
Abstract
Background
Whole-body diffusion-weighted imaging (DWI) has been widely used in detecting malignant metastases, including pulmonary metastases.
Purpose
To evaluate the possible utility of whole-body DWI in detecting pulmonary metastases of patients with clear cell renal cell carcinoma (ccRCC) and compare the exact differences between MR and CT in detecting pulmonary lesions.
Material and Methods
Whole-body DWI and chest CT examinations were performed on nine consecutive patients (8 men and 1 woman) with histologically confirmed ccRCC and possible metastatic lesions before chemotherapy.
Results
CT and MR demonstrated pulmonary metastases in seven patients and no metastatic lesions in two patients. The numbers of pulmonary metastases detected on CT, DWI-only, T1WI-only and DWI in combination with T1WI were 83, 35, 34 and 39, respectively. Metastases with a diameter above 1.0 cm could all be detected by DWI and a diameter above 0.7 cm could all be detected by DWI in combination with T1WI. Significant differences were obtained both for correlationship between diameter and detection rates of DWI and T1WI by using Spearman rank correlation analysis.
Conclusion
Although MR cannot be considered a replacement for CT in pulmonary metastases from ccRCC, whole-body DWI, with the combination of T1 dual echo, might be helpful for the evaluation of tumor response to chemotherapy in the follow-up of patients when the diameter of the pulmonary metastases is over 1.0 cm.
Renal cell carcinoma (RCC) accounts for about 5% of epithelial cancers worldwide. Up to 85% of these cancers are clear-cell RCC (ccRCC). Hematogenous metastasis is the main channel of metastasis in RCC and thus the lungs are the most common metastatic site in ccRCC (1, 2).
At present, computed tomography (CT) is the most effective technology for cross-sectional imaging of pulmonary lesions in clinical practice, because of its high spatial resolution and air-to-tissue contrast in the lung (3). On the other hand, magnetic resonance imaging (MRI) is generally regarded as deficient in pulmonary imaging.
However, with the recent advances in diffusion-weighted imaging (DWI) technology, the application of MRI to pulmonary imaging has become promising. First, DWI is often very sensitive to cancerous tissues because of their increased cellularity and decreased extracellular space (3-5). Thus, it could provide excellent tissue contrast. With the high contrast-to-noise ratio (CNR) of DWI, the lesions should be easily detected, even by beginners with less experience, when compared with other MR sequences. Second, breakthroughs in DWI techniques, such as parallel imaging techniques and increased gradient strengths, have significantly reduced problems with magnetic susceptibility artifacts and severe image distortion in extracranial sites (6-9). Third, DWI is able to provide functional information about the lesion, such as measurement of apparent diffusion coefficient (ADC) values. These values help monitor pathological changes during therapy even when there are no morphologic changes. In addition, now that a free breathing approach with high signal-to-noise ratio (SNR) and little image blurring has been reported in whole-body DWI (10, 11), it is time to evaluate whole-body DWI in pulmonary applications. Some applications of DWI in lung cancer have been reported (12-14), which demonstrated its feasibility in the lung. As a further step, this article is the first study focusing on the application in order to detect pulmonary metastases.
Until now, the exact differences between MR and CT in detecting pulmonary metastases have not been demonstrated. Given the ability to detect distant metastases of whole-body by DWI (15-18), this study aims to explore the possible utility of this convenient and safe examination in combination with whole-body T1 dual echo in detecting pulmonary metastases of patients with possible metastases in the whole body. We hypothesize that whole-body DWI has the potential to become an alternative choice in detecting and monitoring pulmonary metastases of patients with malignancies in the future. In all, we here for the first time evaluate the possible utility of whole-body DWI in detecting pulmonary metastases of patients with ccRCC and compare the exact differences between MR and CT in detecting pulmonary lesions.
Material and Methods
Ethics statement
The institutional review board for research involving human subjects approved the procedures. Written informed consent, in line with the Declaration of Helsinki, was obtained prior to all studies. CT was done as part of routine clinical care, while whole-body MRI (including DWI) was performed in addition as part of the approved protocol.
Patients
This was a prospective study. Nine consecutive patients who were histologically diagnosed with clear cell RCC were enrolled. They all had undergone surgical removal of the primary tumor 1-7 years earlier. They all underwent chest CT, routine T1- and T2-weighted imaging, and whole-body DWI within three days before receiving chemotherapy. There were eight men and one woman (mean age 56 years, range 40-69 years) in this study.
Chest CT protocol
Chest CT without administration of contrast media was performed with a 64-section CT system (Brilliance 64 TM; Philips Medical Systems, Best, The Netherlands). Helical scanning was performed from the root of the neck to the lowest point of the bilateral adrenal glands by using the following parameters: matrix 512 × 512, tube potential 120 kV, and tube current-time product 246 mAs, slice thickness 5 mm, display field of view (FOV) 33.5 × 33.5cm, collimator 20 mm, pitch 1.375; The reconstructed field of view was individually adjusted to encompass the heart (mean FOV 148 mm ± 22, range 121-178 mm, image matrix 512 × 512 pixels) with a section thickness of 1.0 mm (increment 1.0 mm).
Whole-body MRI protocol
Our protocol was performed with a 1.5-T MR system (Signa Excite HD; GE Healthcare, Milwaukee, WI, USA) equipped with a high-performance gradient system (19). The patients were examined in the supine position and placed feet first into the bore of the magnet using the body-coil with an automatic moving table. Two electrolytic cushions were put under the neck and upon the chest, respectively, to reduce distortion. The DW image protocol was a short T1 inversion recovery (STIR)-EPI single shot acquisition in a seven-station series (head, neck, thorax, abdomen, pelvis, thighs, and legs), with a repetition time (TR)/echo time (TE) of 4300/57.6 ms and an inversion time (TI) of 160 ms. The acquisition included a spatial/spectral selective radio frequency pulse sequence to limit excitation to the water resonance (20). Each station-series contained 39 axial slices with an FOV equal to 40 × 40 cm and a matrix size of 128 × 128 per slice during free breathing. Diffusion gradients with two b values (0 and 600 s/mm2) were applied along three directions. The slice thickness was 7 mm with a -1 mm gap and slices were acquired in an interleaved fashion at a bandwidth of 250 kHz and a number of excitation (NEX) of 4 (Table 1). Acquisition time for each series was 3.35 min with a total time of 23.45 min. Beginning with the first axial series covering the brain, the four most inferior slices were overlapped with the four most superior slices from the next series to allow flexibility in the choice of images at the edges of the FOV. From these axial DWIs, maximum intensity projection (MIP) images were reconstructed and black-white inverse grey scale was also used in all the cases. (Fig. 1).
