
Abstract
Background
Moyamoya disease is a chronic progressive steno-occlusion of the distal internal carotid arteries with unknown etiology. As the classical presentation of childhood Moyamoya disease is ischemic stroke, cerebral hemodynamic evaluation is important for patient selection for surgery to prevent recurrent ischemic attacks. Perfusion MR imaging has been applied to evaluate cerebral hemodynamics.
Purpose
To correlate the ‘basal time-to-peak preservation sign’, ‘auto-synangiosis sign’, and ‘posterior involvement sign’ on time-to-peak map of perfusion MRI with catheter angiography.
Material and Methods
Thirty-four children (6.91 ± 3.08 years) with Moyamoya disease who underwent both perfusion-weighted MRI and catheter angiography were enrolled in this study. Given catheter angiography as a reference standard, basal time-to-peak preservation sign, auto-synangiosis sign, and posterior involvement sign were evaluated on time-to-peak maps.
Results
The basal time-to-peak preservation sign was accurate for the diagnosis of childhood Moyamoya disease; both sensitivity and specificity were 100%. The auto-synangiosis sign showed lower sensitivity (65%), however, with an acceptable specificity (98%). The posterior involvement sign showed lower sensitivity (61%) but had an acceptable specificity (96%).
Conclusion
The basal time-to-peak preservation sign may be a universal finding in childhood Moyamoya disease. The auto-synangiosis and posterior involvement sign may be useful in determining transdural collateral status and posterior circulation involvement in childhood Moyamoya disease.
Moyamoya disease is a chronic progressive steno-occlusion of distal internal carotid arteries with unknown etiology (1–4). Angiographic appearance of bilateral supraclinoid distal internal carotid arteries (ICA) and typical Moyamoya collateral vessels are characteristic for the diagnosis of Moyamoya disease (2, 3). Initial stenosis start at the supraclinoid internal carotid arteries and then spread to the proximal parts of the anterior cerebral (ACA) and middle cerebral artery (MCA). In severe cases and later stages of the disease, stenosis also involves the posterior cerebral artery (PCA).
The age distribution is bimodal with a first peak occurring in the first decade and the second in the fourth decade (4). Ischemia is a major feature of Moyamoya disease in childhood (5, 6). On the other hand, intracranial hemorrhage is a major feature in adulthood (4, 7). Because the classical presentation of childhood Moyamoya disease is ischemic stroke, cerebral hemodynamic evaluation is important for patient selection for surgery to prevent recurrent ischemic attacks (8).
MRI has advantages as a non-invasive examination due to lack of radiation and small usage of contrast agents. Recently, perfusion MR imaging has been applied to evaluate cerebral hemodynamics and the results showed good correlation between time-to-peak (TTP) map and cerebral hemodynamics or clinical outcome after surgery (9, 10–12). According to the pathophysiology of Moyamoya disease, dilated striate arteries and external carotid artery (ECA) collaterals can relatively well preserve blood perfusion to the corresponding brain tissue. Encephalo-dural-arterio-synangiosis is a commonly used surgical technique for developing brain surface collaterals from ECA, and time-to-peak (TTP) preservation is also observed at the areas of neovascularization (13). This time-to-peak (TTP) preservation can also be seen without surgery due to self-development of transdural collaterals (auto-synangiosis sign). We also evaluated TTP preservation of basal ganglia by Moyamoya vessels (basal TTP preservation sign) and correlated them with angiographic findings. As Moyamoya disease progresses, defection on posterior cerebral arteries occur in later stage of the disease (4) and TTP delay is observed (posterior involvement sign). The purpose of this study was to correlate these signs on TTP map with catheter angiography as a reference standard.
