
Abstract
Abdominal wall endometriosis is unusual and mostly occurs in scars following Cesarean section. Although malignant transformation is rare, it must be recognized in order to benefit from radical resection. We report a very rare case of mixed endometrioid and serous carcinoma developing in a Cesarean section endometriosis scar and the way we managed it using surgery and chemotherapy. 18-FDG PET-CT imaging was performed to correctly stage the disease.
Pelvic endometriosis is defined by the presence of aberrant endometrial glands and stroma outside the uterine cavity. Abdominal wall endometriosis is a well-established entity as it represents 1–2% of all endometriosis lesions (1). It usually arises on a surgical scar following Cesarean section or hysterectomy and less frequently on a surgical scar following hernia repair or appendectomy (2, 3). Malignant transformation in endometriosis is a rare event occurring in less than 1% of cases, mostly at ovarian sites and extragonadal malignant transformation represents 21.3% of these cases (4). Malignant transformation of abdominal wall endometriosis had already been described in literature (5–7) and mostly includes clear-cell carcinoma followed by endometrioid carcinoma. To the best of our knowledge, this is the first reported case of mixed endometrioid and serous adenocarcinoma arising in parietal endometriosis following Cesarean section.
Case report
A 48-year-old woman presented with a rapidly growing, large and painful mass in the abdominal wall muscles. Her past obstetric history included two Cesarean sections 16 and 20 years ago. She had no treatment except the use of an intrauterine contraceptive device. Physical examination revealed a 6 cm parietal mass on the left side of the Cesarean scar. Despite the absence of known pelvic endometriosis, abdominal wall endometriosis on the Cesarean scar was suspected. A magnetic resonance imaging (MRI) was performed and confirmed a 6 cm, cystic and solid tumor developed on the left side of the Pfannenstiel incision, located in the left rectus abdominis muscle. The lesion was T1-isointense and the cystic component of the lesion presented with moderate hyperintensity on T2-weighted (T2W) images (Fig. 1a) and persistent high signal intensity on fat-suppressed T1-weighted MRI due to hemorrhage (Fig. 1b). Imaging findings were consistent with parietal endometriosis. There were no other MRI signs of pelvic or extrapelvic endometriosis.
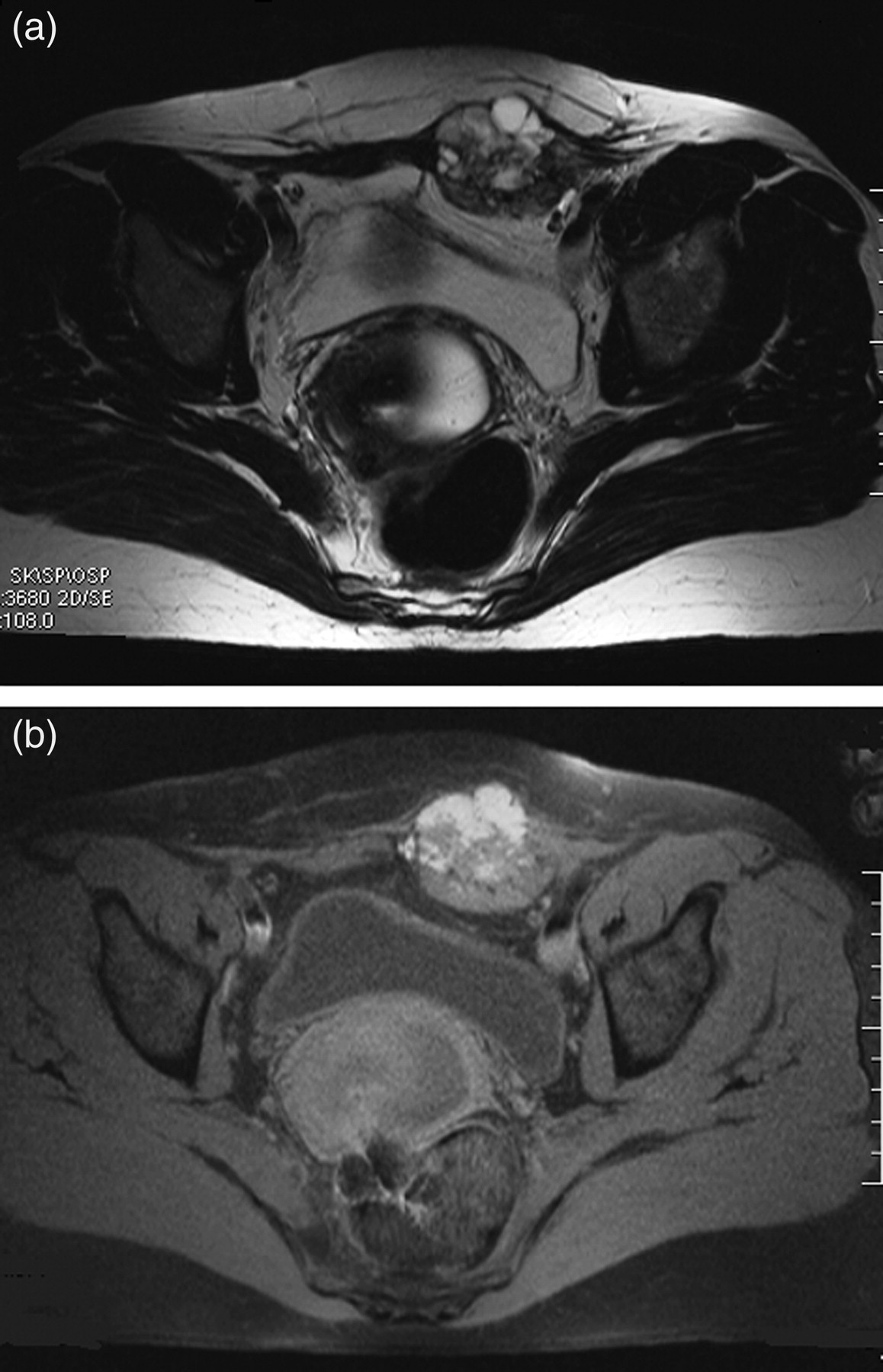
Abdominal wall endometriosis in a 48-year-old woman with a past obstetric history of two Cesarean sections 16 and 20 years ago. Axial T2-weighted (a) and fat-suppressed T1-weighted (b) MRI images show a mixed solid and cystic tumor located in the rectus abdominis muscle, developed on the left side of the Pfannenstiel incision. The cystic component of the lesion is characterized by T2W and T1W hyperintensity due to hemorrhagic foci suggesting endometriosis of the abdominal wall
