
Abstract
This report deals with two rare but similar cases of asymptomatic fracture of a Bird's Nest inferior vena cava (IVC) filter strut, penetrated into the liver parenchyma. Follow-up over 4 and 6 years, respectively, could not reveal any changes in the position of the fragmented strut in the liver parenchyma or any evidence of clinical symptoms owing to the migrated strut fragment.
The placement of a permanent inferior vena cava (IVC) filter is an accepted, minimally-invasive treatment option in patients suffering from recurrent pulmonary embolism despite anticoagulation therapy or in patients presenting with acute venous thromboembolism and a contraindication for anticoagulation (1). The Bird's Nest IVC filter (Cook Medical, Bloomington, IN, USA) was evaluated during clinical trials from 1982 to 1988 and has been approved by the US Food and Drug Administration in 1989, after several cohort studies had demonstrated its safety and effectiveness in the prevention of pulmonary embolism (2, 3). However, over the years, several small series and case reports have reported on early and late complications owing to a structural failure of the filter device (4–8). In this report, we describe two similar cases of late but asymptomatic penetration of a rostral fractured Bird's Nest filter strut into the liver parenchyma, with a stable positioning of the migrated strut over several years.
Case reports
Case 1
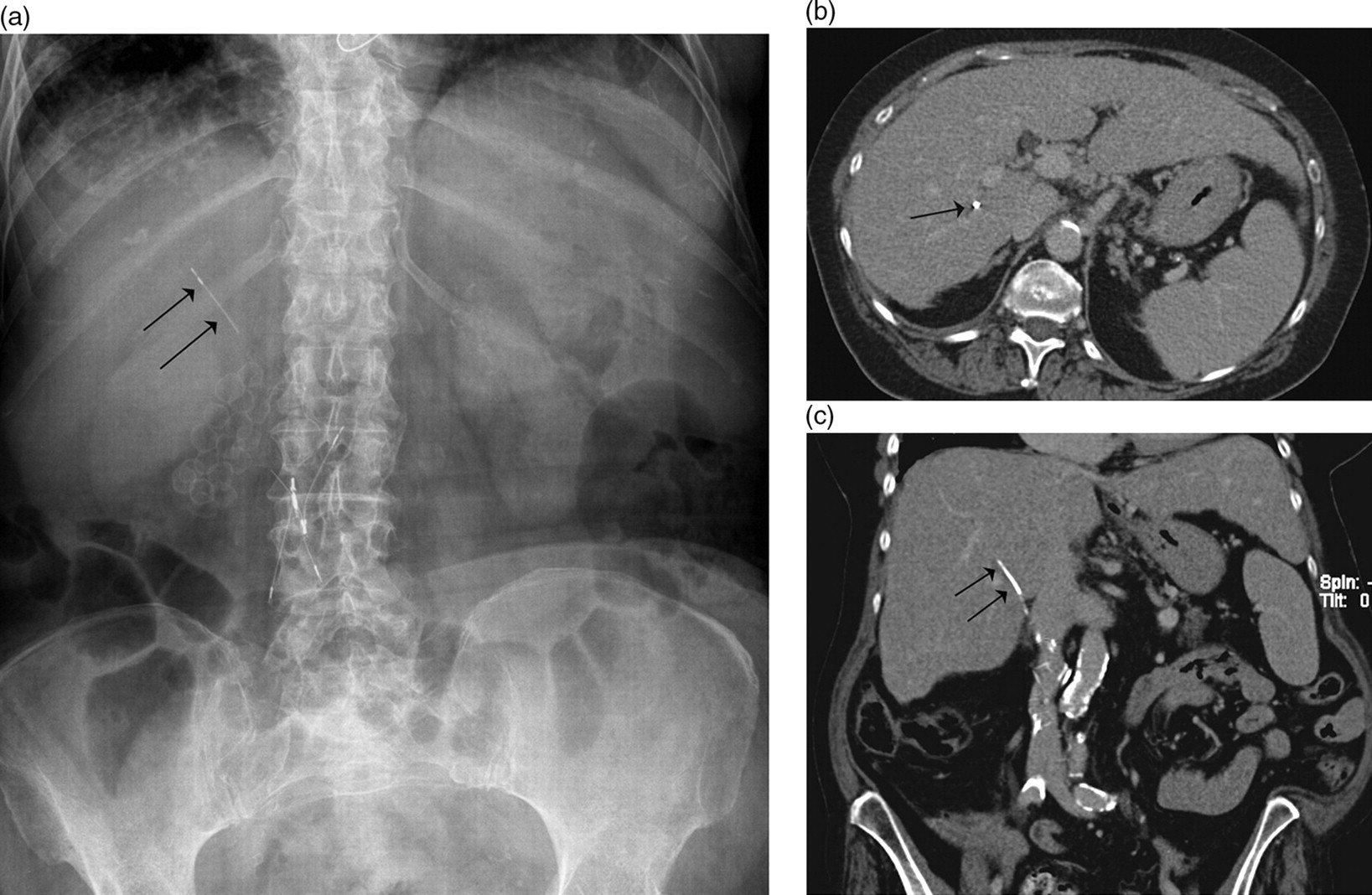
A 75-year-old woman with a past medical history of severe, chronic thromboembolic pulmonary hypertension managed with a bilateral pulmonary endarterectomy and the placement of a permanent IVC filter (Bird's Nest, Cook Medical, Bloomington, IN, USA) in the infrarenal vena cava, presented with hemodynamic shock related to a spontaneous rectus sheath hematoma. Radiological work-up, including plain film and computed tomography (CT) of the abdomen, revealed a major rectus sheath hematoma with an active bleeding. Subcutaneous administration of low-molecular-weight heparin was temporarily stopped and the patient was treated by a transcatheter embolization of the right inferior epigastric artery. Additionally, the Bird's Nest filter, successfully placed 9 years earlier, showed multiple structural defects. One of the cephalad struts was fractured and had penetrated into the liver parenchyma (Fig. 1a and b); the caudal V-shaped struts had perforated both the right proximal common iliac artery and vein. The patient was asymptomatic for the migrated strut and for the erosion of the distal struts into the common iliac vessels. There were no clear clinical signs pointing to recurrent pulmonary thromboembolism. A retrospective analysis of the patient's radiological records could depict the fractured and migrated strut on an abdominal plain film, which had been made 4 years earlier for the investigation of back pain (Fig. 1c). The migrated strut projected at the same position as on the plain film 4 years later.