Material and Methods
Patient population
Thirty-four patients (15 boys and 19 girls) with Moyamoya disease who underwent both MRI and catheter angiography between June 2003 and January 2006 were enrolled in this study. Recent patients were not included because surgery is now performed based on MR angiography findings only. An institutional review board (IRB) approved this retrospective study and waived informed consent form for the retrospective analysis. The mean age of the patients were 6.91 ± 3.08 (mean ± standard deviation, range 2–13 years). Perfusion MR imaging was performed in all patients. The reasons for MRI examination included TIA or infarct (n = 28), seizure (n = 3), headache (n = 2) and aphasia (n = 1). Catheter angiography was performed to evaluate the collateral status and to visualize external carotid arteries for surgical planning when disease progression was suspected on MRI. The interval between MRI and catheter angiography was 5.91 ± 10.76 days (mean ± standard deviation, minimum 0 and maximum 39 days).
Image acquisition and analysis
The MR examinations were conducted by a 1.5T system (Achieva; Philips Medical Systems, Best, The Netherlands) with a 8-channel head coil. Dynamic susceptibility contrast-enhanced perfusion MRI was obtained after injection of 0.2 mmol/kg gadopentetate dimeglumine (Magnevist; Bayer Schering Pharma AG, Berlin, Germany) at a rate of 2mL/s by using the following parameters: TR/TE/excitations 1500 msec/40 msec/1; matrix 128 × 128; field of view 24 cm; section thickness 5 mm; and intersection gap 2 mm. Relative CBV and TTP maps were generated at the off-line workstation. The imaginary area of basal ganglia and posterior circulation on perfusion MR image was used for analysis (Fig. 1) (13). TTP maps were evaluated with emphasis on TTP preservation on basal ganglia and hemispheric cortex. Yellow in red on color-coded TTP map, i.e. 2 seconds or more than 2 seconds shorter TTP compared with adjacent brain tissue, were considered as a positive sign of basal preservation sign and auto-synangiosis sign according to their locations: basal ganglia or hemispheric cortex (Fig. 2). The posterior involvement sign was also evaluated by the presence of red on color-coded TTP map in the territory of posterior cerebral artery (Fig. 3). Two experienced neuroradiologists (SKL and HSC) reviewed the TTP maps and the above mentioned signs in consensus. Kappa statistics were calculated for inter-observer agreement of the