
Abstract
Wandering spleen is rare and is associated with a high incidence of splenic torsion and infarction. Presenting symptoms range from an asymptomatic, incidentally palpated abdominal mass to an acutely ill patient. Because wandering spleen is uncommon in the pediatric population, a heightened awareness of the condition is required for accurate diagnosis and appropriate management. We present a case of a 4-year-old girl who presented with acute abdomen and was surgically confirmed to have a wandering spleen with torsion and complete infarction.
Wandering spleen is a rare clinical entity with a reported incidence of less than 0.2% (1). The cause for splenic hyper-mobility may be absence or maldevelopment of the supporting ligaments (2). To date, there are eight reported cases of wandering spleen with torsion in adults and 10 cases in children, most of whom are younger than 6 years of age (1–12). Wandering spleen with complete infarction and necrosis is seldom reported. We present the CT features with pathological correlation of a child with wandering spleen and complete splenic infarct.
Case report
A 4-year-old girl presented with a 7-day history of acute intermittent left abdominal pain. There were no complaints of fever, nausea or vomiting. She had undergone appendectomy two weeks previously in another hospital. On physical examination a large tender lower abdominal mass was palpable. Laboratory investigation showed an increased platelet count of 824 × 109/L and white blood cell count of 13 × 109/L as well as a reduced hematocrit of 0.363. Abdominal radiographs demonstrated slightly dilated small bowel loops. No spleen was visualized in the left upper abdomen on ultrasound examination. There was a 12 × 4 cm mass in the left lower abdomen with reduced Doppler blood flow suggesting a wandering spleen (Fig. 1). Axial unenhanced CT scan confirmed absence of spleen in the left upper abdomen and an 11.5 × 5 cm mass in the left lower abdomen and pelvis. The mass was encapsulated with homogeneous low density of around 40 Hounsfield units. After intravenous contrast