During surgery, the first findings were a large and suspicious mass on the left side of the abdominal wall, adhering to the fascia (Fig. 2). A wide surgical excision with clear margins and abdominal wall reconstruction using a prosthetic mesh was performed.
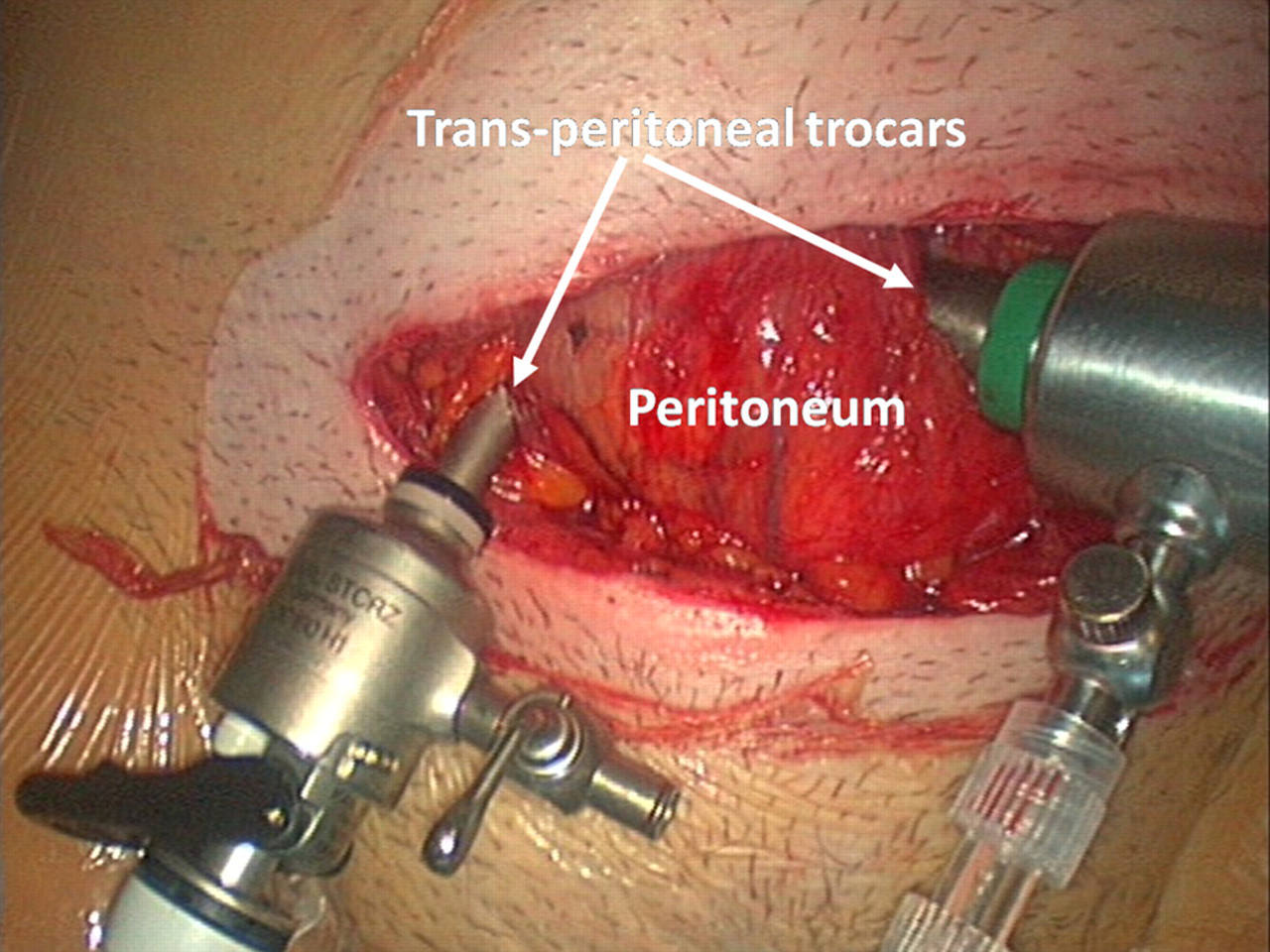
Perioperative photograph showing a 6 x 5 cm parietal mass
Intraoperative frozen section showed a malignant tumor of an ovarian or endometrial origin. Our patient was then surgically staged and laparoscopy was conducted just through the peritoneum. The abdominopelvic cavity was carefully examined and no lesions were found on the peritoneum, ovaries, uterus, mesentery, or small bowel. Hysteroscopy and curettage of the endometrium took place before the wall closure in order to exclude primary endometrial carcinoma.
Gross histopathological examination revealed a 6 × 5.5 × 4.5 cm nodular lesion with cystic, hemorrhagic, edematous, fibrous, and necrotic changes. Microscopic examination showed tumoral proliferation with irregular glands lined by cylindrical epithelium with nuclear pseudostratification, anisocytosis, anisokaryosis, and frequent mitoses. Tumoral stroma was fibrous with edematous changes and inflammatory infiltrate. Benign endometriosis was present on the periphery of the tumor (Fig. 3). Immunohistochemical study showed that tumor cells expressed cytokeratin 7 and sometimes vimentin. Cytokeratin 20 was not expressed. The CD10 marker (cytogenic chorion) was positive, strongly supporting the malignant transformation of endometriosis. A diagnosis of mixed endometrioid and serous carcinoma developed in a Cesarean section endometriosis scar was finally made.