A 46-year-old man with clear cell RCC with multiple pulmonary metas-tases. (a) A coronal view of whole-body DWI showing multiple foci of high signal intensity in the lung (arrow). (b) The coronal MIP images also showing the pulmonary metastases clearly with low signal intensity (arrow)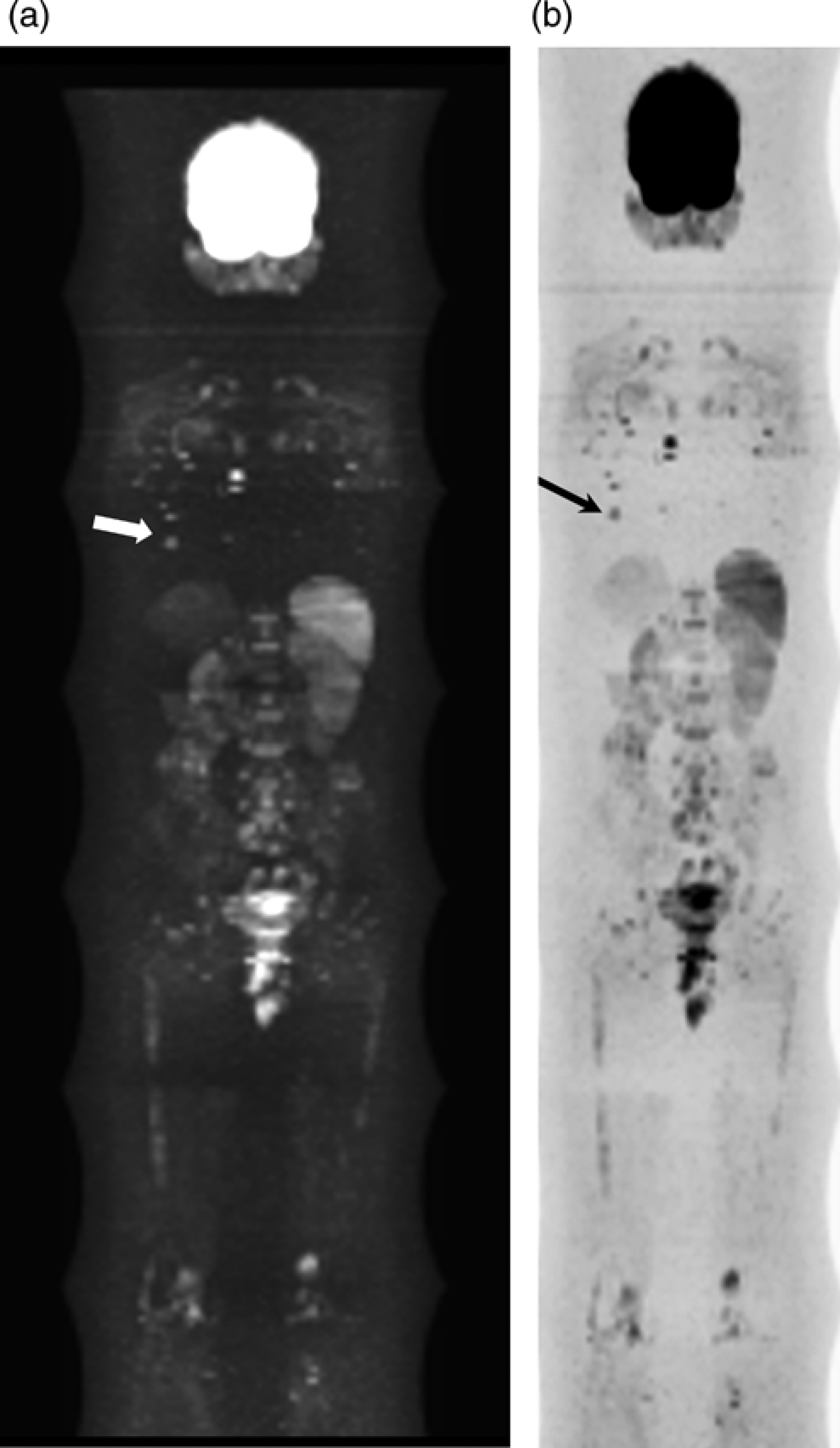
Imaging parameters of whole-body difussion-weighted MR imaging

Because DWI may cause distortion near air-tissue boundaries, whole-body T1-dual echo sequence without administration of contrast media was also acquired for each patient in order to provide an anatomical template. The images were obtained with the fast spoiled gradient-echo sequence with the following parameters: TR 180 ms, TE 4.8 ms for in phase and 2.3 ms for out phase, FA 80°, matrix 288 × 192, FOV 40 × 36 cm, slice thickness 6 mm and with no gap, bandwidth 62.5Khz, NEX 1. The breath-holding technique was used for T1 dual echo in the thorax and abdomen. The acquisition time for each series was 1.06 min with a total time of 7.42 min. The total time for a standard whole-body MR protocol was about 31 min.
Routine MR protocols
All of the patients underwent routine T1 dual echo and T2-weighted imaging in both abdomen and pelvis without administration of contrast media. T1-weighted images were obtained with the fast spoiled gradient-echo sequence with the following parameters: TR 180 ms, TE 4.8 ms for in phase and 2.3 ms for out phase, FA 80°, matrix 288 × 192, FOV 38 × 34 cm, slice thickness 6 mm with interval of 1 mm, NEX 1. T2-weighted images were obtained with the fast spin echo sequence with the following parameters: TR 6000 ms, TE 102 ms, matrix 288 × 192, FOV 38 × 34 cm, slice thickness 6 mm with interval of 1 mm, NEX 2.
Of these nine patients, one patient who was suspected to have metastasis in cervical lymph nodes underwent cervical MR examinations. The protocols included both axial T1- and T2-weighted imaging. T1-weighted images were obtained with the fast spin echo sequence with the following parameters: TR 650 ms, TE 8.3 ms, matrix 256 × 192, FOV 20 × 20 cm, slice thickness 5 mm with interval of 1 mm, NEX 3. T2-weighted images were obtained with the fast spin echo sequence with the following parameters: TR 3775 ms, TE 102 ms, matrix 256 × 192, FOV 20 × 20 cm, slice thickness 5 mm with interval of 1 mm, NEX 3.
Diagnostic standard of metastases
There were three methods in diagnosis of metastases in the lung and outside the lung: biopsy proven, morphological change on chest CT or routine MRI in follow-up after chemotherapy, and diagnosis by urologists according to history of malignancy in combination with image characteristics.
Chest CT data analysis
One radiologist (KK, with 12 years of chest CT experience) who was unaware of the patients’ clinical data and MR data evaluated the reconstructed images of chest CT data with thickness of 1.0 mm (increment 1.0 mm). Any nodule or mass detected in the field of lung or subpleura on CT would be taken into account for each patient. The diameter of each nodule was measured at three directions including axial plane and coronal/sagittal reconstructions, and the longest one was selected as the nodal diameter. All the nodules detected were sorted into different groups based on their measured diameters.