positive signs. Catheter angiography was performed with selection of bilateral internal carotid arteries, external carotid arteries, and vertebral arteries. The ‘basal TTP preservation sign’, auto-synangiosis sign, and posterior involvement sign were correlated with catheter angiography as a reference standard. Sensitivity and specificity of each signs were calculated.
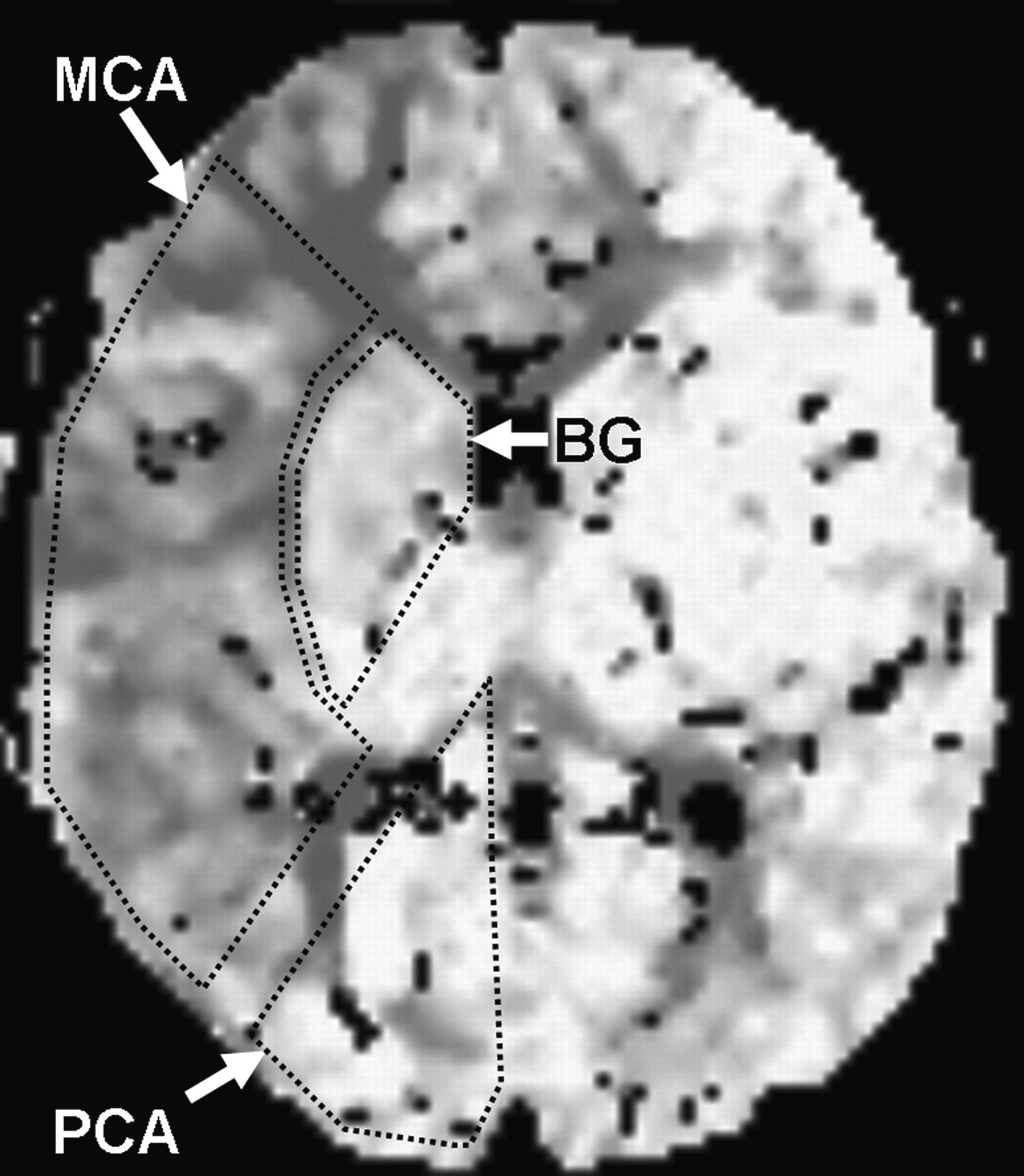
Imaginary territories of middle cerebral artery (MCA), posterior cerebral artery (PCA), and basal ganglia (BG) are drawn on a time-to-peak (TTP) map
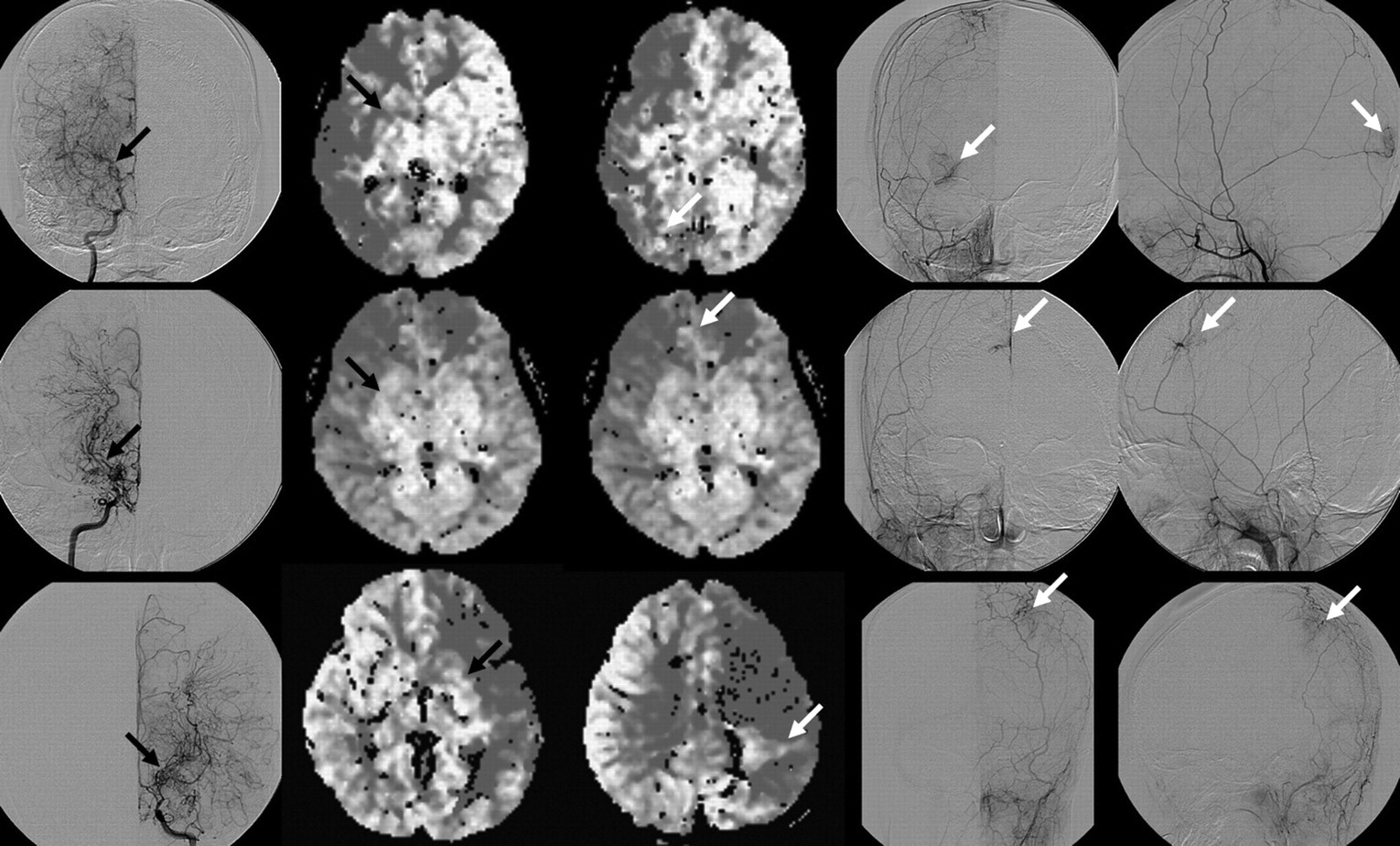
‘Basal TTP preservation sign’ and auto-synangiosis sign on time-to-peak (TTP) map shows correlation with catheter angiography. Black arrows indicate moyamoya vessels on catheter angiography (first column) and ‘basal TTP preservation sign’ on TTP map (second column); white arrows indicate transdural collaterals on catheter angiography (fourth and fifth columns) and auto-synangiosis sign on TTP map (third column)
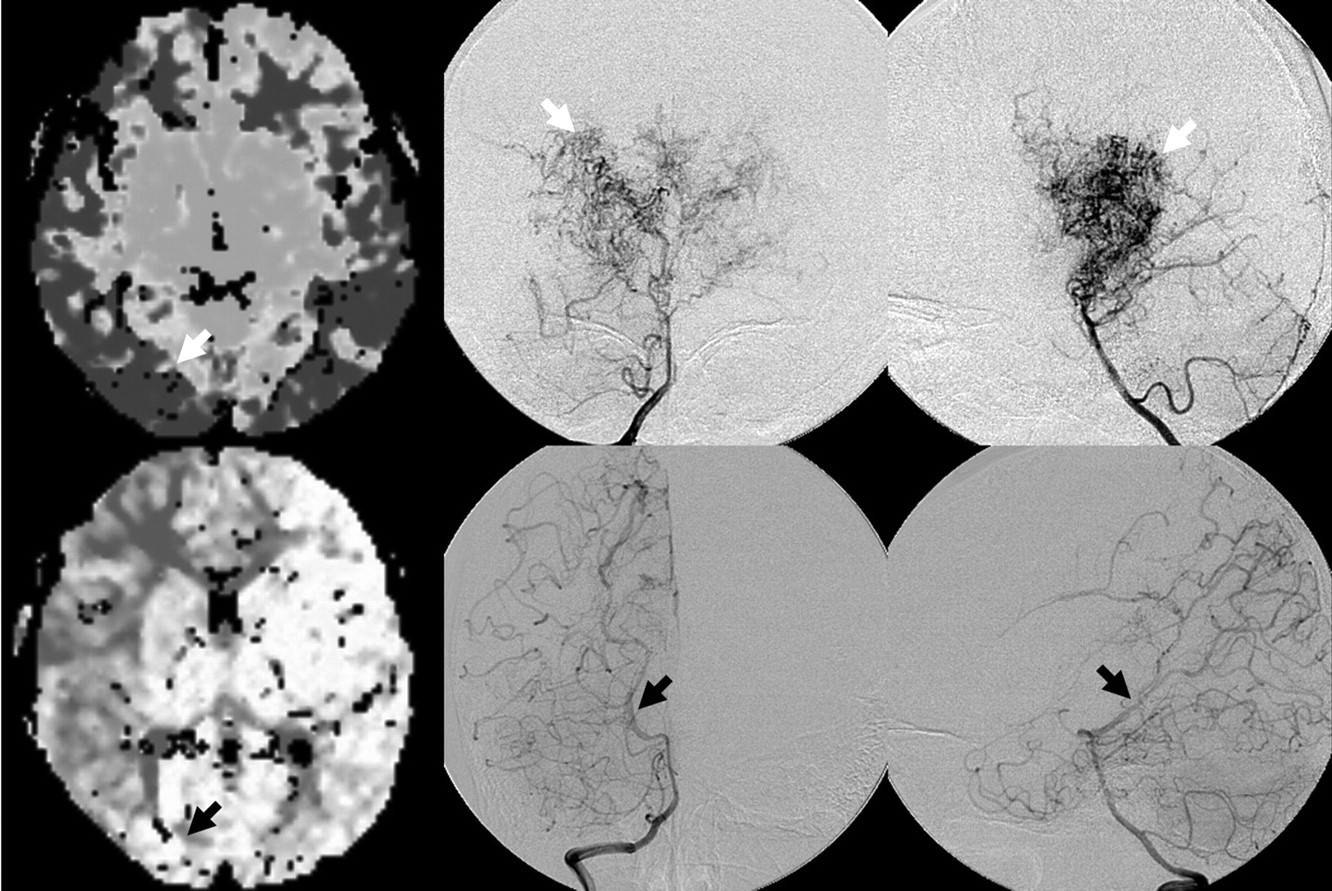
Posterior involvement sign on time-to-peak (TTP) map shows correlation with catheter angiography. White arrows indicate posterior involvement sign on TTP map (first column) and defection of posterior cerebral artery on catheter angiography (second and third column); black arrows indicate negative posterior involvement sign on TTP map (first column) and no defection on posterior cerebral artery (second and third column)
Results
Catheter angiography revealed overall 63 stenotic distal internal carotid arteries with Moyamoya vessels consistent with Moyamoya disease. TTP maps on perfusion MR imaging revealed positive ‘basal TTP preservation sign’ in all affected 63 hemispheres (Fig. 2) and negative basal TTP preservation sign in five unaffected hemispheres, i.e. both 100% sensitivity and specificity. Auto-synangiosis sign showed a sensitivity of 65% and a specificity of 98% in detecting ECA transdural collaterals with poor inter-observer agreement (0.31 of kappa statistic) (Table 1). The location of auto-synangiosis sign was correlated well with the areas of the catheter angiography if the two observers agreed with consensus (Fig. 2). Posterior involvement sign was positive in 14 out of 23 hemispheres with defection of the posterior cerebral artery (Fig. 3). The posterior involvement sign had a sensitivity of 61% and specificity of 96% with excellent inter-observer agreement (0.84 of kappa statistic) (Table 2).
