
Abstract
Background
Persistent primitive trigeminal artery (PPTA) is the most common permanent carotid-basilar anastomosis. Magnetic resonance angiography (MRA) has become the primary non-invasive imaging technique for evaluation of cerebral vascular anatomy and can provide detailed 3D imaging of intracranial vessels.
Purpose
To evaluate the usefulness of MRA for the detection of PPTA and to re-classify its variations based on the embryologic types of PcomA and its relationship with the basilar artery and its branches.
Material and Methods
Of the total 7329 patients who underwent MRA at our institution from March 2008 through November 2010, we retrospectively analyzed the MRAs of 24 patients with a PPTA. Special attention was given to defining the relationship of the PPTA and the basilar artery with PcomA and to determine the site of origin, size, and course of the PPTA. The PPTA classification included five types based on their anatomic relationship to the neighboring arteries. Clinical features and associated vascular anomalies are also described.
Results
Twenty-four (17 women and seven men, 34 ~ 81 years of age, mean age 59.67 years) of the 7329 patients had a PPTA (0.33 %). Eleven cases (45.8%) were classified as type 1, three (12.5%) as type 2, five (20.8%) as type 3, one (4.2%) as type 4, and four (16.7%) as type 5b. Fifteen PPTAs (62.5%) were located on the left side and nine were located (37.5%) on the right side. The basilar artery proximal to the insertion of the PPTA showed severe to moderate hypoplasia in 13 cases (54%). Nine intracranial artery aneurysms were detected in seven (29%) of the 24 study patients.
Conclusion
This study revealed five types of PPTA and necessitates an adjustment of the previous classification of PPTA on the basis of our MRA examinations. A PPTA should be considered by both the clinician and the radiologist who interpret MR angiography.
Keywords
Understanding possible variations in the normal vascular anatomy, particularly with respect to persistent embryonic vessels, is necessary in order to understand the mechanisms of cerebrovascular diseases and to develop optimal treatment plans. Primitive embryonic anastomoses, including those of the trigeminal, hypoglossal, and proatlantal inter-segmental arteries, are temporary communicating arteries between the developing internal carotid and basilar arterial systems during the embryonic period. Among these embryonic, carotid-basilar anastomoses which can remain into adulthood, the persistent primitive trigeminal artery (PPTA) occurs most frequently with an incidence of 0.06 ~ 0.6% (1-3).
Saltzman classified the angiographic appearance of PPTA into three types, i.e. types 1, 2, and 3 (4). There may, however, still be some confusion regarding type 3, which was originally described as a mixture of types 1 and 2, as some authors have also described some PPTA variants which terminate at three different cerebellar arteries as type 3 (4-6). As these types differ in that the one, so-called mixed type of types 1 and 2 is connected to the basilar artery while the other, the so-called PPTA variants, is not, considering these two different variations as type 3 may be inappropriate. Furthermore, we encountered a case that did not meet the Saltzman classification and which thus made it complicated for us to understand the various types of PPTA. Therefore, we considered that re-evaluating the PPTA is necessary in order to clarify and simplify its classification.
Magnetic resonance angiography (MRA) has become the primary and most popular non-invasive imaging technique for evaluation of cerebral vascular disease and can provide 3-dimensional (3D) imaging of intracranial vessels in detail without arterial catheterization. The purposes of this study were to evaluate the usefulness of MRA for the detecting the PPTA as well as emphasizing its anatomical vascular relationships and to classify any possible variations in order to obtain a comprehensive understanding of the PPTA based on both the embryologic types of the posterior communicating artery (PcomA) and its relationship to the basilar artery and its branches.
Material and Methods
Patients and the MRA technique
Between March 2008 and November 2010, cerebral MRA was performed on a total of 7329 patients (3322 men and 4007 women) aged 1-97 years (average age 58.3 years) in a tertiary-referral, university hospital. MRA was performed on either a 3.0 T system (Intera Achieva; Philips, Best, The Netherlands) or a 1.5 T system (Achieva; Philips, Best, The Netherlands) using an 8-channel-sensitivity-encoding (SENSE) head coil or a 16-channel-SENSE Neurovascular (NV) head coil. TOF-MRA was obtained using 3D T1-weighted fast field echo (3D-T1-FFE) sequences with TR/TE 29/3.9, flip angle 20°, field-of-view (FOV) 210 × 190 × 96, matrix 600 × 272, and acquisition time of 5 min 45 s with the 3.0 T system. TOF-MRA was obtained using 3D T1-weighted fast field echo (3D-T1-FFE) sequences with TR/TE 25/6.9, flip angle 20°, field-of-view (FOV) 200 × 200 × 102, matrix 500 × 250, and acquisition time of 6 min 33 s with the 1.5 T system. Parallel imaging was performed using a generalized, autocalibrating, partially parallel acquisition algorithm based on autocalibration of the simultaneous acquisition of spatial harmonics and parallel acquisition. The acquired image data-sets were then transferred to a workstation (EWS 2.6.1, Philips Medical Systems, Best, The Netherlands) where the 3D images were reconstructed using a 1024 × 1024 matrix by maximum intensity projection (MIP) and volume rendering (VR) using a special 3D software package.