injection, the capsule of the mass enhanced homogeneously without parenchymal enhancement. The splenic artery and vein were abruptly interrupted at the hilum of this mass (Fig. 2a). Coronal reconstructed contrast-enhanced CT scan showed the mass suspended by a dilated tortuous vascular pedicle arising from the portal vein and vascular occlusion in the hilum of this mass (Fig. 2b). A diagnosis of wandering spleen with torsion was made. Intraoperatively, a completely infarcted spleen was found in the left lower abdomen adhering to small bowel loops (Fig. 3). The histopathological examination of the resected spleen revealed complete hemorrhagic infarct (Fig. 4). The postoperative recovery was uneventful and the patient was discharged 12 days later.
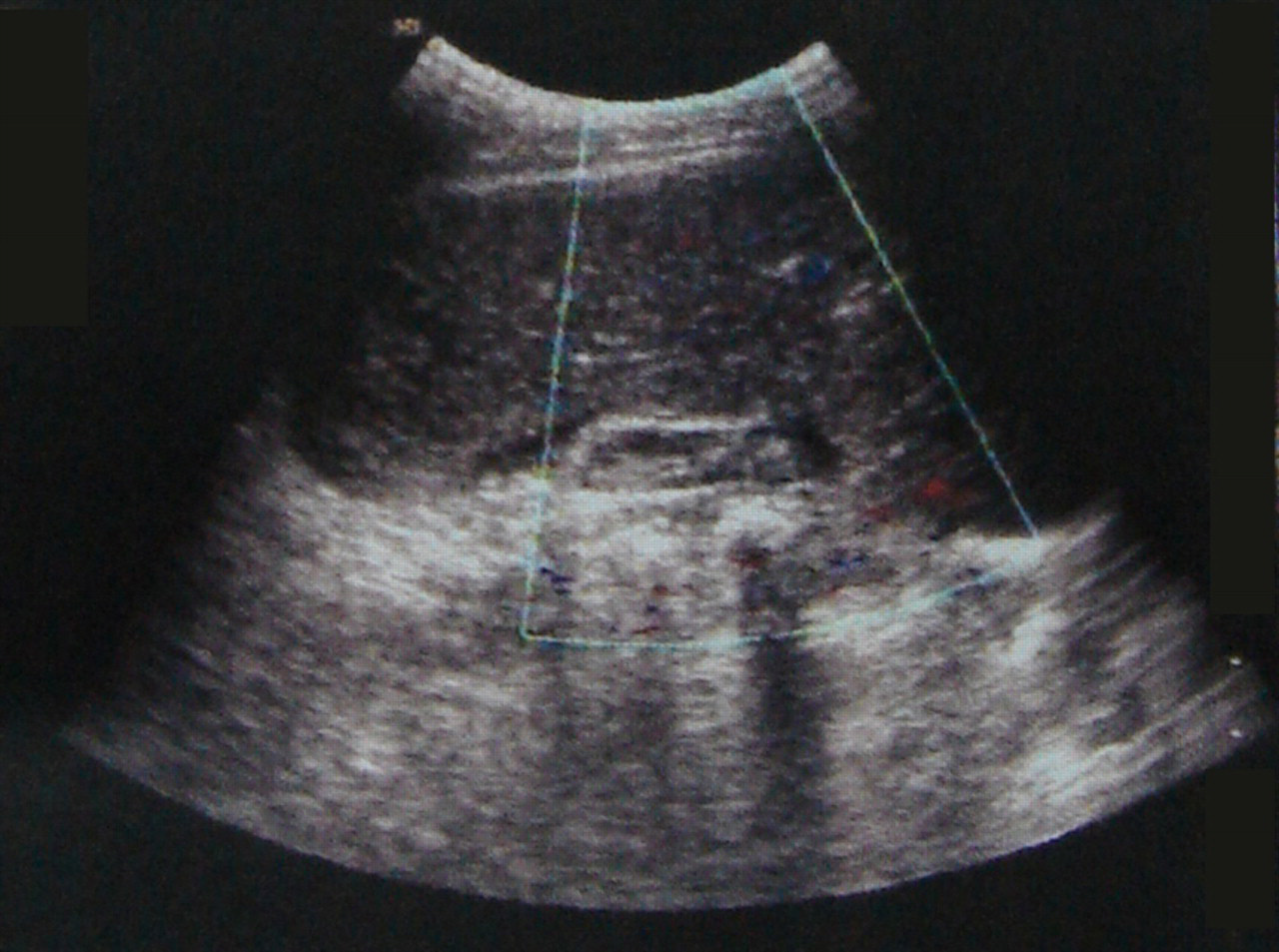
Transverse Color Doppler sonogram shows absence of blood flow in the parenchyma and hilum of a spleen-like mass in the left lower abdomen
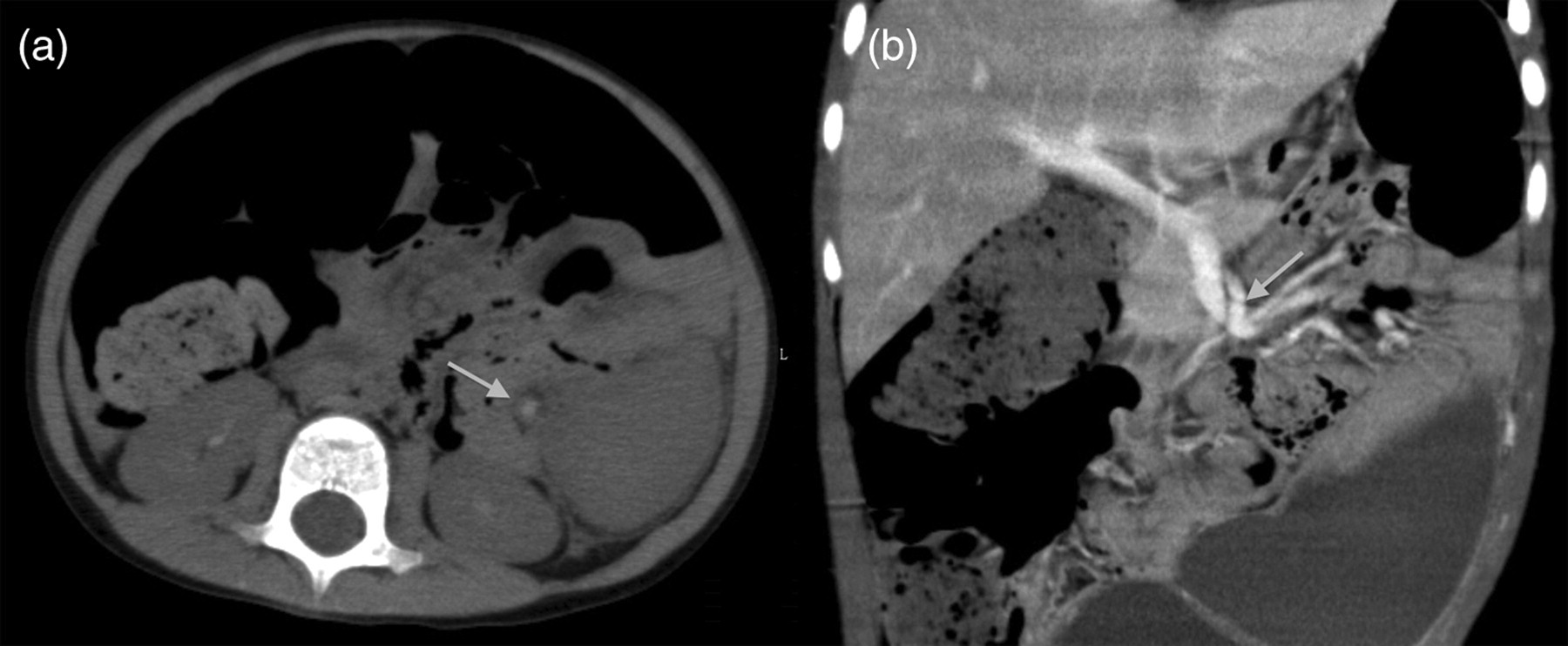