The number of hemispheres in relationship between auto-synangiosis sign on time-to-peak map and ECA (external carotid artery) transdural collaterals on catheter angiography
The number of hemispheres in relationship between posterior involvement sign on time-to-peak map and PCA (posterior cerebral artery) defection on catheter angiography
Discussion
Moyamoya disease is a chronic progressive vasculopathy which changes dynamically and Suzuki suggested a staging system by conventional angiographic appearance of the disease (4). Steno-occlusive changes of the distal ICA and development of collateral circulation are in reciprocal dynamic relationship, thus monitoring the disease progression is essential for medical or surgical management (14–17). Because catheter angiography has risks of complications related to the procedure itself or anesthesia, non-invasive imaging modalities should be used for clinical follow-up and guidance for time of surgical management (18). There have been various non-invasive modalities to assess cerebral hemodynamic status qualitatively or quantitatively (9–13, 18–23). Perfusion MR imaging has been widely used for preoperative or postoperative follow-up imaging of childhood Moyamoya disease (10, 12, 13, 24, 25).
Delayed TTP of the anterior circulation compared with normal subjects has been reported (13). Correlation studies with perfusion MRI and catheter angiography have shown that the mean transit time of the anterior circulation positively correlated with the degree of ICA stenosis (21). The ‘basal TTP preservation sign’ was a universal sign of steno-occlusion of distal ICA. Its diagnostic sensitivity and specificity for Moyamoya disease was both 100%. In our series, only five non-affected hemispheres were included for normal controls because age-matched normal control subjects could not be recruited due to ethical considerations for sedation. We therefore consider that ‘basal TTP preservation sign’ is a pathognomonic sign in childhood Moyamoya disease. Further investigations for this sign with a larger number of normal subjects seem, however, necessary.
The detection of well-developed basal Moyamoya vessels and steno-occlusion of distal ICA is not difficult on time of flight (TOF) MR angiography. However, for the evaluation of transdural collaterals a variety of results have been presented (14, 15, 17). Small diameter and transdural tortuous ECA collaterals can be easily saturated and may not be visible on TOF MRA. In our series, any ECA collaterals penetrating the dura were not identified on non-contrast TOF MRA. Although contrast-enhanced MR angiography will demonstrate transdural collaterals more clearly than non-contrast TOF MRA, there are no reports about this to the best of our knowledge. We expected TTP map on perfusion MRI to visualize areas supplied by ECA collaterals better. However, the results showed 65% sensitivity and 98% specificity with poor inter-observer variation. The relatively low sensitivity with poor inter-observer variation in detecting transdural collaterals may be attributed by small areas of TTP preservation intermingled in the affected hemisphere, partial volume artifacts, and noise derived from poor spatial resolution of TTP map.
It is well-known that Moyamoya disease involves the posterior circulation in later stages (4). Minimization of the basal Moyamoya vessels and progressive occlusion of the ICA, which reaches the origin of the PCA occur in Suzuki stage 4. Further reduction of Moyamoya vessels, complete disappearance of main cerebral arteries and increased collateral supply from the ECA occur in Suzuki stage 5. Our series have 23 hemispheres of Suzuki stage 4 or 5, and 14 hemispheres which showed TTP delay in the posterior cerebral artery territory, i.e. red on color-coded TTP map in PCA territory. There was also a tendency for more frequent transdural collaterals in Suzuki stage 4 or 5 in our series. The combination of auto-synangiosis sign and posterior involvement sign on TTP map may help to predict later stage of the disease, to monitor disease progression, and to select symptomatic candidate for surgery.
There are limitations in this study. Our algorithm for calculating TTP maps without arterial input function and deconvolution inevitably produced relative values of TTP. Therefore, there may be over- or under-estimation of TTP. Second, because SPECT with acetazolamide challenging test was not analyzed and correlated with perfusion MR imaging, our suggested signs and their meaning of cerebral hemodynamics should be further verified, pre- or postoperatively. Finally, imaginary line for posterior circulation which was introduced in our study may be a potential bias because altered hemodynamics in Moyamoya disease can change the area supplied by the posterior circulation.
In conclusion, the basal time-to-peak preservation sign may be a universal finding in childhood Moyamoya disease. Auto-synangiosis sign and posterior involvement sign may be useful in determining transdural collateral status and posterior circulation involvement in childhood Moyamoya disease.
Footnotes
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (KRF-2008-331-E00247).