Feasibility of the DW images
Two experienced radiologists (SS and TT, with 15 and 11 years of MRI experience, respectively) assessed the quality of the DW images. Rank Score with 5 grades was adopted for assessment. Standards for each grade were as follows: 5 - excellent: no blurring, no/slight artifacts, clear visualization of lesions, detectable signal intensity of lesions; 4 -good: slight blurring, no/slight artifacts, relatively clear visualization of lesions, detectable signal intensity of lesions; 3 - moderate: slight to moderate blurring, moderate artifacts, relatively clear visualization of lesions, detectable signal intensity of lesions; 2 - fair: moderate to severe blurring, moderate artifacts, obscure visualization of lesions, detectable signal intensity of patial lesions; 1 - poor: severe blurring, moderate to severe artifacts, obscure visualization of lesions, undetectable signal intensity of lesions.
Whole-body MR data analysis
Two experienced radiologists (SS and TT, with 15 and 11 years of MRI experience, respectively) who were unaware of the patients’ clinical data, CT, and routine MR results evaluated the whole-body MR data independently. Abnormally high signal intensity on pulmonary DWI and any nodule or mass detected by T1 dual echo would suggest lesions. For evaluation of pulmonary metastases, they first evaluated only DWI results by detecting all abnormally high signal intensities on DWI without knowledge of T1WI results. Then they found their corresponding anatomical locations on T1 dual echo and chest CT, marked them, and recorded their diameters on the CT images. For evaluation of metastases outside the lung, they first evaluated the DWI results and recorded all abnormally high signal intensities on DWI, then found their corresponding anatomical locations on T1 dual echo and routine MR sequences. Thus, we could get the results of DWI-only data evaluation. Subsequently, they reviewed the whole T1WI and recorded the lesions which were not detected by DWI, and then we could get the results of DWI in combination with T1WI data evaluation. All the DW images were evaluated mainly in axial plane.
The two radiologists independently evaluated only the whole-body T1 data greater than 6 months after DWI and CT evaluation. They were also unaware of the patients’ clinical data, CT, and routine MR results before the image evaluation. Thus, we also got the results of T1WI-only data evaluation.
The two radiologists performed all measurements separately. After independent image readings, inter-observer agreement was assessed for evaluation of DWI-only, T1WI-only and DWI in combination with T1WI, respectively, and the discrepancies were resolved in a consensus reading. The results of the consensus reading were used for statistical analyses.
To explore the stability of lesions on T1W images, all the pulmonary nodules on whole-body T1WI were reviewed and measured for their maximum transverse diameters on T1WI as well as on CT at the same section of axial plane. Comparison between the diameter measurements on the two modalities was conducted.
Routine MR data analysis
One radiologist (SS, with 15 years of MRI experience) who was unaware of the patients’ clinical data evaluated the routine MR data. Any nodule or mass with abnormally high signal intensity on T2-weighted images and abnormally low or iso-intensity on T1 dual echo would suggest lesions.
Statistical analysis
Inter-observer agreement for image data analysis was assessed by the Bland-Altman plotting method (MedCalc Statistical Software, Mariakerke, Belgium) (20). The mean difference between the two observers and the 95% limits of agreement were calculated. The differences between the two observers were plotted against the mean of the two results.
Comparison between the transverse diameter measurements of pulmonary nodules on T1WI and CT was also conducted by the Bland-Altman plotting method. The mean difference between the two modalities and the 95% limits of agreement were calculated.
Spearman rank correlation analysis (SPSS 11.5 for windows) was conducted to investigate the correlation between diameter of nodules and detection rates of pulmonary metastases in DWI and T1WI.
Epicalc software was used to explore 95% confidence intervals (CI) of all the sensitivities of MR in detecting metastases.
Results
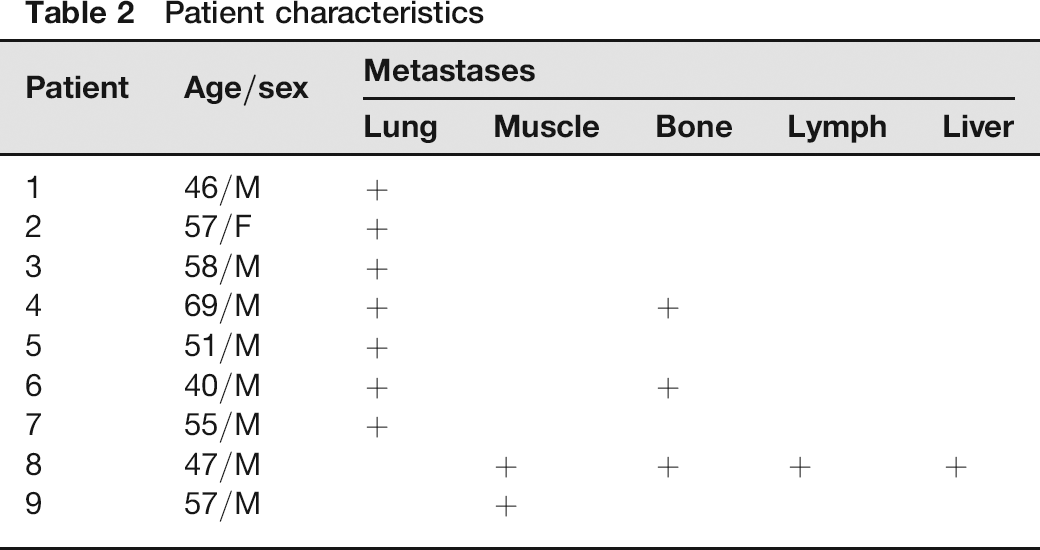
All whole-body DWI and pulmonary CT studies were completed successfully without any adverse effect. The characteristics of the patients were summarized in Table 2.
Patient characteristics
Feasibility of the DW images
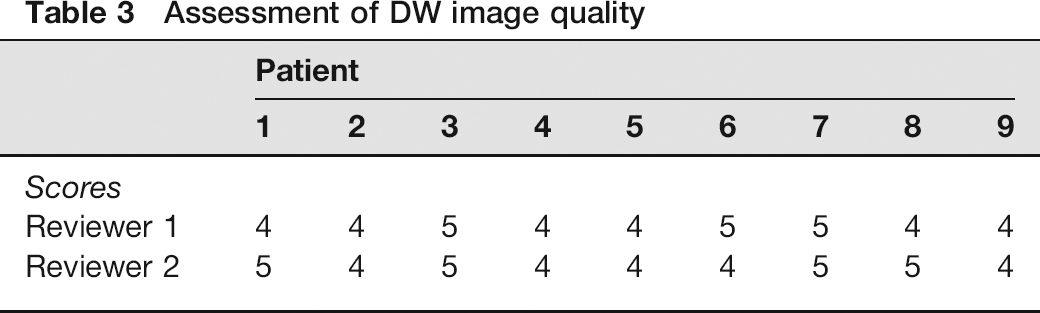
Two observers assessed all the DW images separately. The scores were concentrated in grades 4 and 5, which demonstrates that the images were generally of sufficient quality for reporting. There were no grades 3, 2, or 1 in any observer's reporting. Details of image quality assessment for each patient were in Table 3.
