
Abstract
Background
There are very few reports regarding the use of 3D rotational angiography (3D RA) in embolization of renal artery aneurysms (RAAs). No valuable data have been reported on the follow-up result of coil embolization for RAAs on computed tomography (CT).
Purpose
To evaluate the clinical and multidetector computed tomography (MDCT) follow-up results of renal artery aneurysms treated by detachable coil embolization using 3D RA.
Material and Methods
Six patients diagnosed with RAAs were included. Five patients underwent detachable coil embolization. Five patients underwent 3D RA and the parameters used for planning endovascular treatment obtained by 2D CT, reformatted 3D CT angiography (3D CTA), 2D digital subtraction angiography (2D DSA) and 3D RA were compared. The postembolization MDCT follow-up findings were analyzed retrospectively.
Results
The technical success rate for detachable coil embolization was 40%. The 3D CTA showed the dome-to-neck ratio (DNR) and tangential view of the renal artery aneurysm in five patients (83.3%) and the 2D CT showed it in four (66.7%). An optimal working angle assessment could not be obtained on the 2D CT and 3D CTA. The 3D RA showed the DNR, tangential view, and optimal working angle in all patients. Renal infarction occurred in three patients and postprocedural hypertension developed in two patients during the follow-up period.
Conclusion
The 3D RA was useful in preoperative determination of adequate working angle for detachable coil embolization of RAAs. Late complications of detachable coil embolization for RAAs were renal infarction and hypertension.
Renal artery aneurysms (RAAs) are rare, occurring in approximately 0.09% of the general population (1). Surgical treatment is difficult because the common location of RAAs is at the bifurcation of the renal artery near the renal hilum (1, 2). Endovascular treatment of a RAA has been reported as a less invasive and effective method used to prevent rupture of the aneurysm. However, pure coil embolization may be impossible in some wide-neck aneurysms or ones straddling arterial bifurcations. Several technical attempts including stent assisted or balloon assisted embolization have been reported as effective alternatives in such difficult circumstances (2–6).
Although endovascular coil embolization is an established treatment for RAAs, there are few data regarding the follow-up results of treated aneurysms and the involved kidneys on multidetector computed tomography (MDCT). To that end, this study was designed to investigate the usefulness of 3D rotational angiography (3D RA) in the preoperative planning of detachable coil embolization for RAAs and to describe the follow-up changes of the treated aneurysms and kidneys on MDCT.
Material and Methods
Patients and preoperative work-up
The institutional research review board (IRB) approved exemption of this retrospective clinical study and informed consent was waived by IRB. Between January 2008 and February 2010, six consecutive patients were confirmed to have RAAs on MDCT and were analyzed retrospectively. There were two male patients and four female patients and their age ranged from 45 to 62 (mean 53.6 years). The indications for treatment included symptomatic aneurysms (n = 3), and/or aneurysms larger than 2 cm in diameter (n = 4) (2). All six patients met these criteria (Table 1). The symptoms were right flank pain in two patients, and right subcostal pain and hypertension in one patient. Three asymptomatic patients had their aneurysms identified on routine healthcare evaluations; one of them had bilateral renal artery aneurysms (two in the right and one in the left kidney) and a gastroduodenal artery aneurysm. Therefore, a total of eight renal aneurysms were found in six patients.
