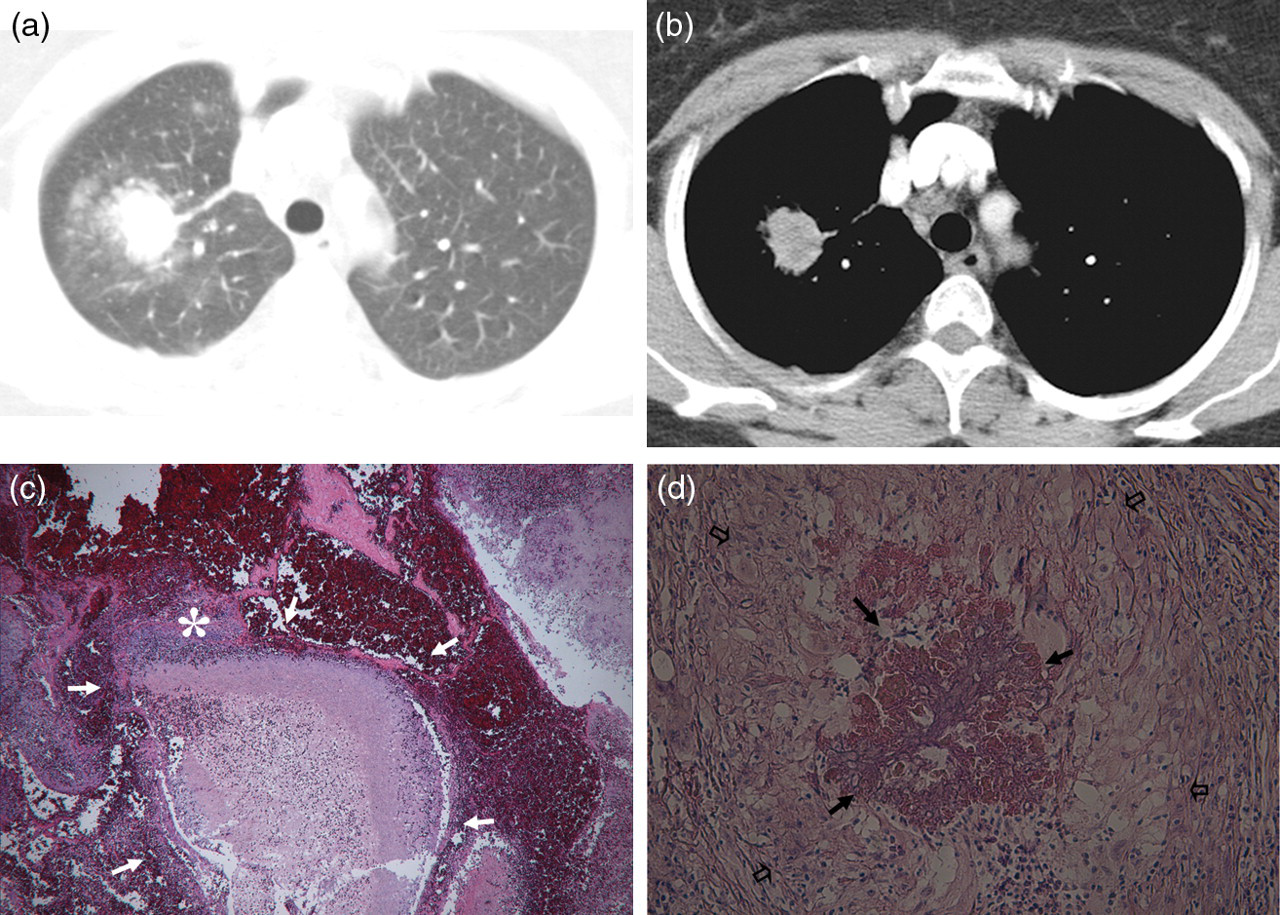
Axial CT image of the chest of a 59-year-old woman presented with blood-tinged sputum. The nodule was confirmed as chronic necrotizing pulmonary aspergillosis. (a) Lung window setting of chest CT scan shows a 2.7 cm solid nodule with irregular margin and the CT halo sign in the right upper lobe. (b) Mediastinal window setting shows the hypodense sign. (c) Photomicrograph of the specimen shows a collection of fungal hyphae in the bronchial tree (arrows) that invades into the surrounding lung parenchyma (asterisk) (H & E, ×100). (d) Photomicrograph of the specimen shows granulomatous inflammation in the surrounding lung parenchyma (open arrows) and a collection of fungal hyphae (arrows)(H & E, ×200)
Discussion
The main findings obtained in this study were as follows: (a) all pulmonary aspergillosis in immunocompetent patients without an air-meniscus and underlying lung disease were shown on CT as a nodule or mass in elderly without immunosuppressive conditions except for age; (b) among seven lesions in which CT-pathologic correlation was performed, three were pathologically proven primary aspergilloma and four were chronic necrotizing pulmonary aspergillosis. The nodular appearance of pulmonary aspergillosis without an air-meniscus sign has been reported not only in immunocompetent patients without underlying lung disease (4, 10) but also in mildly immunosuppressed patients with underlying chronic lung diseases (9, 11–15). The possible etiologies of nodular pulmonary aspergillosis include chronic necrotizing pulmonary aspergillosis, primary aspergilloma, and sequelae of invasive pulmonary aspergillosis. In case of primary aspergilloma, it is suggested that primary aspergilloma may arise from implantation of fungus in a normal bronchus followed by gradual dilatation of bronchus by the pressure of its growing colony (10).