Assessment of DW image quality
Statistical analysis for inter-observer agreement
The mean difference between the two observers in accounting lesions on only DWI data was 0.22 with 95% limits of agreement from -1.08 to 1.53. The mean difference between the two observers in accounting lesions on only T1 data was 0.3 with 95% limits of agreement from -2.4 to 3.1. The mean difference between the two observers in accounting lesions on DWI in combination with T1 data was 0.33 with 95% limits of agreement from -1.05 to 1.72 (Fig. 2). All of the three plots showed good agreement between the two reviewers in each section of evaluation.
Bland-Altman plots of inter-observer agreements for accounting lesions on DWI-only, T1WI-only, and DWI in combination with T1WI, respectively. Solid line (center) represents mean of differences between the two observers. Top dashed line represents upper limit of agreement (mean difference plus two times standard deviation); bottom line represents lower limit of agreement (mean difference minus two times standard deviation). (a) is for agreement of DWI-only evaluation (mean difference = 0.22, 95% limits of agreement -1.08 to 1.53); (b) is for agreement of T1WI-only evaluation (mean difference = 0.3, 95% limits of agreement -2.4 to 3.1); (c) is for agreement of DWI in combination with T1WI evaluation (mean difference = 0.33, 95% limits of agreement -1.05 to 1.72)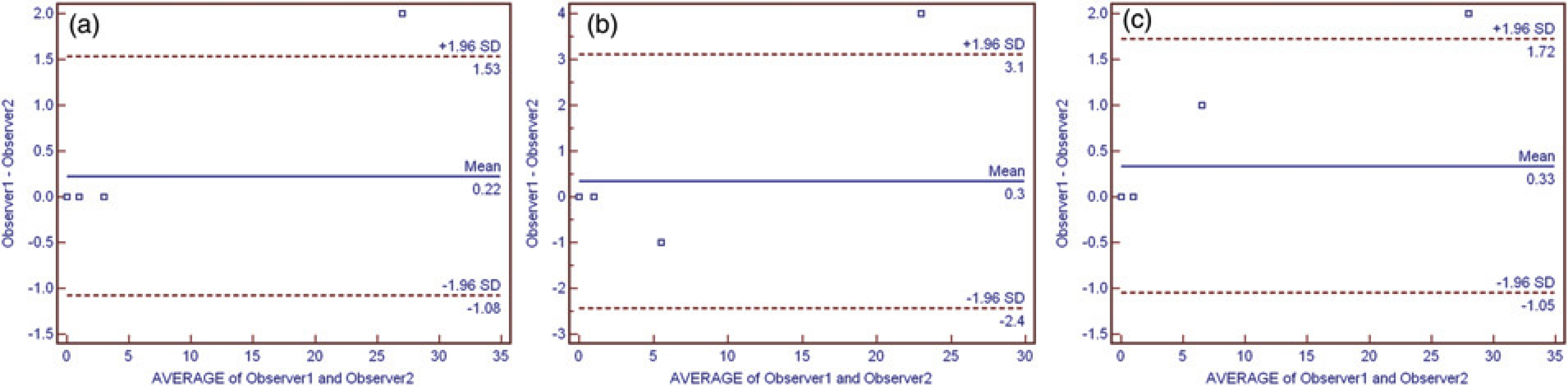
Pulmonary metastases
All of the nodules detected by chest CT were diagnosed as metastases by urologists according to the diagnostic standard mentioned before. Most of the metastases found on CT appeared as focal, well-circumscribed, and soft tissue-like densities. The metastases detected by DWI showed high signal intensity with slight deformation (Fig. 3). There was not any image blurring on T1WI images and the lesions all showed isointensity. In our study, none of these lesions had apparent calcifications on CT. Most of them appeared as homogenous, well-defined nodules with diameters below 1.0 cm, only one patient which was shown to have a solitary, large (about 8.4 cm in diameter) and irregular mass with necrosis. Multiple nodules (above 10) were also found in two patients.
A 58-year-old man with clear cell RCC with focal pulmonary metas-tases. (a) An axial view of DWI showing a focus of high signal intensity sub-pleura (arrow); (b) An axial view of T1 dual echo showing a focus of isointensity subpleura at the same anatomical region (arrow); (c) An axial view of CT showing the pulmonary metastases clearly with 0.6 cm of the size measured at the same anatomical region (arrow)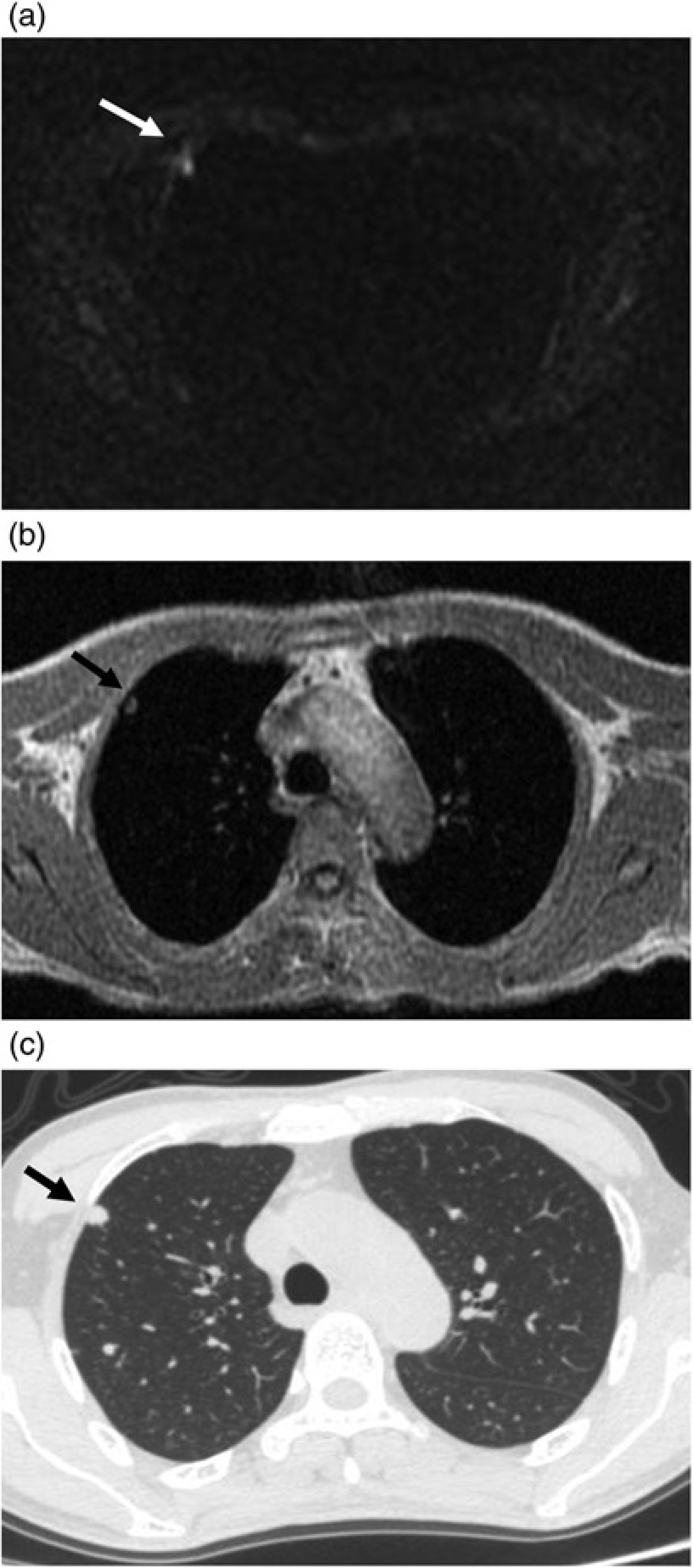
CT demonstrated pulmonary metastases in seven patients and showed normal in the other two patients. A total of 83 foci were detected by CT. Among these foci, DWI alone, T1WI alone, and DWI in combination with T1WI detected 35 (42.2%), 34 (41%) and 39 foci (47%), respectively. Thus, the sensitivity of T1WI only is the lowest while the sensitivity of DWI in combination with T1WI is the highest. Additionally, all the nodules detected on DWI could be found on T1WI when using analysis of DWI in combination T1WI. No focus which was not depicted by CT showed positive on DWI or T1WI in this study.