(a) Axial unenhanced CT image demonstrates a small hyperdense solid component at spleen hilum (white arrow) surrounded by fat density suggesting thrombus in the splenic vein. (b) Coronal reconstructed contrast-enhanced CT scan shows a large well-defined mass in the left lower abdomen suspended by a dilated and tortuous vascular pedicle (white arrow) draining into the portal vein
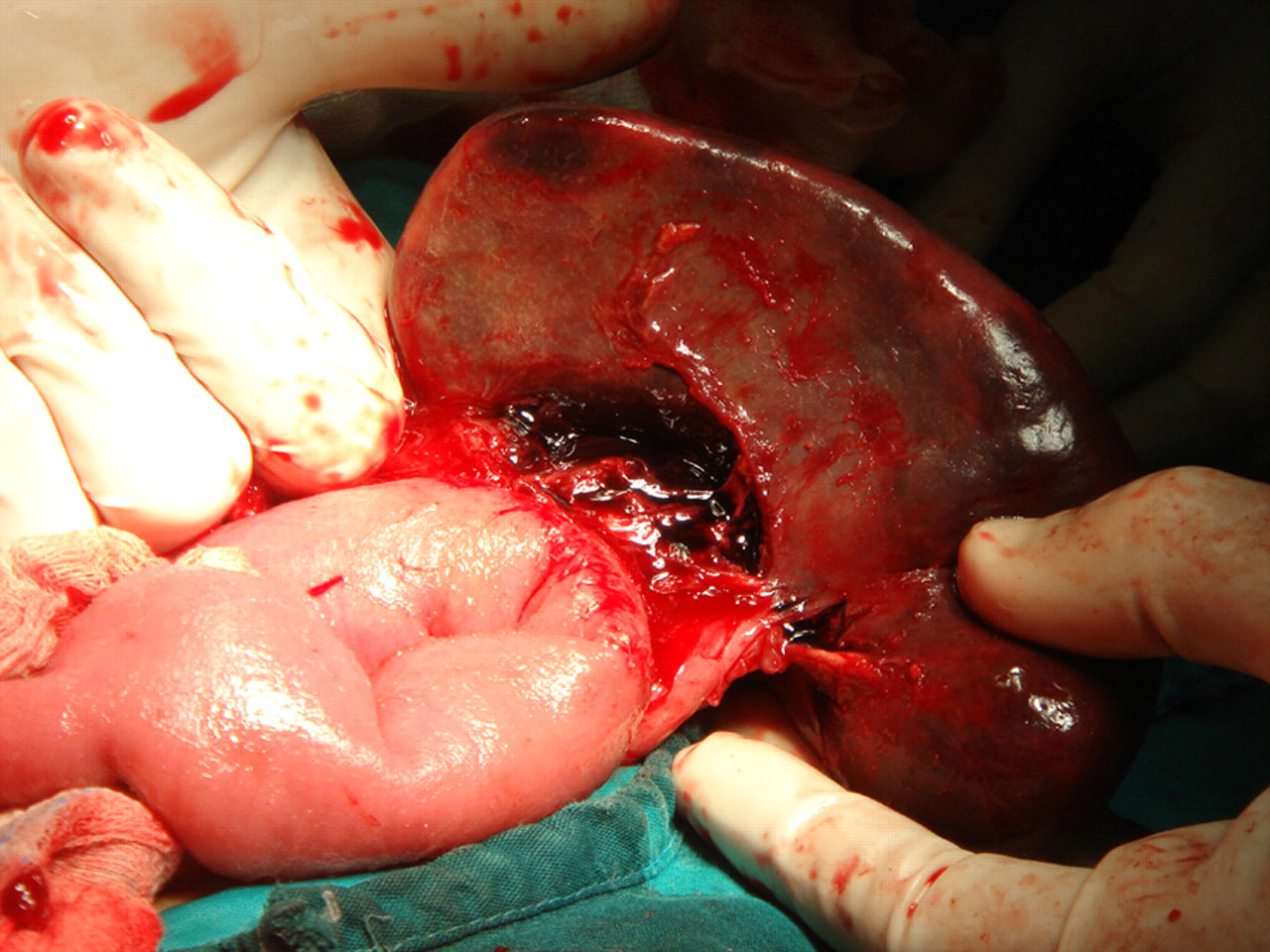
Intraoperative view shows a congested, hemmorhagic spleen with torted and thrombosed vessels. Note multiple wedge-shaped splenic infarcts
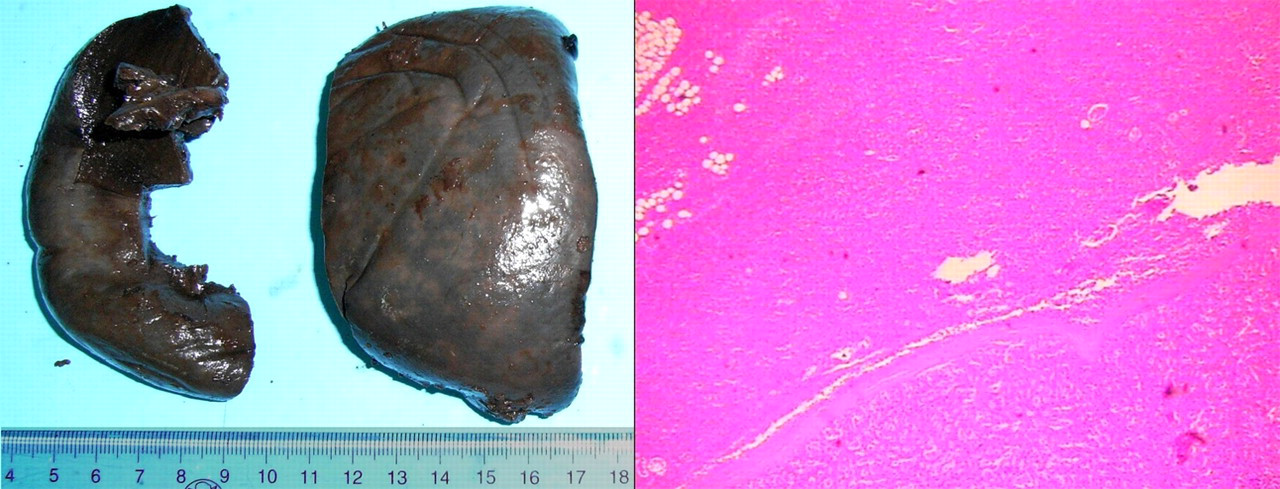
Gross specimen showed visceral surface of a large congested spleen with infarction. Hemorrhagic spleen infarction was confirmed histologically (H&E × 20)
Discussion
Wandering spleen may be congenital or acquired (10). Congenital wandering spleen is caused by absence of fixating ligaments or abnormally long ligaments and is more commonly found in children accounting for half of the reported cases (2–12). Acquired wandering spleen is most common in women because of ligamental laxity from hormonal changes during pregnancy (2, 6).