Clinical and anatomical characteristics of the renal artery aneurysms
*Maximum diameter of the aneurysm
†Change in maxium diameter of the aneurysm after embolization
All patients underwent subsequent pretreatment imaging work up with MDCT angiography and standard 2D digital subtraction angiography (2D DSA) with the routine anteroposterior view to evaluate the possibility of endovascular treatment. Five of these patients underwent subsequent 3D RA (Allura 3D-RA Release 5/XPerCT Release 1; Philips Medical Systems, Best, The Netherlands) to obtain exact information regarding the anatomical orientation between the aneurysm neck and parent renal artery. MDCT used in CT angiography were 64-MDCT scanner (Lightspeed VCT; GE Healthcare, Milwaukee, WI, USA) and 40-MDCT scanner (Brilliance 40; Philips Medical Systems, Best, The Netherlands) with rotation time of 0.5–0.6 s, collimation of 0.625 mm × 40 to 20 mm, pitch of 0.926–1.375, tube voltage of 120 kV, and tube current of 300–370 mA. Slice thickness was 1–2.5 mm. Arterial phase was obtained when the attenuation value of ascending aorta reached 150 HU, this was determined with a bolus tracking technique
Endovascular detachable coil embolization
The endovascular detachable coil embolizations were performed by three interventional radiologists (SSW, PKB, KKH). One patient received 100 mg of aspirin one day before the procedure and two patients received 100 mg of aspirin and 75 mg of clopidogrel on the day of the procedure. Prior to coil embolization, a 2D DSA and subsequent 3D RA were obtained with a 5F angiographic catheter. With the image intensifying tube rotated to the optimal working angle (the best view of the aneurysm neck without interruption or overlapping of adjacent renal artery branches and the parent renal artery), coil embolization of the aneurysm sac was performed with initial 3D framing coil followed by 2D or 3D detachable coils through 3F Excelsior microcatheter (Excelsior 1018 microcatheter; Boston Scientific, Natick, MA, USA). Used detachable coils were Microplex (Microplex coil; MicroVention, Aliso Viejo, CA, USA), Axium (Axium detachable coil; EV3 Neurovascular, Irvine, CA, USA), Detachable (Guglielmi detachable coil; Boston Scientific, Natick, MA, USA) and Sapphire coil (Sapphire coil; Micro Therapeutics, Irvine, CA, USA). The double microcatheter technique, which has been used for the endovascular treatment of wide-necked intracranial aneurysms (7), was used in three patients.
During coil embolization, intermittent angiography was performed to confirm the compact filling of the aneurysm sac and preservation of free arterial blood flow to the segmental renal branch. The embolization was stopped when no residual contrast filled the aneurysm sac. Technical success was defined when complete occlusion of aneurysmal sac with conservation of renal artery and its branches was confirmed on completion angiography.
Preoperative image analysis and follow-up data
Two radiologists (SJM, PKB) retrospectively analyzed 2D DSA, 3D RA, and CT images side-by-side in consensus. The maximum diameter of the dome and neck, dome-to-neck ratio (DNR), visibility of the tangential view of the aneurysm neck, and predictability of the actual working angle were evaluated on the 2D CT, reformatted 3D CT angiography (3D CTA) that were reconstructed using a 3D workstation (Aquarius; TeraRecon, San Mateo, CA, USA), 2D DSA, and 3D RA. To minimize beam hardening artifacts, measurements were performed under maximum suppression of background CT density with the window and the level ranged from 14,182–15,245 (median 14,714) and from 3323–5880 (median 4602), respectively.
An aneurysm having dome-to-neck ratio <1.5 was defined as a wide-necked aneurysm (8). The DNR was defined as the maximum sac diameter divided by the maximum neck width. The maximum sac diameter was the longest diameter orthogonally directed to the longitudinal axis from the dome to the neck. The tangential view of the aneurysm neck was defined as the view that best showed the complete separation of the neck from the adjacent renal artery.
All patients were discharged one day after the embolization and their follow-up was performed in the outpatient clinic after 3 and 6 months, and then every year with postoperative MDCT. Initial maximum diameters of aneurysm sac were compared with that of final MDCT follow-up. The kidney size and defects of renal parenchymal perfusion were evaluated on the follow-up MDCT.
Laboratory data including blood urea nitrogen (BUN) and serum creatinine were recorded serially during the follow-up period. Changes of systemic blood pressure were also recorded at the initial admission and final follow-up. Mean value of three blood pressures of the preoperative day were compared with the mean value of three blood pressures obtained on postoperative day 1, midday during follow-up and at the final outpatient visit. The use of anti-hypertensive agents was reviewed.
