
Abstract
Chondromyxoid fibroma (CMF) is a rare benign bone tumor of chondroid origin that occurs mostly in the metaphyses of long bones. CMF can occasionally mimic a chondrosarcoma on CT, and the literature on the 18F-FDG PET/CT imaging characteristics of CMF tumors is limited. In the presented case, a large histologically proven CMF chest wall mass was initially misinterpreted as a chondrosarcoma. This case highlights a potential pitfall in the PET/CT evaluation of these rare benign bone tumors.
Chondromyxoid fibroma (CMF) is a rare benign bone tumor of chondroid origin that accounts for less than 0.5% of all primary bone tumors. (1, 2). CT imaging findings of CMF have been described (3–10) and in rare cases, CMF has been mistaken for a chondrosarcoma on CT as well as pathology (1, 5–10). 18F-FDG PET/CT is useful in differentiating some benign bone tumors from malignant bone tumors, and in the case of CMF tumors, only mild FDG uptake has been described. However, the literature regarding the PET/CT imaging characteristics of CMF tumors is very limited compared to the PET/CT literature on chondrosarcomas and it is important to be aware of this limitation (11–16). We report a case of a CMF of the rib misinterpreted as a chondrosarcoma based on PET/CT imaging characteristics.
Case report
A 60-year-old man presented with a several week history of persistent cough, and had a chest radiograph (Fig. 1) showing an expansile left upper chest wall mass. He was referred for a contrast-enhanced CT and an 18F-FDG PET/CT. The contrast-enhanced CT (Fig. 2) showed a 9.0 × 6.5 × 5.5 cm expansile lytic lesion replacing most of the left first rib, sparing the tubercle and neck. There was also extrinsic compression and occlusion of the left brachiocephalic vein between the lesion and the clavicle with opacification of extra thoracic venous collaterals. There was no supraclavicular, axillary or mediastinal adenopathy. The CT was interpreted as strongly suspicious for a chondrosarcoma.

A chest X-ray of a 60-year-old man who presented with a several week history of cough showed an expansile lytic mass involving the first rib (arrows)
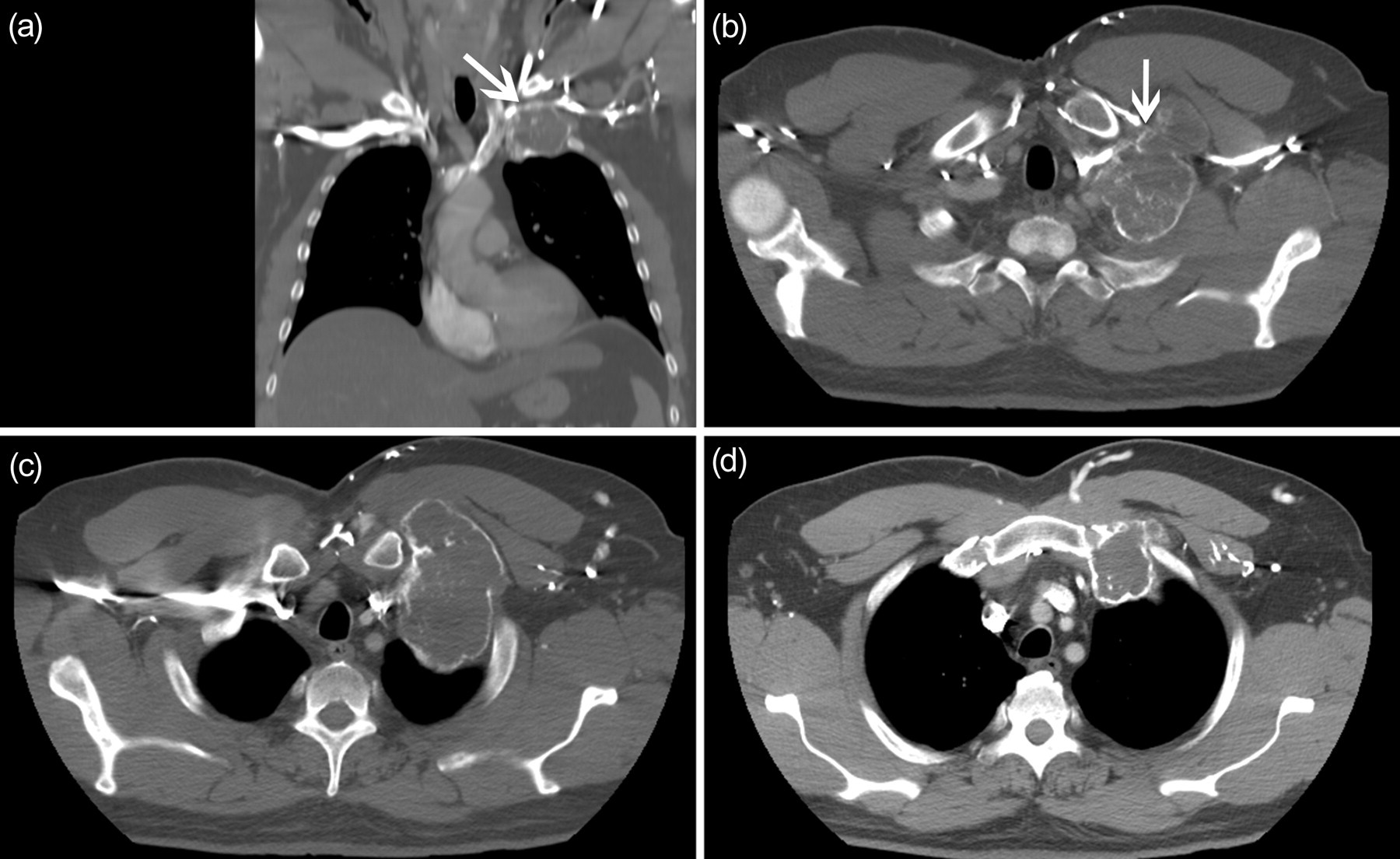
