
Abstract
Background
Morphology microcalcification descriptors help stratify the risk of breast malignancy. Micro CT is feasible for visualization of the fine-structure of tissues and may be suitible for high resolution microcalcification analysis.
Purpose
To analyze the interior structure of microcalcifications using a micro CT imaging system.
Material and Methods
Core needle breast biopsy specimens from 16 women with clustered microcalcifications were examined with micro CT. The samples measured between 0.8 to 1.2 mm in diameter. Micro CT scans with an isotropic voxel size of 8.4 µm were obtained to generate two- and three-dimensional images of the microcalcifications. The number of microcalcifications were counted on the magnified specimen radiogram and on micro CT. Attenuation values of microcalcifications were measured by drawing a region of interest (ROI) in the center of the microcalcifications. Two blinded observers assessed the morphology and the interior structure of microcalcifications.
Results
Five patients had benign and 11 patients had malignant breast lesions. On micro CT, microcalcifications of benign tissue showed a coarse lamellar or trabecular interior structure, whereas microcalcifications of breast cancer tissue showed a more uniform granular interior structure. There was no correlation between attenuation values of benign compared with malignant microcalcifications.
Conclusion
On micro CT, an interior structure of microcalcifications is detectable. Benign and malignant microcalcifications display different patterns of interior structure.
Micro-computed tomography (micro CT) is a non-invasive high resolution imaging method applied in industry and biomedical science. Micro CT is increasingly used as an in vitro and in vivo tomographic method to examine tissue specimens and small laboratory animals at micrometer resolution (1, 2). In medicine, micro CT has been predominantly employed to analyze bone architecture and, with lesser frequency, soft tissue of various organs (3, 4). Zarsi et al. scanned calcium oxalate monohydrate renal calculi with micro CT and found that it is stone morphology and interior structure, rather than apparent X-ray attenuation, which correlates with lithotripsy fragility (5). There are only a few initial reports in the literature dealing with breast tissue analysis and microcalcification imaging with micro CT. However, the interior structure of microcalcifications has not been analyzed in these studies (6, 7).
The purpose of this study was therefore to evaluate the feasibility of micro CT to assess the interior structure of microcalcifications in vacuum-assisted core biopsy specimens of benign and malignant breast lesions.
Material and Methods
Vacuum-assisted stereotactic core biopsy specimens from 16 women (range 44–78 years, mean 59.4 years) were analyzed with micro CT. From each patient, informed consent was obtained to use one specimen containing microcalcifications for micro CT examination prior to histological work-up. Approval for use of biopsy specimens was given by the heads of pathology, radiology, and gynecology of the university clinic, in accordance with the requirements of the State Ministry of Science and Arts of the country.
The breast tissue samples were scanned with an X-ray microfocus computed tomograph (SkyScan 1072; Aartselaar, Belgium). The technical details of this system are described in detail elsewhere (4). In summary, the equipment consists of an X-ray microfocus tube, a moveable specimen stage, and a detector system. The tungsten microfocus X-ray tube (Hamamatsu Photonics, Toyooka-village, Japan) has a source voltage of 20–80 kV, a current of up to 100 µA, and a minimum spot size of 8 µm at 8 W. X-rays are produced in a cone-beam geometric formation. The sample holder is positioned between the X-ray source and the detector, the distances between them determining the magnification. The detection system consists of a scintillator screen, fibre optics, and a charge-coupled device (CCD) sensor. The P43 gadolinium oxysulphide phosphor scintillator has a thickness of 25 µm. Optical coupling of the scintillator screen with the CCD sensor, is a tapered fibre optics with a reduction of 3.7:1. The high-resolution 12-bit CCD sensor has a dimension of 6.76 mm2 and 1024 x 1024 pixels.
The biopsy samples were first packed into paraffin foliage for stabilization then positioned on the computer-controlled rotation stage. The specimens were rotated at minimum angular increments of 0.45° and scanned 180° around the vertical axis which corresponds to 400 projections. Sixty kV and 100 µA with 2.75 s of exposure time for each rotation step were used. The voxel size was 8.4 µm. Three-dimensional images were reconstructed using a modified Feldkamp's filtered back projection algorithm.
Analysis of microcalcifications
Analysis of micro CT data was carried out using the commercially available software package Analysis version 5.0 (Biomedical Imaging Resource, Mayo Foundation, Rochester, MN, USA), and the 3D-Calculator (Skyscan, Aartselaar, Belgium). These packages provide tools to display and analyze reconstructed volume images. We used volume-rendering techniques, maximum intensity projections, multiplanar reformations to display the structure and spatial arrangement of the microcalcifications, and region-of-interest based attenuation measurements.