Results
Analysis of preoperative images and endovascular treatment
The characteristics of patients and aneurysms are shown in Table 1. Five out of six patients (patients 2–6) underwent 3D RA as preoperative planning for the coil embolization. Five out of six patients (patients 1–5) underwent endovascular detachable coil embolization for the RAAs. Four patients underwent 2D DSA and 3D RA at the same day of renal artery embolization. Embolization of a RAA in one patient with co-existing gastroduodenal artery aneurysm was performed after five days from embolization of gastroduodenal artery aneurysm with 3D RA.
In one patient (patient 6), the 3D RA showed that endovascular treatment of the renal artery aneurysm was not feasible because the aneurysm neck was located at the trifurcation point of the main right renal artery into the segmental arteries (Fig. 1). This patient was discharged and underwent regular follow-up at one year with MDCT in the outpatient clinic.
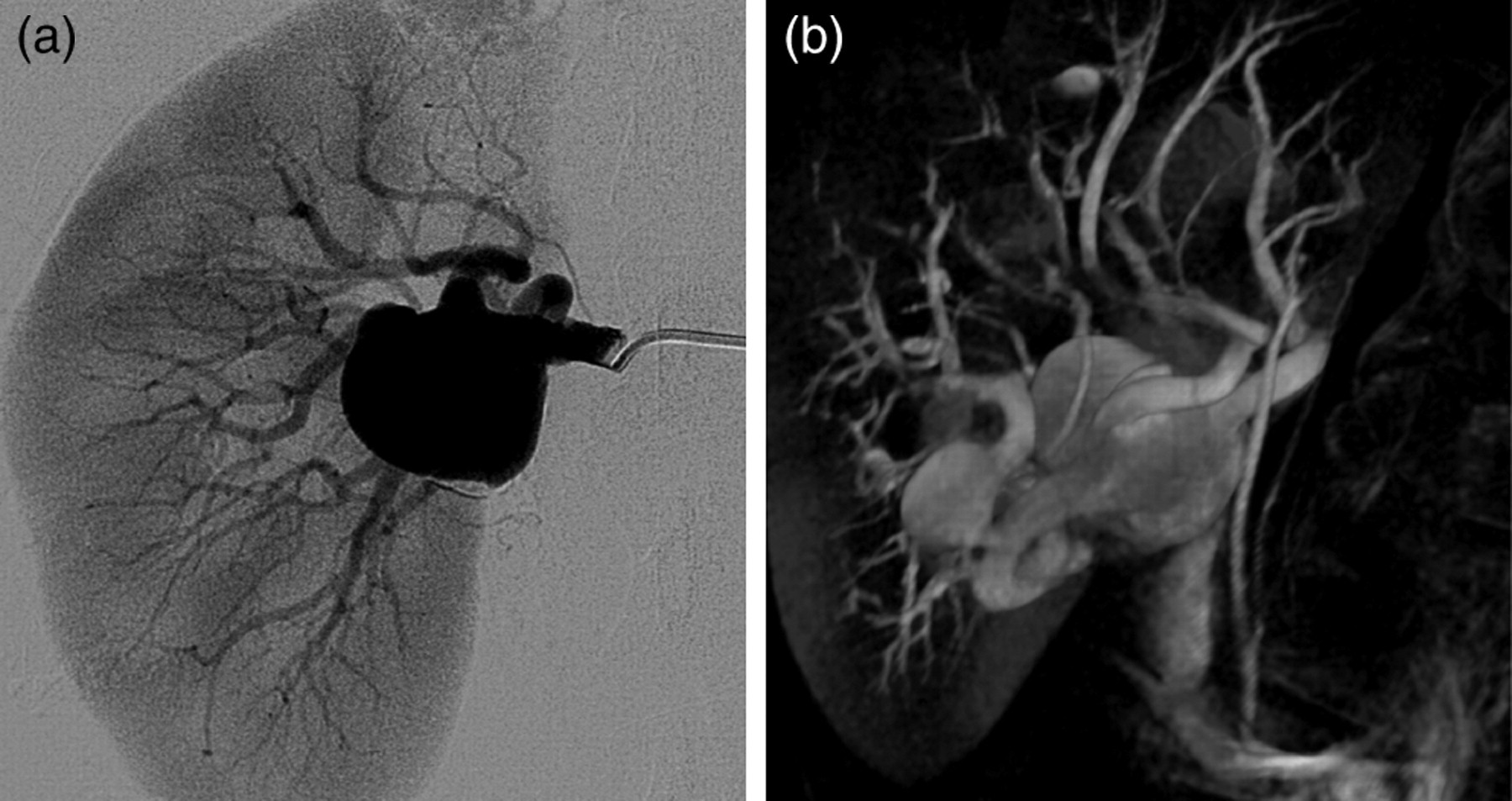
Case 6: (a) Anteroposterior 2D DSA fails to show separation of the aneurysm neck from the right renal artery; (b) 3D RA shows the wide aneurysm neck at the trifurcation of the right main renal artery
Five out of six patients (83.3%) had wall calcifications in the renal artery aneurysms. The shapes of the aneurysms were all saccular. The anatomical direction of the aneurysm sac in relation to the parent renal artery was anterior in three patients, inferior in two patients, and posterior in one patient. The location of the aneurysms was the main renal artery in one patient, main artery branch point in four patients (bifurcation in three, trifurcation in one) and segmental renal artery in one patient.