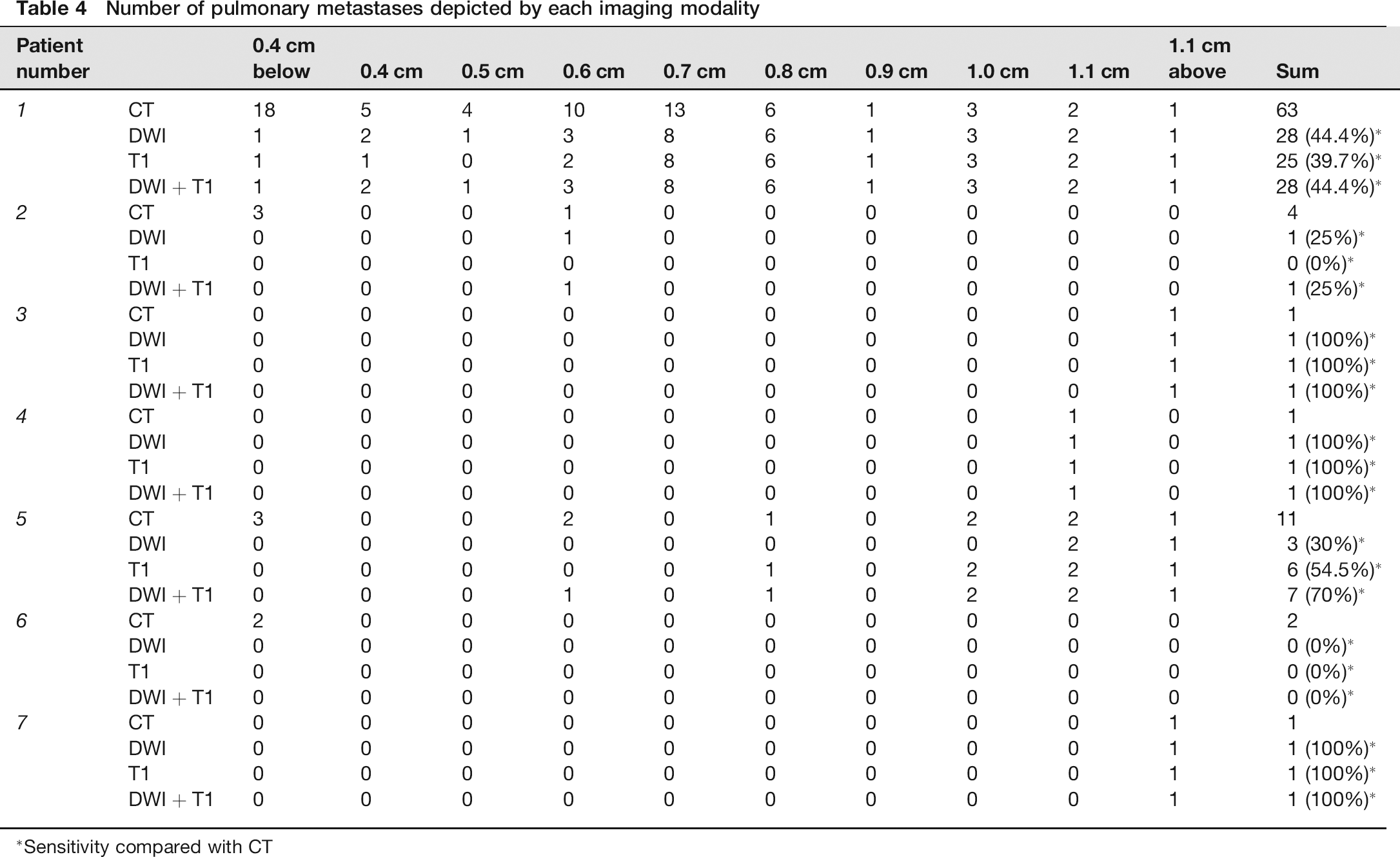
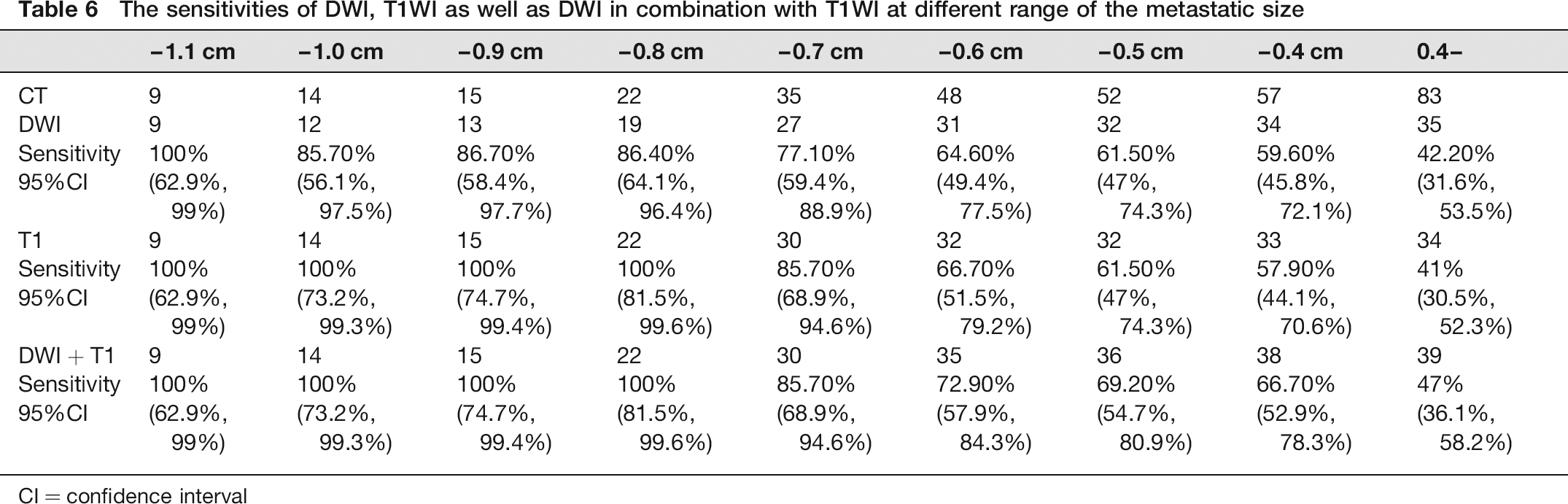
The mean diameter of these 83 nodules on CT was 0.43± 0.26 cm (range 0.1-8.4 cm). The details are summarized in Table 4. The smallest diameter of the metastases detected by either DWI or T1WI was 0.3 cm. The detection rate of either DWI or T1WI goes up as the diameter of lesion increases (Table 5 and Fig. 4). When the diameter is above 0.6 cm, the sensitivity exceeds 60% for both DWI and T1WI. When the diameter reaches 0.8 cm or above, the detection rate exceeds 85% for DWI and reaches 100% both for T1WI and the combination of DWI and T1WI (Tables 5 and 6). Additionally, 95% CI of sensitivities for each MR protocol in detecting pulmonary metastases are also listed in Tables 5 and 6.