The clinical presentation of wandering spleen is variable. Most patients with wandering spleens are asymptomatic (4, 5). A mobile non-tender abdominal mass can be found on routine physical examination. Abdominal pain, gastrointestinal disturbances, dysuria, and irregular menstruation can occur because of compression of adjacent organs by the ectopic spleen (4, 10). Unusual presentations include pancreatitis from necrosis of the pancreatic tail, and esophago-gastric varices and upper gastrointestinal bleeding from portal hypertension secondary to chronic splenic torsion (5, 6, 11, 12).
In torsion, the venous drainage is initially compromised, later leading to arterial occlusion. The imaging appearance will vary depending on the phase – acute/chronic and the degree of torsion – partial or complete. Most of the reported cases presented with incomplete splenic torsion. Incomplete splenic torsion results in reduced splenic blood flow and congested splenomegaly. Complete torsion leads to splenic vascular occlusion and splenic necrosis. Our patient presented with complete torsion and total necrosis.
Accurate preoperative diagnosis of wandering spleen with or without torsion is difficult without imaging evaluation because of its rare occurrence (8). Evaluation of wandering spleen with torsion includes abdominal radiographs, ultrasound and CT. The common findings for incomplete and complete splenic torsion are listed below. Intestinal obstruction is a common finding on abdominal radiographs, sometimes with a soft tissue mass or gas-filled bowel loops in the left abdomen replacing the splenic silhouette (5). Ultrasound examination can demonstrate absence of spleen in the left upper abdomen and an encapsulated lower abdominal or pelvic mass with homogeneous echogenicity. In our case, color Doppler sonography shows dilatation of the splenic vein and markedly reduced splenic blood supply. On non-enhanced CT, the density of spleen parenchyma was less than normal hepatic parenchyma. Splenic pedicle showed slight hyperdense sections suggesting thrombosis in spleen vessels. After contrast media administration, a cork screw-like soft tissue density containing enhanced splenic vessels and fat on coronal reconstructed CT represented the distorted splenic pedicle and surrounding fat tissue. Other CT findings, such as a lower abdominal mass with a homogeneous capsule and patchy contrast enhancement, indicate compromised perfusion to the wandering spleen (3). In addition, mild contrast enhancement may be attributed to collateral circulation from the short gastric and left gastric veins (1).
In our case, a wandering spleen with torsion and complete infarction was seen. We would like to emphasize several subtle but important findings. Color Doppler sonography showed heterogeneous echogenicity in spleen parenchyma without any detectable blood flow. Slight hyperdense sections in the splenic pedicle may be a subtle finding suggesting thrombosis in splenic veins on non-enhanced CT. Ring enhancement of the spleen capsule and no enhancement in spleen parenchyma was also typical findings of complete infarction on contrast-enhanced CT.
Since wandering spleen is a rare cause for acute abdomen, other causes should be taken into account. More common causes of an acute abdomen in the pediatric population include intestinal obstruction, appendicitis, intussussception and more rarely pancreatitis. The spleen will be in a normal position in these conditions.
Treatment for wandering spleen depends on the viability of the spleen (2). Splenopexia is performed in patients with incomplete torsion. Splenectomy is required when the wandering spleen infarcts.
In conclusion, wandering spleen with torsion is a rare cause of acute abdomen. The accurate preoperative radiologic diagnosis and assessment for complete and non-complete torsion of wandering spleen are crucial due to different surgical options. Both ultrasound and coronal reconstructed CT scan can play important roles in assessing position of the spleen, thrombosis on spleen vessels and viability of the spleen.
Footnotes
ACKNOWLEDGMENTS
The authors thank Dr Margaret Pui and Linda Zhang for their help in revising this paper.