Microcalcifications were categorized on the X-ray mammograms using the Breast Imaging Reporting and Data System (BI-RADS) lexicon of the American College of Radiology. The number of microcalcifications was counted on the magnified specimen radiogram and on micro CT. The length (mm) of microcalcifications and the attenuation values (by drawing regions of interest [ROIs] in the center of a microcalcification) were measured on micro CT images. The interior structure (free description by each reader) and the border characteristics (sharp or blurred) of microcalcifications were assessed by two blinded observers. If there was disagreement between the two readers, decision was obtained by consensus
Statistical analysis
The unpaired t test was applied to test the significance of differences (level of significance, P < 0.05) between the length and attenuation values of benign versus malignant microcalcifications. Fisher's exact test was used to calculate differences between the descriptors structure and border for benign and malignant microcalcifications.
Results
The patients’ characteristics, histological diagnoses, and microcalcification category according to the BI-RADS are summarized in Table 1. The patients’ breast microcalcifications were classified as highly suspicious (BI-RADS IV) (n = 11) or typically benign (BI-RADS II) (n = 5). The breast tissue specimens measured from 0.5 to 1.3 cm in length, while the diameters ranged between 0.8 and 1.2 mm.
Summary of the histological findings of breast core needle biopsies from 16 patients, pre-interventional mammography-based microcalcification classification (BI-RADS), number of microcalcifications in the specimen radiogram, interior structure of microcalcification on micro CT, and number of microcalcifications detected with micro CT
*Additional mass lesion
If micro CT images were generated with a soft tissue reconstruction algorithm, all benign and malignant microcalcifications appeared uniformly dense without any interior structure detectable. Using a sharp bone reconstruction algorithm, however, an internal structure could be seen in most of the microcalcifications. Four different patterns of internal structure were found in microcalcifications: trabecular, lamellar, granulous, and amorphous (i.e. no interior structure). Coarse trabeculation or lamellation was found inside of microcalcifications in four of the five specimens with benign lesions (Fig. 1a–d). Microcalcifications of the fifth biopsy specimen showed no interior structure (Fig. 1d). This sample was from a patient who had undergone lumpectomy from the same area one year ago (histological diagnosis at that time was invasive ductal carcinoma). The current histological specimen showed scarring tissue and fatty tissue necrosis. Microcalcifications