(a) Coronal view of a contrast-enhanced CT showed a mass arising from the left first rib, causing compression of the left brachiocephalic vein between the lesion and the clavicle (arrow), which can also be seen on the (b) transaxial views (arrow), along with contrast opacification of extrathoracic venous collaterals just left of the midline. The left subclavian artery was patent and there was no clinical evidence of venous obstruction of the neck; (c) and (d) are selected sequential transaxial views which revealed diffuse calcifications in the first rib mass. The mass appeared to invade into the pectoralis muscles but was contained by a thin shell of bone. The CT findings of the chest wall mass were strongly suggestive of a chondrosarcoma. Additional superficial venous collaterals were seen in the left axilla
An 18F-FDG PET/CT (Discovery ST, GE Healthcare, Montreal, Canada) was obtained the same day (Figs. 3 and 4). The patient fasted overnight prior to the examination, and waited in a quiet, dark room the morning of the scan. An 18F-FDG emission scan extending from the base of the skull to mid thighs was obtained approximately 60 minutes after intravenous injection of 0.22 mCi/kg of 18F-FDG. Emission scans were acquired for 5 min per field of view, each covering 15 cm, at an axial sampling thickness of 3.75 mm/slice. PET images were reconstructed with CT-derived attenuation correction using ordered subset expectation maximization software. Only the maximum standardized uptake value (SUVmax) was reported, corrected for body weight.

Anterior and left lateral views of the maximum intensity projection (MIP) image of the 18F-FDG PET/CT (Discovery ST, GE Healthcare, Montreal, Canada). The large eccentric chest wall mass was moderately FDG-avid with a SUVmax of 5.4. There were no other suspicious foci of FDG uptake in the remainder of the study
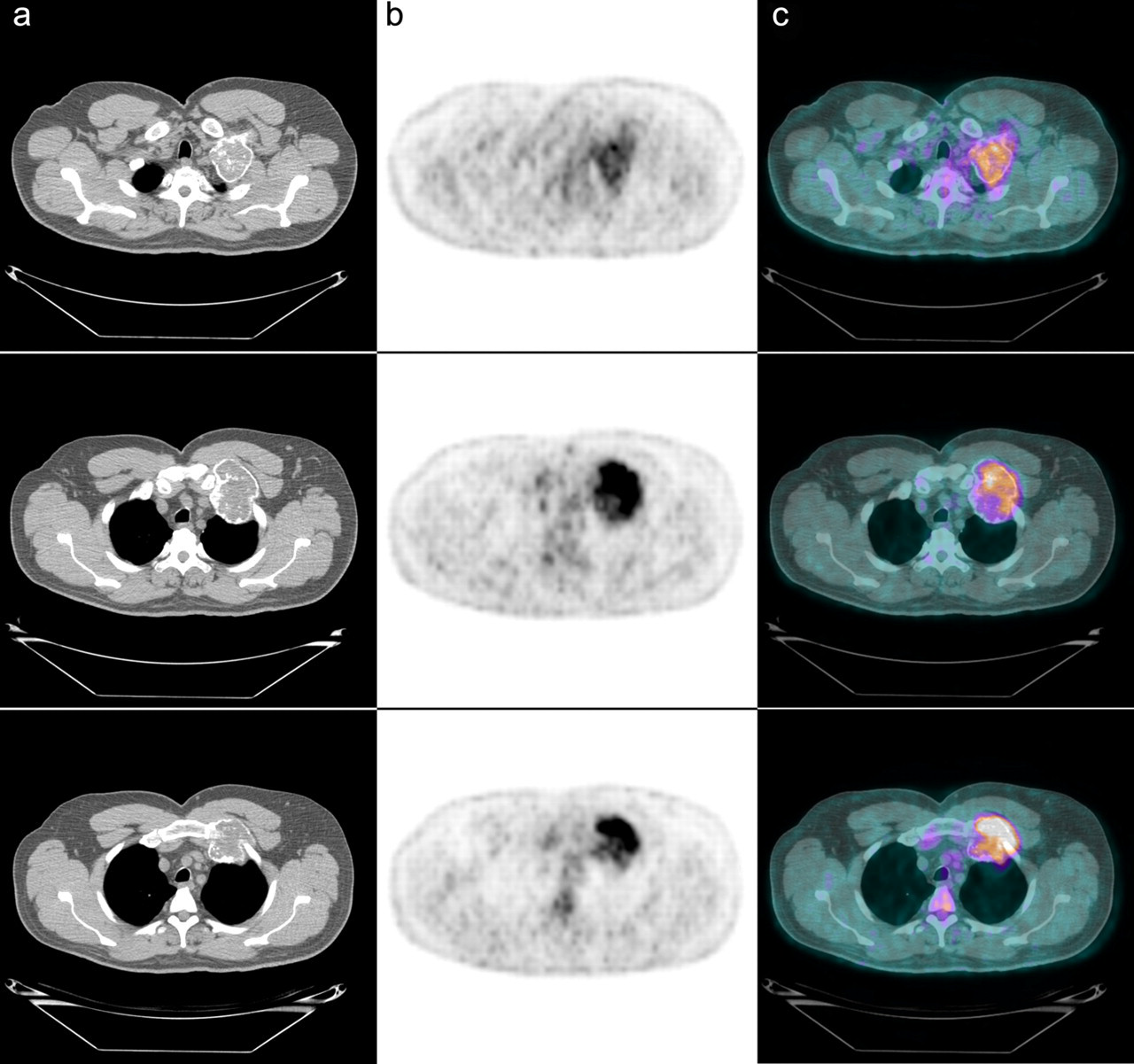
Sequential transaxial views of the chest with (a) CT portion of the PET/CT, (b) PET, and (c) PET/CT fusion images showed moderately intense FDG uptake in the diffusely calcified chest wall mass. The PET/CT was interpreted as strongly suspicious for a chondrosarcoma
The PET/CT showed a large eccentric expansile left chest wall mass arising from the first rib with significant calcification, measuring 10 cm in the maximum diameter with SUVmax of 5.4. There were no other FDG-avid abnormalities in the remainder of the scan. Based on the anatomic and metabolic findings, the PET/CT was also interpreted as strongly suspicious for a chondrosarcoma, with no evidence of FDG-avid distant metastases.