Histology section shows endometriosis lesions in the abdominal wall with dilated endometrial glands (*) surrounded by cytogenic chorion and endometrioid adenocarcinoma (arrow) (hematoxylin and eosin stain x4)
Routine laboratory findings and tumor markers (CA125, CA15-3, CA19-9, CEA and NSE) were normal. A whole-body positron emission tomography with computed tomography using 18-fluorodeoxyglucose (18-FDG PET-CT) procedure was performed for disease staging 25 days after surgery and showed a suspicious hypermetabolic right adnexal lesion and two hypermetabolic left iliac nodes which were missed both during surgical exploration and on preoperative pelvic MRI (Fig. 4). Standard uptake values (SUV) of those lesions were superior to 6. The multidisciplinary oncology team meeting proposed first a surgical exploration with histological analysis of left external iliac lymph nodes. Conclusion of the pathologist was involvement of the two iliac lymph nodes by subcapsular micro-metastasis. The multidisciplinary oncology meeting proposed complementary chemotherapy. Our patient underwent six courses of chemotherapy (Taxol® and Carboplatine®). 18-FDG PET-CT was then performed after three chemotherapy courses and showed good response, with significant decrease of all SUV values. Post-treatment imaging showed disappearance of all hypermetabolic lesions. A laparoscopic hysterectomy with bilateral salpingo-oophorectomy and installation of abdominal wall prosthesis was decided. On definitive histopathological examination there was no residual carcinoma in the uterus and adnexa. Our patient presented no sign of recurrence 15 month after the initial diagnosis.
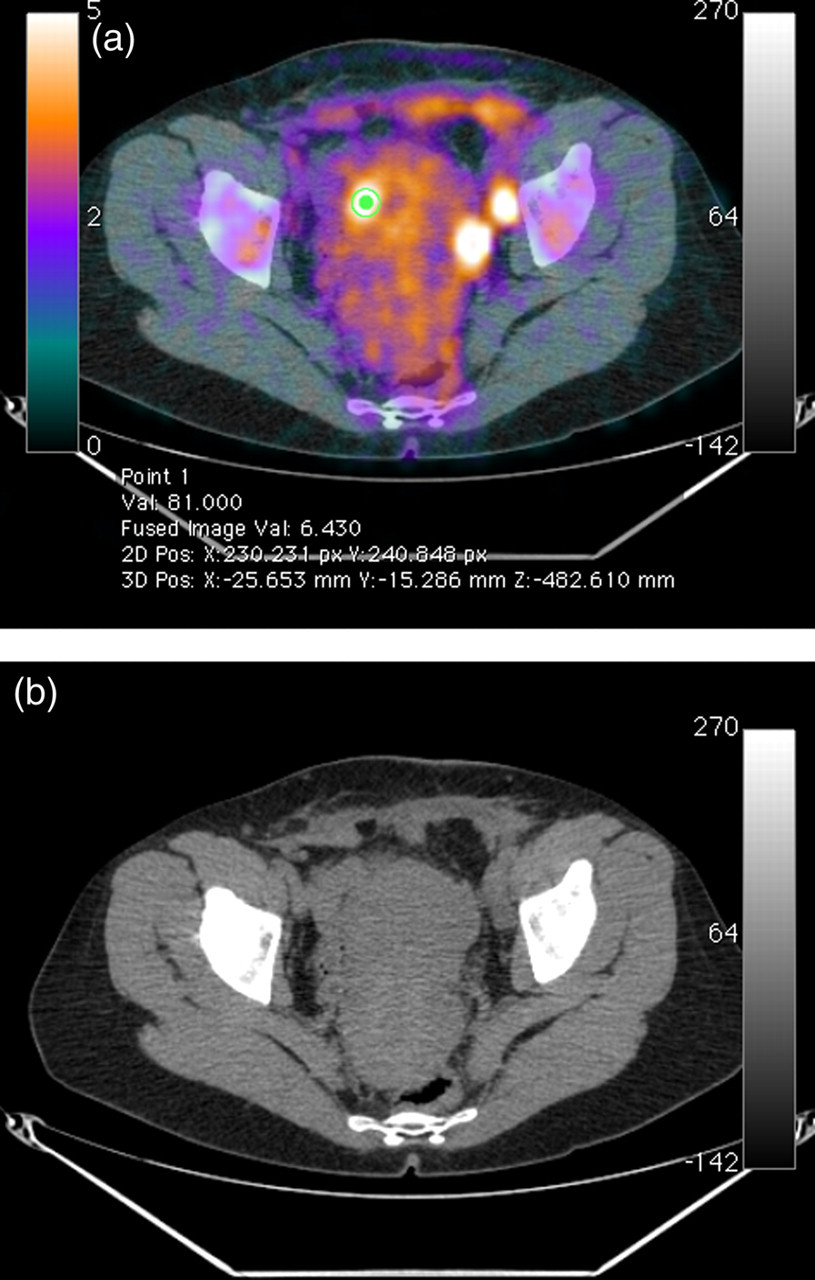
18-FDG PET-CT with the fused images (a) and the coregistered CT (b) shows a right adnexal lesion and two left external iliac lymph nodes with intense uptake indicative of active and residual malignant disease. The SUV were above 6
Discussion
The first case of malignant transformation of endometriosis was described by Sampson in 1925 (8), who proposed three criteria for diagnosis: demonstration of both neoplastic and benign endometrial tissue in the tumor, histological type of tumor compatible with endometrial origin, and no other primary site identified. It may be difficult to determine whether the tumor developed from endometriotic lesions, as some tumors may destroy the tissue of origin, and as tumor and endometriosis lesions may co-exist. A fourth criterion was proposed by Scott (9), who adds the concept of transition between histological benign endometriosis and carcinoma, but this idea still is subject for discussion. Malignant transformation of extragonadal endometriosis is endometrioid carcinoma in 69.1%, sarcoma in 25%, clear cell carcinomas in 4.5% and other in 4.6% of cases (4). A