of malignant lesions showed a fine granular interior structure if the calcifications exceeded 0.2 mm in diameter (Fig. 2a–d). The interior structure was best observed on thin source images and on thin MPRs (multiplanar reformation) followed by thin slab MIPs (maximal intensity projection). VRT (volume rendering technique), SSD (shaded surface display), and ray-sum projections (i.e. thick MPR) images were not helpful in showing the interior structure of microcalcifications but demonstrated the spatial arrangement of microcalcification cluster (Fig. 2c).
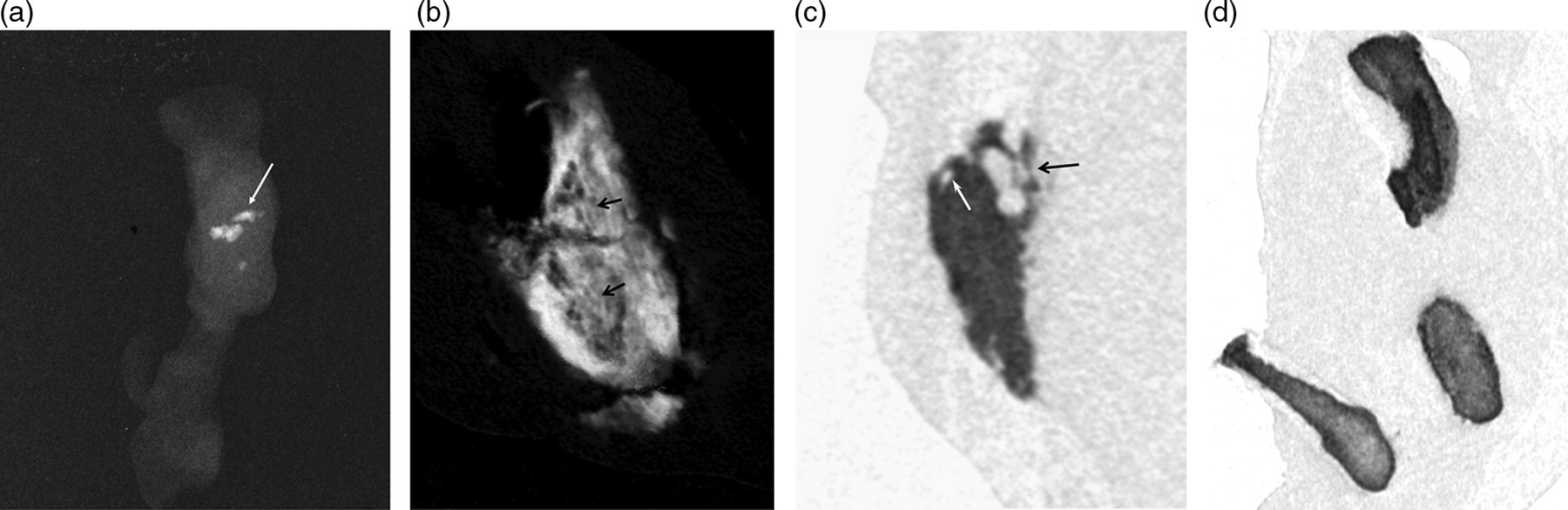
Structural analysis of microcalcifications in benign tissue by micro CT. (a) Magnification radiogram of breast core biopsy with triangular-shaped microcalcifications. Arrow indicating the microcalcification depicted in (b). (b) Thick MPR obtained from source data generated with bone reconstruction algorithm. Triangle-shaped microcalcification measuring 0.52 x 0.27 mm shows fine interior laminated texture (black arrows). The borders are sharp. (c) Thin MPR image shows triangle-shaped microcalcification 2.1 x 0.8 mm in a patient with fibrocystic glandular tissue. Trabecular pattern (black arrow), inclusion of fat (white arrow). (d) Three microcalcifications (thin MPR) without interior structure in scar tissue one year after breast biopsy
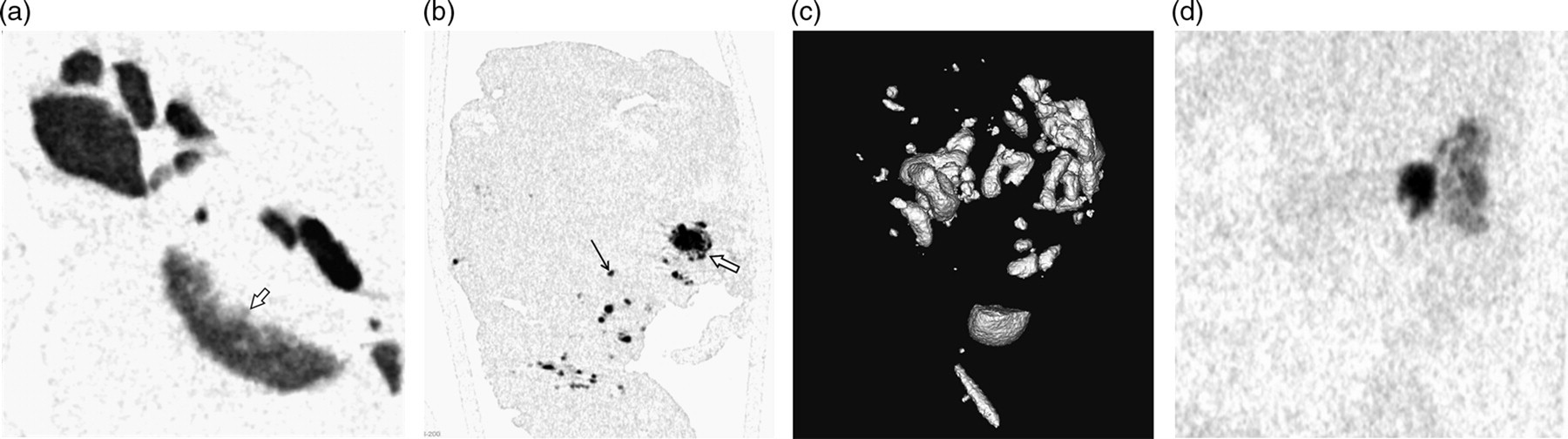
Analysis of microcalcifications in malignant lesions with micro CT (thin MPR). (a) Cluster of oval and rounded microcalcifications (diameters between 0.09 to 0.31 mm). The borders (open arrow) of the microcalcifications are not as sharp as in Fig. 1. At the periphery, a fine granular pattern is visible. The inhomogeneities in the center of the microcalcifications are most likely beam hardening artefacts. (b) Multiple small microcalcifications (black arrow) between 0.04 to 0.15 mm. One larger calcification with satellites and granular appearance in the periphery (open arrow). (c) Clusters of microcalcifications in invasive carcinoma and DCIS; reconstructed with SSD showing spatial arrangement but no internal structure. (d) Thin MPR. Single microcalcification in extensive DCIS with coarse granular interior structure
Benign microcalcifications were significantly larger (0.1–2.7 mm, mean 0.80 ± 0.92 mm) than malignant microcalcifications (0.05–0.5 mm, mean 0.24 ± 0.17; P < 0.001). The borders of benign and malignant microcalcifications showed no statistically significant differences, though benign microcalcifications tended to have sharper margins. No statistically significant difference was found for attenuation values between benign and malignant microcalcifications. Additionally, more microcalcifications were detected with micro CT imaging than with specimen radiography (P < 0.03).