Table 2 shows a comparison of the imaging modalities used in the preoperative evaluation of the renal artery aneurysms. Although subtle motion artifacts and linear intravascular artifacts due to laminar flow were seen in three patients (3/5 patients, 60%) on 3D RA images, we had no difficulties in image interpretation and size measurements. The DNR measured by each imaging modality and their mean value are listed in Table 2. The neck diameter was not measurable in one patient by 3D CTA due to overlapping calcifications. Three aneurysms were diagnosed as wide-necked and three as narrow-necked on 3D RA. The 2D DSA revealed the DNR and tangential view of the aneurysm neck only in one patient (16.7%). The DNR and tangential view were determined by 3D CTA in five patients (83.3%) and by the 2D CT in four patients (66.7%).
Comparison of parameters in individual imaging modalities in preoperative evaluation of renal artery aneurysms
N/A = not available as not performed; – = unmeasurable
However, the postprocessed 3D RA showed the DNR, tangential view, and optimal working view in all patients that had this study (5/5 patients, 100%) (Fig. 2). The 2D DSA showed an optimal working angle in only one out of six patients (16.7%).
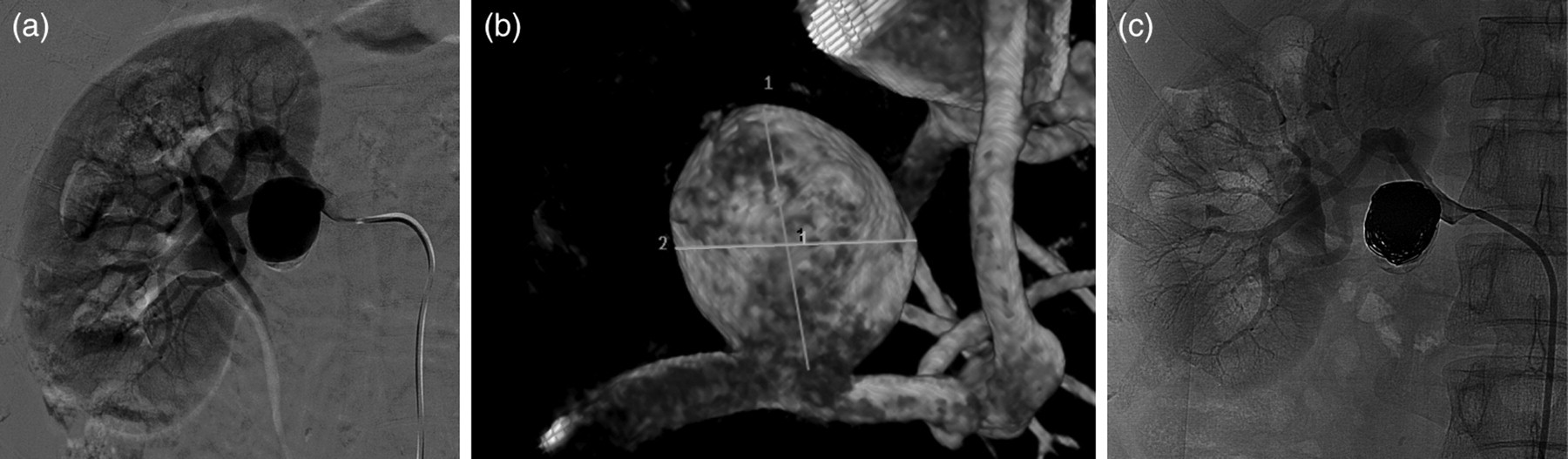
Case 3: (a) Anteroposterior 2D DSA does not show the relationship between the aneurysm neck and the renal artery; (b) 3D RA shows the aneurysm neck to be clearly separate from the renal artery; (c) Completion angiogram after coil embolization shows absence of aneurysm sac staining with preservation of renal artery flow
Technical success rate of coil embolization was 40% on completion angiography. Two patients showed complete packing of the aneurysm sac without residual contrast filling. The remaining three patients showed very subtle localized contrast filling between the coil interstices, or residual neck concavity. However, the procedure was stopped because it was deemed not possible to safely deploy any additional coils due to lack of residual dead space in the aneurysm. Involved renal artery flow was completely preserved in all patients and there were no defect in renal parenchymal staining. The number of detachable coils used ranged from 9–20 (median 14.5).