Contrast-enhanced axial (a) and reconstructed coronal (b) abdominal CT images reveal a metallic, needle-like foreign body (black arrow), located in the right liver lobe; (c) Abdominal plain film confirms the presence of a migrated cephalad strut (black arrows) of the Bird's Nest filter, projecting in the right hypochondrium at the level of the 12th thoracic vertebra
The patient recovered from this bleeding event and was discharged without any intervention as to retrieve the migrated strut or erosed filter fragment.
Case 2
A 64-year-old woman with a past medical history of bilateral pulmonary emboli and progression to chronic pulmonary hypertension underwent pulmonary endarterectomy and placement of a Bird's Nest IVC filter in the inferior vena cava 11 years ago. The patient recovered well without any residual clinical signs of pulmonary hypertension. An abdominal plain film some years ago revealed that a strut fragment of the filter had migrated into the liver parenchyma. At that time, the filter function seemed to be intact without any clinical evidence of recurrent pulmonary thromboembolism. There was no evidence of clinical symptoms owing to this structural failure of the filter device and the patient was further managed conservatively. Up to 6 years later, control abdominal X-rays (Fig. 2a) did not reveal any changes in the position of the migrated strut, which was still located within the liver parenchyma, as demonstrated by CT scan (Fig. 2a and b). The patient is still doing well without any complaints related to the migrated strut.
(a) Abdominal plain film demonstrates a migrated strut (black arrows) of the Bird's Nest filter, projecting in the right hypochondrium at the level of the 12th rib. Corresponding axial (b) and reconstructed coronal (c) abdominal CT images confirm the presence of the migrated strut (black arrow) in the right liver lobe
Discussion
Complications like malposition or cephalad migration of the filter device and puncture site thrombosis (4) can occur after the insertion of IVC filters. Other complications will be detected early or late after successful placement. Among this type of complications, the most frequently reported ones are insufficient clot trapping resulting in recurrent pulmonary embolism, IVC obstruction, lower extremity venous insufficiency and finally, a number of late complications directly related to the filter device itself, such as: strut erosion through the IVC wall (5) (or in extreme condition through the aorta resulting in a bleeding aortic pseudoaneurysm [9]), late filter migration, strut fracture and strut penetration of the IVC wall with further migration of the fractured strut into one of the surrounding organs of the IVC (the peritoneum [10], the duodenum [6], the pancreas [11], the right ureter [12] or even the right atrium, and beyond the pulmonary arteries after cephalad migration [8]).
In the two particular cases presented, one cephalad strut of the Bird's Nest filter first penetrated the IVC wall and then progressively migrated into the liver parenchyma. The reason why the liver was perforated by the strut was probably related to the right anterolateral position of the strut after filter deployment and to the level in the infrarenal IVC where the strut was deployed. It is still unclear why one or more struts of the Bird's Nest will fracture and subsequently penetrate and migrate into a surrounding structure; however, some hypotheses have been made like excessive traction on the guide wire pusher during delivery, structural failure of the hooks or the very broad deployment of the struts up to 6 cm in diameter when placed in vitro outside a tube structure (7). Potentially, wall penetration of one of these struts might be more obvious in small calibre IVCs.
Interestingly, in the two presented cases, the migration of the fragmented strut stopped when completely embedded in the liver parenchyma as demonstrated by two abdominal plain films with 4 and 6 years interval, respectively. This sustained stable position without any clinical symptoms at all, convinced us not to intervene to retrieve the migration strut fragment or to place an additional filter in the IVC or both iliac veins as in both patients there was no clear evidence of recurrent pulmonary embolism.
However, we suggest controlling the position and structure of all filter devices by plain X-rays on a regular basis as already proposed by Nicholson et al. (13) who detected fracture and fragmentation of the Bard retrievable IVC filter in up to 25% of cases. For other types of filter devices, like the Bird's Nest filter, no such long-term follow-up has ever been done, certainly not in a group of patients with a long life expectancy after filter insertion.
In conclusion, two similar complications with an initially correctly placed Bird's Nest filter are presented, consisting in a late strut fracture with penetration and migration into the liver parenchyma. Because of the sustained stable position of the fragmented strut in the liver parenchyma over 4 and 6 years, respectively, without any related clinical symptoms, it was decided to follow-up the patients without any attempt to retrieve the fragments.