In contrast to the saprophytic aspergillosis in immunocompetent patients accompanied by an air-meniscus sign which enables to distinguish from malignancy, most pulmonary aspergillosis in this study were shown as a non-specific solid nodule or mass on CT scans. Not only a specific diagnosis of pulmonary aspergillosis but also differentiation from malignancy was radiologically impossible, especially considering the old age of patients, the size of pulmonary aspergillosis being 3 cm or more in two patients and the maximum SUV being 3.4 on PET scan in one patient. Therefore the pathologic evaluation by obtaining specimen using percutaneous lung biopsy is essential for the differentiation between this unique pulmonary aspergillosis and lung cancer.
However, even when the lesions are confirmed as pulmonary aspergillosis by percutaneous core biopsy, differentiation between primary aspergilloma and chronic necrotizing pulmonary aspergillosis might still prove to be difficult. Considering that anti-fungal treatment is usually needed in chronic necrotizing pulmonary aspergillosis (3), it could be important to differentiate chronic necrotizing pulmonary aspergillosis from primary aspergilloma in case of biopsy proven nodular pulmonary aspergillosis.
Among the four patients found to have chronic necrotizing pulmonary aspergillosis in this study, no patients had an underlying immunocompromised disease except for age which is quite contrary to previous reports (12–15). There are also very few reports that have described the presence of fever or laboratory findings of chronic necrotizing pulmonary aspergillosis in immunocompetent patients without underlying lung disease (4). In our study, two patients with chronic necrotizing pulmonary aspergillosis showed mild fever and a minimal increase of absolute neutrophil count. The remaining two patients with chronic necrotizing pulmonary aspergillosis and three patients with primary aspergilloma did not show any clinical sign of infection such as fever, leukocytosis, or elevated C-reactive protein.
The hypodense and CT halo signs are radiologic findings suggestive of invasiveness of pulmonary aspergillosis (6, 7). The hypodense sign in invasive pulmonary aspergillosis of immunocompromised patients has been reported as pulmonary infarctions or coagulation necrosis on pathologic examination. According to previous articles (7), the hypodense sign found in invasive pulmonary aspergillosis has been an indicator of good prognosis, which appear prior to cavitation. On the other hand, the hypodense sign found in this study was pathologically proven as intracavitary massive fungal hyphae without pulmonary infarction or coagulation necrosis. Moreover, our study revealed that the hypodense sign in pulmonary aspergillosis in immunocompetent patients without underlying lung disease could be found in primary aspergilloma or chronic necrotizing aspergillosis. Therefore, in pulmonary aspergillosis in immunocompetent patients, the hypodense sign on CT might not have any clinical significance. The CT halo sign in our immunocompetent patients was pathologically proven as hemorrhage similar to the invasive pulmonary aspergillosis (6).
The main limitation of this study was that small number of cases and selection bias may have been present due to the retrospective collection of data.
In conclusion, pulmonary aspergillosis predominantly presented as a nodule or mass in the upper lobes on CT scan in elderly patients without underlying lung disease and immunosuppressive conditions except for age and was histopathologically revealed to be either primary aspergilloma or chronic necrotizing pulmonary aspergillosis. The presence of CT halo sign and clinic-laboratory signs of infection including fever, elevated absolute neutrophil count or C-reactive protein can help to differentiate chronic necrotizing pulmonary aspergillosis from primary aspergilloma.
Footnotes
Acknowledgements
This study was supported by grant no 04-2008-0700 from the SNUH Research Fund.