Follow-up results
The follow-up period ranged from 3–14 months (mean 8.6 months). Compared to the maximum diameter of the original aneurysmal sac, minimal aneurysmal sac diameter changes were observed with a range of –0.1 to +0.2 mm (median 0.05 mm). Persistent aneurysmal sac enhancement was not evaluable due to streak artifacts.
The mean decreases in anteroposterior and longitudinal diameters of kidney were 3.47% and 1.15%, respectively, on the final follow-up MDCT. Two patients had normal renal parenchymal enhancement and three patients demonstrated signs of chronic renal infarction (Fig. 3).
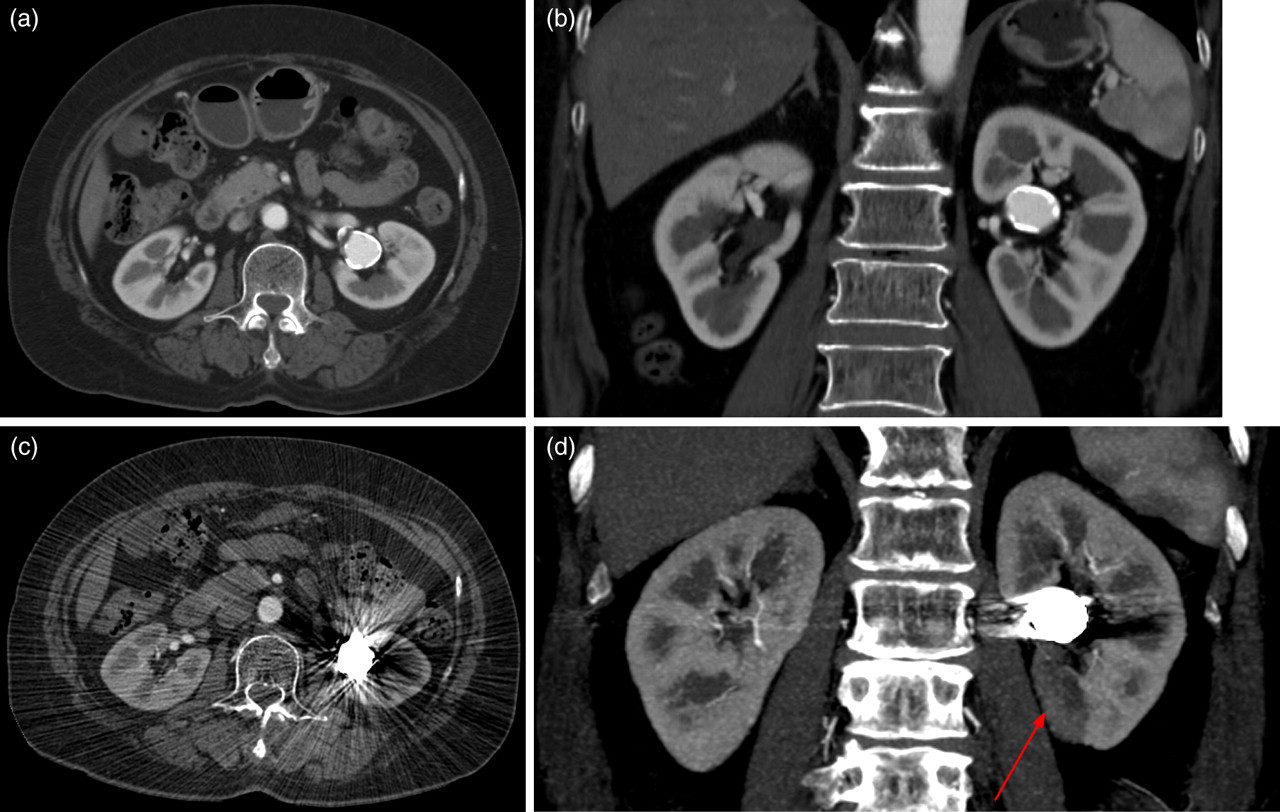
Case 1: (a) and (b) Initial axial and coronal images of MDCT show an aneurysm located anterior to the left main. Renal parenchyma appears normal; (c) and (d) Follow-up axial and coronal MDCT images 14 months after embolization demonstrated that the aneurysm is packed with coils. Imaging findings of a postero-medial chronic renal infarction are seen (red arrow)
The mean pre- and postoperative blood pressure was 118/71 and 125/73. During the follow-up period two normotensive patients (mean preoperative pressures 110/62 mmHg and 122/56 mmHg) with findings consistent with segmental infarction and diffuse cortical infarction developed postoperative hypertension (mean postoperative pressures 152/74 mmHg and 140/89 mmHg). However, another patient had normal postoperative blood pressure despite the segmental renal infarction and atrophy. Subjective clinical symptoms described preoperatively completely resolved on follow-up. The serum creatinine and blood urea nitrogen levels did not increase in any of the treated patients after short-term and long-term follow-up.
Discussion