Discussion
To detect the interior structure of microcalcifications, high spatial resolution of the imaging system is required. X-ray mammograms provide a spatial resolution of 50–100 µm which allows for the identification of microcalcifications. Under experimental conditions, Gong et al. used a cone-beam CT mammography with a flat-panel imager and 100 or 200 µm detectors (8). They found that microcalcifications equal to or greater than 170 µm could be detected but the authors did not report on differences in interior structure of microcalcifications. Bravin et al. used diffraction-enhanced X-ray imaging with a voxel size of 47 µm for breast tissue examination (9). Nishide et al. reported that micro CT imaging was comparable to pathological images in terms of resolution and contrast. Microcalcifications were more clearly detected on micro CT than with specimen radiographs (6). Additionally, 3D imaging of microcalcifications provided a tool for studying the shape and distribution of calcifications. Gromoll and Salomon examined four tissue samples with micro CT at a voxel size of 24.2 µm. They showed the spatial arrangement of microcalcifications in breast tissue and the distance of microcalcifications to the resection margins (7). However, neither groups reported on whether they had also examined the interior structure of microcalcifications or not.
The micro CT system we used in this study had a minimal voxel size of 8.4 µm and the spatial resolution was 17 µm. On micro CT, we found differences in the interior architecture between microcalcifications situated in benign and malignant breast tissue. Microcalcifications of benign tissue had a tendency to form a trabecular interior structure. Malignant microcalcifications showed a different pattern of interior structure with a more granular appearance. The interior structure was best seen on source images and on thin MPRs. 3D reconstructions of clusters of microcalcifications were most helpful in displaying their spatial arrangement.
Microcalcifications are responsible for the detection of 85–95% of cases of ductal carcinoma in situ by screening mammography and are visible in about 55% of non-palpable breast malignancies (10, 11). It has been shown by Brunside et al. and Bent et al. that the refined morphology microcalcification descriptors in the BI-RADS help stratify the risk of malignancy (12–14). Class IV microcalcifications showed a progressively increasing risk of malignancy from amophous, coarse heterogeneos, fine pleomorphic, and fine linear/branching. They also showed that apart from the above mentioned morphology descriptors, descriptors of distribution (ductal, scattered, regional, clustered, and multifocal) and descriptors of stability over time have impact on patient outcome.
Moreover, Tabar et al. have shown that ‘casted-like’ microcalcifications are an independent predictor of long-term outcome among women with small (T1a and T1b) invasive breast carcinomas. Patients without associated casting-type microcalcifications had excellent long-term outcomes. Women who had small invasive breast carcinomas accompanied by casting-type microcalcifications, however, had a poor prognosis despite of the small tumor sizes (15, 16). Therefore, further morphologic analysis of microcalcifications seems to be a promising field to look for tumor surrogate parameters.
Besides tissue analysis, micro CT could be considered as an additional tool to show if microcalcifications reach the borders in a lumpectomy specimen. Histological analysis is usually done on a few 3 µm-thick slices at 0.5–1 cm intervals; therefore spots of tumor may be missed at the resection border (17). We think that if micro CT is performed prior to pathological analysis, the histological examination could then be focused on already known suspicious areas with microcalcifications. This process should avoid excessive slicing and more importantly increase the rate of correct diagnoses.
There are several limitations to our study. First, the number of tissue biopsies evaluated was small. Particularly the low number and type of benign microcalcifications is a serious limitation, moreover, there were no cases of benign microcalcifications from atypical ductal hyperplasia (ADH) and flat epithelial atypia (FEA) included in the study. Therefore, the specificity of the interior structure of microcalcifications as a marker of dignity has to be confirmed in larger studies. Second, since microcalcifications in benign breast tissue were significantly larger than those in malignant lesions, the different interior structures could be related to extension rather than dignity. Third, no analysis of the microcalcifications was performed to assess their chemical composition, therefore, no information is available if presence of an interior structure is related to the type of microcalcification. Fourth, we had to use breast core needle biopsy specimens because the micro CT system was restricted to specimens not larger than 1 x 1 cm. Therefore, parameters like distance of microcalcifications from the specimen borders could only be assessed in a few cases.
In conclusion, this study shows that microcalcifications of benign and malignant tissue have different internal structures on micro CT. Although the role of micro CT for breast microcalcifications in a clinical setting is not established, micro CT can advance our understanding of breast cancer morphology. Larger studies should be performed to evaluate whether the internal structure of microcalcifications could be used as an additional prognostic parameter.