Chart of detection rate of DWI-only, T1WI-only and DWI in combination with T1WI in detecting pulmonary metastases at each diameter range compared with chest CT. The chart illustrates the change trend of detection rate of MR with pulmonary nodules growing in size. X axis stands for the diameter of pulmonary nodules. Y axis stands for detection rate of MR with chest CT as standard. Each point on the curve chart stands for each detection rate at each diameter range. Note point A: the first point of detection rate of T1WI and DWI in combination with T1WI reaching 100%; Note point B: the first point of detection rate reaching 100%; Note point C: the point of detection rate of DWI not reaching 100% when the diameter exceeding 0.9 cm
Number of pulmonary metastases depicted by each imaging modality
Sensitivity compared with CT
Sensitivity of DWI, T1WI as well as DWI in combination with T1WI in detecting pulmonary metastases compared with CT
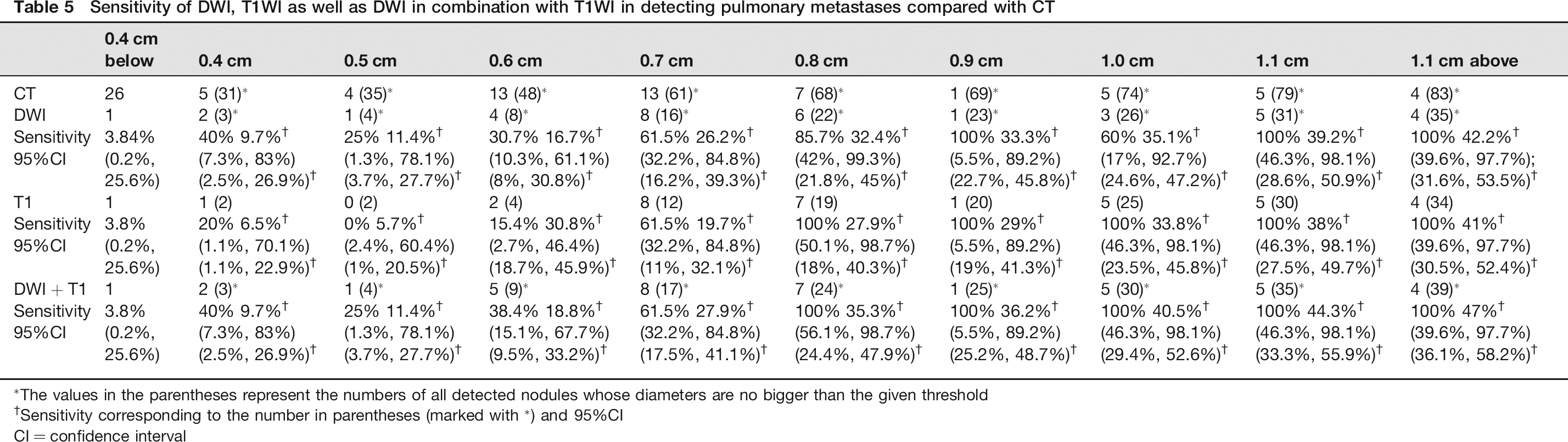
The values in the parentheses represent the numbers of all detected nodules whose diameters are no bigger than the given threshold
Sensitivity corresponding to the number in parentheses (marked with *) and 95%CI
CI = confidence interval
Metastases outside the lung
Abnormal signal intensity was detected in bone (3 cases), muscle (1 case), cervical lymph nodes (1 case), and liver (1 case) by routine MR protocols (Table 2). Metastases were confirmed in bone, muscle, and lymph nodes while suspected metastasis was diagnosed in liver lesions by clinician.
All of these metastases and suspected metastases showed high signal intensity on whole-body DWI and slight hypointensity on whole-body T1WI, which have shown that the sensitivity of both DWI and T1WI in detecting metastases outside the lung could reach 100% when compared with routine MR protocols. No metastasis which was not depicted by routine MR showed positive on DWI or T1WI in this study.
Statistical analysis for diameter measurements
Thirty-nine foci were detected by T1WI during analysis of DWI in combination with T1WI. Most of them showed iso-intensity without deformity and distortion, but due to artifact near the mediastinum, five of the foci were affected in diameter measurement and excluded. Thus, comparison between the transverse diameter measurements of pulmonary nodules on T1WI and CT was conducted in 34 foci. The mean difference between the two modalities in measuring lesions was 0.04 cm with 95% limits of agreement from -0.19 to 0.26 (Fig. 5).