review of the literature (10) indicates that malignant abdominal wall endometriosis concerns mostly clear cell and endometrioid carcinoma. The differential diagnosis of tumors occurring in endometriosis includes endometrioid peritoneal tumors (malignant, benign or borderline), endometrial sarcoma, malignant mixed tumors, and adenosarcoma. In our case, a transition zone as defined by Sampson (8) allowed diagnosis of malignant transformation of parietal endometriosis. Above all, CD10, which is a reliable and sensitive (88%) immunohistochemical marker of endometrial stroma (11), was expressed on few cells of the cytogenic chorion, strongly supporting the diagnosis.
The delay between benign endometriosis and malignant transformation varies from 3 to 39 years with an average of 17 years (12), which is similar to our case. Clinically, the diagnosis of malignancy is extremely difficult and should be suspected in patients with a history of recurrent scar endometriosis and absence of improvement with medical treatment, especially when the mass shows rapid growth (13), as in our patient.
There is no specific marker of malignant degeneration, and CA 125 is frequently normal. MRI is useful to define the limits of the lesion. 18-FDG PET-CT enables disease staging and thus optimizes treatment. In our case, chemotherapy and laparoscopic hysterectomy with bilateral salpingo-oophorectomy were performed on the basis of 18-FDG PET-CT findings in order to treat active and residual disease.
Due to its rarity, there is no standardized approach for treatment. Primary surgical treatment remains the gold standard and as far as possible included a wide and complete excision with healthy margins to prevent tumor recurrences that occur in 0–15% of cases during the first year (14). Complementary radiotherapy (15) combined with progestin therapy is frequently used. The effectiveness of chemotherapy based on salts of platinum used in metastatic forms is uncertain. Miller (15) established some good prognosis factors: age below 60 years, small-sized tumor, well-differentiated and non-metastatic tumor, early resection of endometriotic lesions, and endometrioid carcinoma as histological type.
In conclusion, malignant transformation of abdominal wall endometriosis is a very rare complication but should be considered when faced with any scar lesion evolving with rapid growth, thus requiring surgical resection with oncological principles and histopathological examination. Radical surgery is the main treatment and chemotherapy can be added if there is still any doubt about extrapelvic metastasis. In our case, we used 18-FDG PET-CT as a staging tool and to evaluate response to treatment. This clinical observation is all the more important due to the increasing number of Cesarean sections performed nowadays.