The patient had an en block resection of the first and second ribs, with distal clavicle and left upper part of the sternum. On sectioning, a 10 × 7.5 × 4.5 cm tan grey, well-defined intercostal mass was identified, extending into pericostal soft tissue but uniformly contained by a shell of reactive bone. The mass was heavily calcified with rare foci of softening cystic or myxoid changes. Focally the tumor appeared white, spongy with numerous small capillaries. There was no gross appearance suggestive of cartilage. The final diagnosis was a CMF arising from the first rib.
Discussion
Radiographic and CT imaging characteristics of CMF include the presence of a single lobular and eccentric lesion with expansion of the affected bone towards local soft tissue, cortical thinning and destruction, and a sclerotic rim (3–5). CMFs and chondrosarcomas have occasionally been mistaken for each other on diagnostic CT, as well as pathology (1, 5–7). On CT, both are locally aggressive and can have calcifications within the lesion, although calcifications in CMFs are much less common (<15% of all CMFs will show calcifications) (3, 7–9). The patients with calcifications tend to be older (mean age 46) than those without calcifications (mean age 21), and calcifications are associated with a longer duration of symptoms (average 43.2 months) compared to asymptomatic tumors (6.4 months) (10). However, the tumors differ in the type of chondroid differentiation and in genomic structure, as chromosome 6 rearrangements have been reported for chondromyxoid fibromas but not for chondrosarcomas (3).
18F-FDG PET/CT can differentiate benign from malignant bone tumors in some cases, although there is a significant overlap, especially in the mild SUVmax range (11). There are only two cases of CMF imaged with 18F-FDG PET/CT described in the literature with SUVmax ranging from 3.0–3.2, making this one of the benign bone tumors that can potentially be differentiated from a malignant bone tumor based on SUVmax alone (12, 13). There is significantly more PET/CT literature on chondrosarcomas, and although their SUVmax varies widely, values as high as 12.4 have been described (14–16). In this case, the SUVmax of the CMF was almost twice as high as previously reported in the literature and in the range known for chondrosarcomas, and the CT imaging characteristics (extensive calcification) were also suggestive of a chondrosarcoma. Only the histopathological evaluation of the excised chest wall mass revealed the benign nature of this tumor.
In conclusion, PET/CT readers should be aware of the pitfalls that arise in evaluating primary bone tumors with 18F-FDG PET/CT, and the limitations of the available literature, especially for rare tumors such as CMF.