RAAs are rare; their detection rate has been reported to be 0.3–2.5% by angiography (9, 10). Complications (rupture, hemorrhage, renovascular hypertension, renal artery thromboembolism or renal infarction) and size criteria are the main indications for therapeutic intervention (9, 11–13). Surgery has been the conventional treatment of choice for RAAs; however, endovascular coil embolization has gained acceptance as a minimally invasive treatment of RAAs (14–17). Even a wide-necked aneurysm or aneurysms at bifurcations have been successfully treated with detachable coils and various supplementary instruments such as a balloon (3, 6), a neck bridge device (4) or stent (2, 5).
In our study, planning of coil embolization was performed by neurointerventional radiologist based on 3D RA. Although wide-neck aneurysms were included in this study, embolization of RAAs was feasible with a detachable coil alone or by the double microcatheter technique. Stent assisted coil embolization of RAAs has been reported (5) and can be a reasonable technique. However, we have no long-term follow-up data for the fate of a stent in a parent renal artery, treated aneurysm, affected kidney, and clinical changes. Recent report on stent assisted coil embolization of intracranial aneurysm showed delayed stent occlusion or in-stent restenosis (18, 19). Therefore, we planned to preserve the native renal artery lumen without stent, if possible.
CT angiography performed by MDCT with its 3D reformatted images is used as a preoperative baseline diagnostic evaluation for RAA. However, CT information is insufficient to establish an endovascular treatment plan. The results of this study showed that complete separation of the aneurysm neck from the adjacent vascular structures was not possible in two patients (33.3%) with 2D CT and in one patient with 3D CTA (16.7%). To determine whether surgical or endovascular treatment is the better option for a patient, an exact evaluation of the aneurysm neck and the anatomical relationship with adjacent vessels are critical. Although, the tangential view of aneurysm neck can be estimated on the reformatted MDCT, in several cases, the acquisition of the actual working angle was not possible. Therefore, the MDCT has limitations with regard to the thorough preoperative evaluation of RAAs.