Bland-Altman plots of comparison between the transverse diameter measurements of pulmonary nodules on T1WI and CT. The mean difference between the two modalities in measuring lesions was 0.04 cm with 95% limits of agreement from -0.19 to 0.26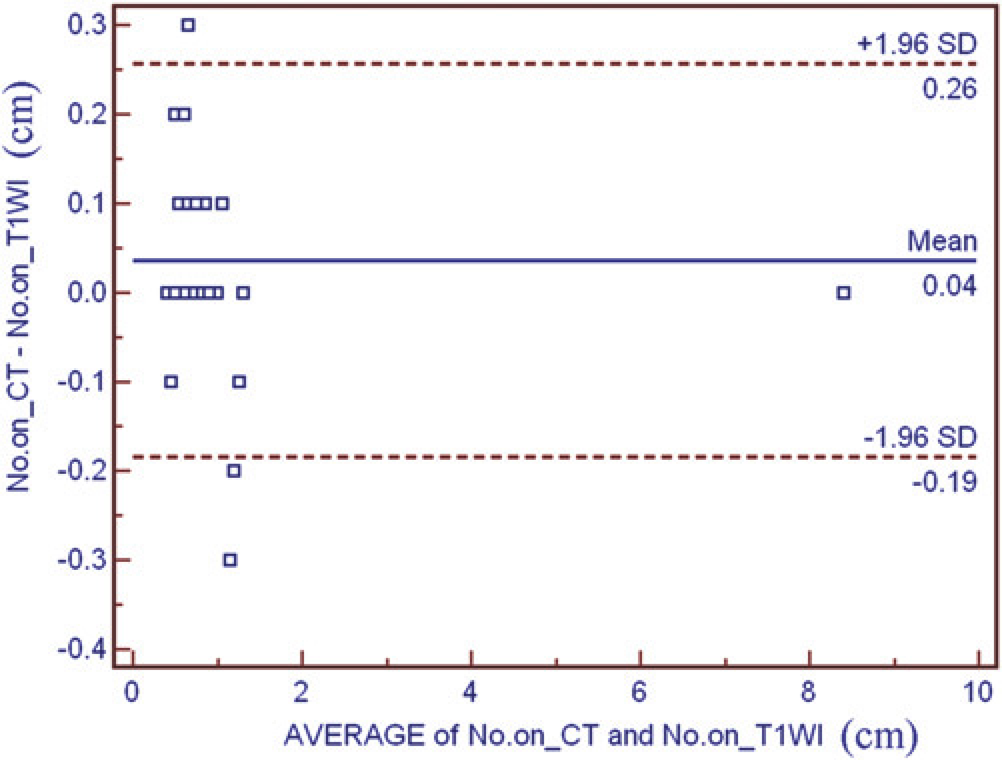
Correlation analysis between nodular diameter and detection rates of MR
Spearman rank correlation analysis (SPSS 11.5 for windows) was conducted to investigate the correlation between diameter of nodules and detection rates of DWI alone, T1WI alone and DWI in combination with T1WI in detecting pulmonary metastases, respectively. Significant differences were obtained for them (significances were set at two-tailed P values of 0 for all of them, with correlation coefficients of 0.865, 0.873 and 0.899, respectively).
It is notable that all statistical analyses above were carried out in seven patients with positive lesions.
Determine the cut-off values
In our study, the smallest lesion diameter that could be detected by either DWI or T1WI in the lungs was approximately 0.3 cm. So, we set 0.3 cm as the totally undetectable cut-off value for the diameter of tumor; a 1.0 cm diameter was also set as the totally detectable cut-off value for DWI-only because 100% of the metastases above 1.0 cm can be detected; 0.7 cm was defined as the totally detectable cut-off value for T1WI-only and DWI in combination with T1WI for the same reason; The range of 0.3-1.0 cm was defined as possibly detectable areas for DWI-only, and the range of 0.3-0.7 cm was defined as possibly detectable areas for T1WI-only and DWI in combination with T1WI (Table 7). The detection rate is higher with larger diameters for all of them Tables 5 and 6).
The sensitivities of DWI, T1WI as well as DWI in combination with T1WI at different range of the metastatic size
CI = confidence interval
Cut-off values of nodular diameter
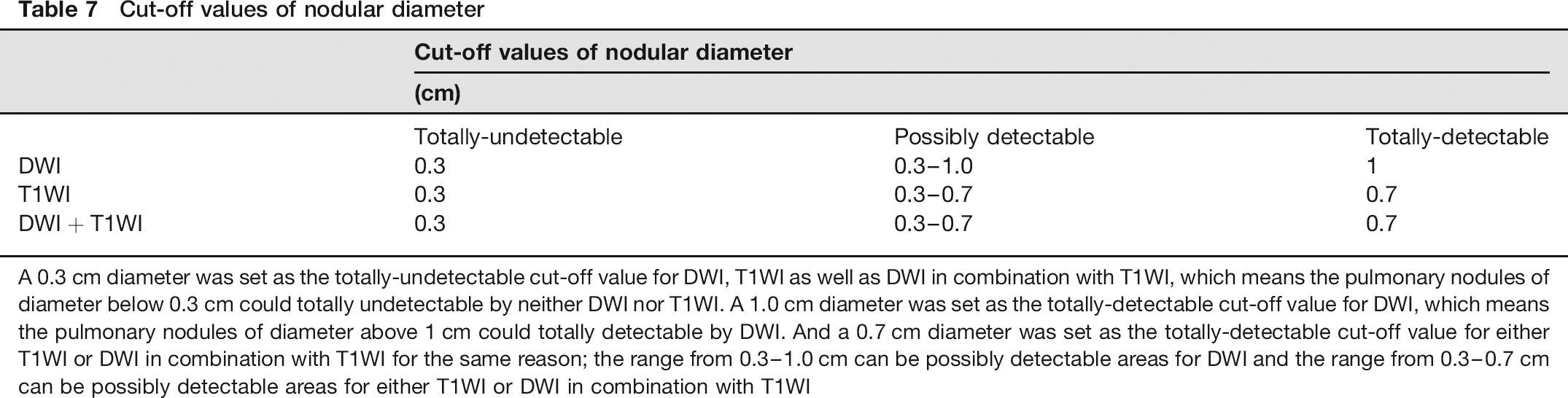
A 0.3 cm diameter was set as the totally-undetectable cut-off value for DWI, T1WI as well as DWI in combination with T1WI, which means the pulmonary nodules of diameter below 0.3 cm could totally undetectable by neither DWI nor T1WI. A 1.0 cm diameter was set as the totally-detectable cut-off value for DWI, which means the pulmonary nodules of diameter above 1 cm could totally detectable by DWI. And a 0.7 cm diameter was set as the totally-detectable cut-off value for either T1WI or DWI in combination with T1WI for the same reason; the range from 0.3-1.0 cm can be possibly detectable areas for DWI and the range from 0.3-0.7 cm can be possibly detectable areas for either T1WI or DWI in combination with T1WI
Discussion
Given the radiation exposure, CT poses considerable health hazards for people undergoing frequent examinations. Making appropriate choices about CT use is important both for the clinicians and patients, and searching for a safer examination is desirable, especially in this population. Several studies have reported the application of MR to pulmonary imaging (12-14). Though these are still in the initial phases - as in our study - this preliminary research could inspire additional work and form the foundational concepts for more definitive work.