2D DSA is limited with regards to aneurysm visualization (8). In this study, the 2D DSA failed to fully show the aneurysm neck in five out of six patients (83.3%) due to the overlapping of the aneurysm neck with adjacent vascular structures. In addition, the 2D DSA requires several exposures at different angles to determine the working angle and precise anatomical evaluation of the aneurysm and adjacent vascular structures (20). However, the 3D RA, introduced in the field of neurointervention, provides an adequate working angle and neck information with a single examination. Data regarding patient radiation dose for the 3D RA used in the assessment of cerebral aneurysms showed a significantly lower peak skin dose and cumulative incident dose than with the biplanar DSA (20). Therefore, the 3D RA has definite advantages for the preoperative anatomical assessment of RAAs with the least amount of radiation exposure to the patient as well as the operator.
There is only limited information on the long-term follow-up with MDCT after endovascular treatment of RAAs. Centenera et al. reported normal blood pressure and renal function at the 3- and 6-month follow-up of their case (3). Klein et al. reported their experience with Guglielmi detachable coils in eight RAAs; successful treatment was achieved in all cases clinically and radiologically at 3- and 6-month intervals (21). Follow-up of delayed or late complications after detachable coil embolization for RAAs by angiography has not been evaluated. Embolization of the main or branch renal artery, with Gianturco coils, in cases of renal cell carcinoma, have shown several renal infarcts or sustained hypertension due to occlusion of the arterial lumen (22, 23). Segmental infarction might cause localized over-production of renin and subsequent hypertension, which is usually transient (24–27). However, in this study, even patients with complete preservation of parental renal artery flow, without any renogram defects on final angiography, showed segmental renal infarction and hypertension as a late complication. These complications are likely due to similar events that cause thromboembolic complications during detachable coil embolization of intracranial aneurysms. The frequency of thromboembolic complications, including stroke and transient ischemic attacks, has been reported to be between 3.2% and 28% (28). Dislodging of a friable plaque in the parent artery, iatrogenic dissection of a vessel, migration of a pre-existing thrombus or fresh clot within an aneurysm during coil manipulation and even metallic fragments are potential causes of thromboembolic events in the treatment of intracranial aneurysms with detachable coils (28, 29). They also reported that a tendency for an increase in the procedural complexity in combination with a longer procedural time was associated with an increase in the embolic risk (29). This tendency was illustrated in one of our cases with a large aneurysm requiring a large number of coils and the double catheter technique.
Based on our result, CT has a limitation in the follow-up evaluation for coil embolized RAAs due to beam hardening artifacts but useful for evaluation of renal parenchymal ischemic defect or shrinkage. Although aneurysm size measurement was feasible under maximum suppression of background CT density, enlarging residual aneurysm sac filling or recurred sac filling is hardly detectable by MDCT. There is no consensus for adequate imaging modality for follow-up evaluation of coiled RAAs. As seen on reports in cerebral aneurysm, volume rendering 3D RA can be a reasonable modality in follow-up of coiled RAAs (30). Further study would be needed to determine the necessity of such an invasive modality in follow-up of treated RAAs.
The limitations of this study were the small number of patient that limits statistical analysis. However, RAA is a very rare disease. Since most of previous reports concentrated on the technical success of the procedure without reporting the clinical and imaging follow-up, larger multicenter studies would be useful to further define prognosis of treated RAA. A final limitation is some heterogeneity in the imaging protocol due to an initial learning curve period needed to establish adequate protocol in our institution.
In conclusion, the 3D RA provides accurate anatomical information on RAAs with an acceptable radiation exposure; the data it provides can be used for preoperative planning of detachable coil embolization. The late complications associated with detachable coil embolization of RAAs include segmental renal infarction and hypertension.