As a whole-body imaging tool, DWI has the dual advantages of detecting distant metastases and providing functional information about lesions (21-23). Compared with bone scintigraphy and positron emission tomography (PET)/CT, whole-body DWI has no significant radiation exposure concerns. In addition, performance on only one machine is convenient when compared with PET/CT. Thus, it has found particular utility in tumor staging and treatment monitoring, such as in lymphoma (19, 21). It may also have potential in staging ccRCC in the future. Though lung is the most common metastatic site of ccRCC (1, 2), metastases to other sites are not rare (24). In our study, in addition to pulmonary metastases, whole-body DWI detected all extra-pulmonary lesions that were detected by conventional T1- and T2WI. And these metastases were confirmed by either biopsy proven or follow-up of MR protocol. False-positive metastases on whole-body DWI were not observed in this study.
Selection of the optimal b values for diffusion-weighted MRI is important for assessment of metastases. It has been reported (25) that if the b value is low, such as 100 s/mm2 and 300 s/mm2, the SNR of the DW images and CNR of the lesions are relatively good but the ADC values will be impacted heavily by the perfusion effects of blood flow. However, if the b value is high, such as 1100 s/mm2, SNR of the DW images will be reduced, especially for the organs which have relatively short TE such as liver. Thus, the optimal selection could be relatively high b value with sufficient SNR of the DW images. It is not very easy to select the optimal b value for imaging the whole-body, but the image quality assessed in this study with b value of 600 s/mm2 gained relatively high scores, which has demonstrated that the whole-body DWI protocol was feasible for data analysis.
DWI has the ability to highlight lesions and the concurrent whole-body T1 dual echo could be complementary for the anatomical location. Although it is not recommended to measure the sizes of lesions on DWI due to imaging deformation, it is also noteworthy that the lesions on both CT and T1WI were seen as stable without deformity and distortion and the diameters measured on T1WI were almost the same as with CT (Fig. 5). Thus, whole-body T1 dual echo is a fairly good supplement to whole body DWI not only for anatomical location, but also for lesion size measurement.
Nonetheless, it is still of interest to perform DWI in the lung instead of T1WI. Besides the characteristics of highlighting lesions and providing functional information which have been introduced before, the analysis in our study showed that the inter-observer agreement was best for evaluation of DWI-only data. There were four foci which showed positive at DWI while negative at T1WI-only. These foci with diameters below 0.7 cm were concentrated in the patient with multiple pulmonary metas-tases. That may indicate that the CNR of the lesions at T1WI is relatively low. There were five foci which showed negative at T1WI-only while positive at DWI in combination with T1WI (Fig. 6). The missing focus was due to unware of history of metastases and DWI data.
A 40-year-old man with ccRCC with focal pulmonary metastases. (a) An axial view of DWI showing a focus of high signal intensity at the left lung field (arrow); (b) An axial view of T1 dual echo showing no focus of obvious nodular appearance at the same anatomical region, which suggests negative at T1WI; (c) An axial view of CT showing the pulmonary metastases clearly with 0.6 cm of the size measured near the descending aorta at the same anatomical region (arrow)
Although CT shows its superiority in detecting small pulmonary metastases, we have also found that if the diameter of pulmonary metastasis is large enough, then tumors can be consistently and safely detected by the combination of DWI and T1WI (Fig. 4), a concept which has not been introduced before. In addition, significant correlations between the diameter of the nodules and detection rates in DWI and T1WI have been obtained from the statistics. In our study, the totally detectable cut-off values is 1.0 cm for DWI-only, and 0.7 cm for T1WI-only and DWI in combination with T1WI (Table 7). These cut-off values mean that whole-body DWI may be an alternative choice in monitoring treatment response of the pulmonary lesions which are big enough. We are therefore interested in exploring in detail the cut-off values of totally detectable and totally undetectable pulmonary nodules.
We speculate that the cut-off values might be correlated with the slice thickness and slice gap. After being reconstructed, the slice thickness of CT is 1 mm with no gap. As a result, it is reasonable to believe that the smallest diameter detected is 0.1 cm by CT in our study. Moreover, we assume that some metastases could be missed using DWI or T1WI for the same reason. Thus, reducing slice thickness with minimal prolongation of scanning time and increasing the matrix for improving SNR might be helpful in evaluating the detection rate of DWI in pulmonary lesions.
However, there were only nine nodules with diameters above 1.0 cm. DWI detected all of them, but the lower limit of 95% CI was only 62.9%) (Table 6). The main reason is considered to be the small sample capacity. Therefore, a diameter of 1.0 cm as the cut-off value of DWI in detecting pulmonary metastases should be further proven by increasing in sample capacity especially the nodules above 1.0 cm. Additionally, the lower limit of 95% CI of sensitivity of T1WI in detecting nodules above 0.7 cm is 81.5% (Table 6). It is a little higher than the one of DWI, but further study is still needed.
There are several limitations in this study. First, not all pulmonary metastatic lesions have been pathologically confirmed. However, with three experienced radiologists interpreting the CT and MR images, the follow-up of these patients under chemotherapy showed that all of them showed changes in their pulmonary nodules after starting treatment consistent with malignancy of the nodules. Second, the number of the patients in this study is quite limited. Though the number of pulmonary nodules is of adequate amount, all of these nodules were detected and analyzed in only seven patients. Thus, cluster bias exists in this study, and more cases should be enrolled in further study. Finally, the initial results were based on clear cell RCC metastases and more studies are required to extend this method to other malignant tumors.
However, the totally detectable cut-off value of DWI is higher than the slice thickness. From Table 7 and Fig. 4, we found that there is one missing nodule at diameter 0.8 cm and two nodules at diameter 1.0 cm. These missing metastases are mainly from the low lobes of the lung, which are close to the diaphragm. This may be due to image blurring caused by the periodic displacement of the diaphragm, which is the disadvantage brought by free-breathing applied in DWI. Some studies (6) suggested that the Tracking Only Navigator (TRON) technique may adequately deal with this problem. Data acquired during the entire breathing cycle can be used for image formation in this technique, but it is only used to track and correct for displacements in liver (26). The performance of this promising tool still needs to be investigated in the lung.
In conclusion, although MR cannot be considered an adequate replacement for CT in pulmonary metastases from ccRCC, whole-body DWI in combination with T1 dual echo might be helpful for the evaluation of tumor response to chemotherapy for the follow-up of the metastases in the whole body when the diameter of the pulmonary metastasis is over 1.0 cm.
Footnotes
Acknowledgment
We would like to thank all the volunteers participated in this study. Acknowledgment is also made to Dr Hua Zhong and Alexander Merkle, MD for their literal corrections to this paper. Additionally, we would like to thank Ms Xueying Li for her support in statistics.
None