Classification of the PPTA
The classification of PPTA was made based on its course, the termination, and the morphology of the neighboring blood vessels on the 3D-TOF-MRA. The PPTA classification is shown in Fig 1. For Type 1, the PPTA is the main supply of the distal basilar artery, posterior cerebral artery, and superior cerebellar artery territories (as with the Saltzman type 1). The portion of the basilar artery that is proximal to the PPTA insertion may be hypoplastic and the PComA is absent. This type has the adult type of both posterior cerebral arteries. For Type 2, the PPTA is the main supply of the superior cerebellar artery territories, and the posterior cerebral arteries receive their blood supply predominantly through the patent PComA (as with the Saltzman type 2). This type has the fetal type of both posterior cerebral arteries. Saltzman described another type which he indicated to be a combination Types 1 and 2; some authors have described this as Type 3 PPTA as the contralateral posterior cerebral artery is supplied by the PPTA and the ipsi-lateral posterior cerebral artery receives its blood supply via anterior circulation of the PComA. As we treated a case in which the contralateral side of the posterior cerebral artery received its blood supply via anterior circulation of the PComA, we considered these variations as types 3 and 4, respectively. There are other reported types of PPTAs, so-called PPTA variants, which terminate at three different cerebellar arteries including the superior cerebellar artery, anterior inferior cerebellar artery (AICA), and posterior inferior cerebellar artery (PICA). Some authors have classified this as Saltzman Type 3, although Saltzman did not describe this type in his study (4-6). We considered this type as Type 5 and further subclassified it according to the terminating arteries, i.e. when the terminating artery is the superior cerebellar artery, Type 5a; the AICA, Type 5b; and the PICA, Type 5c. This subclassification was adapted from that of Ali et al. (5).
There are five types of persistent primitive trigeminal artery (
Image analysis
The MRA images were retrospectively analyzed by two radiologists with consensus and the PPTA was classified according to our new classifications. Our institutional review board approved this study. Special attention was given in defining the relationship of the PPTA to the basilar artery, the PcomA, the site of origin of the PPTA relative to the internal carotid artery, and the size of the PPTA, as well as its course. We also assessed the presence and degree of hypoplasia of the proximal basilar artery, i.e. none, mild, moderate, or severe according to the size of the basilar artery proximal to the connection of the PPTA compared to the basilar artery distal to the connection. Clinical configurations and associated vascular lesions, including aneurysms, arteriovenous malformation (AVM), and a vascular stenosis or occlusion, were also described. Four patients who had PPTA underwent digital subtraction angiography (DSA) to treat ischemic stroke or aneurysms.
Results
Prevalence and sex distribution of the PPTA
Among the 7329 patients who underwent MRA, 24 patients (34 ~ 81 years of age, mean age 59.67 years) had a PPTA; the total occurrence was 0.33%. Among these 24 patients (seven were men [29%]), the occurrence of PPTA in male study patients was 0.21% (7/3322). As the remaining 17 patients were women (71%), the occurrence of PPTA in female study patients was 0.42% (17/4007). PPTA was an incidental finding in all 24 patients during MRI and MRA evaluation for headache (n = 12), focal neurologic symptoms (n = 3), dizziness (n = 6), resting tremor (n = 1), transient ischemic attack (n = 1), or visual disturbance (n = 1). Three patients with focal neurologic symptoms and one of the six patients with dizziness showed acute cerebral infarction in the right corona radiata, the pons, the medulla, and the insular cortex. One patient with visual disturbance had a meningioma involving the cavernous sinus (Table 1).
The clinical features and imaging findings of patients with persistent primitive trigeminal artery (PPTA)
A meningioma involving the cavernous sinus
Classification and anatomical characteristics of the PPTA
Of all 24 patients with PPTAs, 11 (45.8%) were classified as type 1, three (12.5%) as type 2, five (20.8%) as type 3, one (4.2%) as type 4, and four (16.7%) as type 5b (Figs. 2-6). Fifteen PPTAs (62.5%) were located on the left side, and nine PPTAs (37.5%) on the right side. Of all 24 patients with PPTAs, 14 PPTAs (58.3%) originated from the posterior wall of the cavernous segment of the ICA, nine (37.5%) from the lateral wall, and one from the medial wall (4.2%). The PPTA diameter was larger than that of the BA in 10 cases (41.7%) and was smaller in the remaining 14 cases (58.3%). The portion of the basilar artery proximal to the insertion site of the PPTA showed severe to moderate hypoplasia in 13 cases (54%) and mild or no hypoplasia in 11 cases (46%).
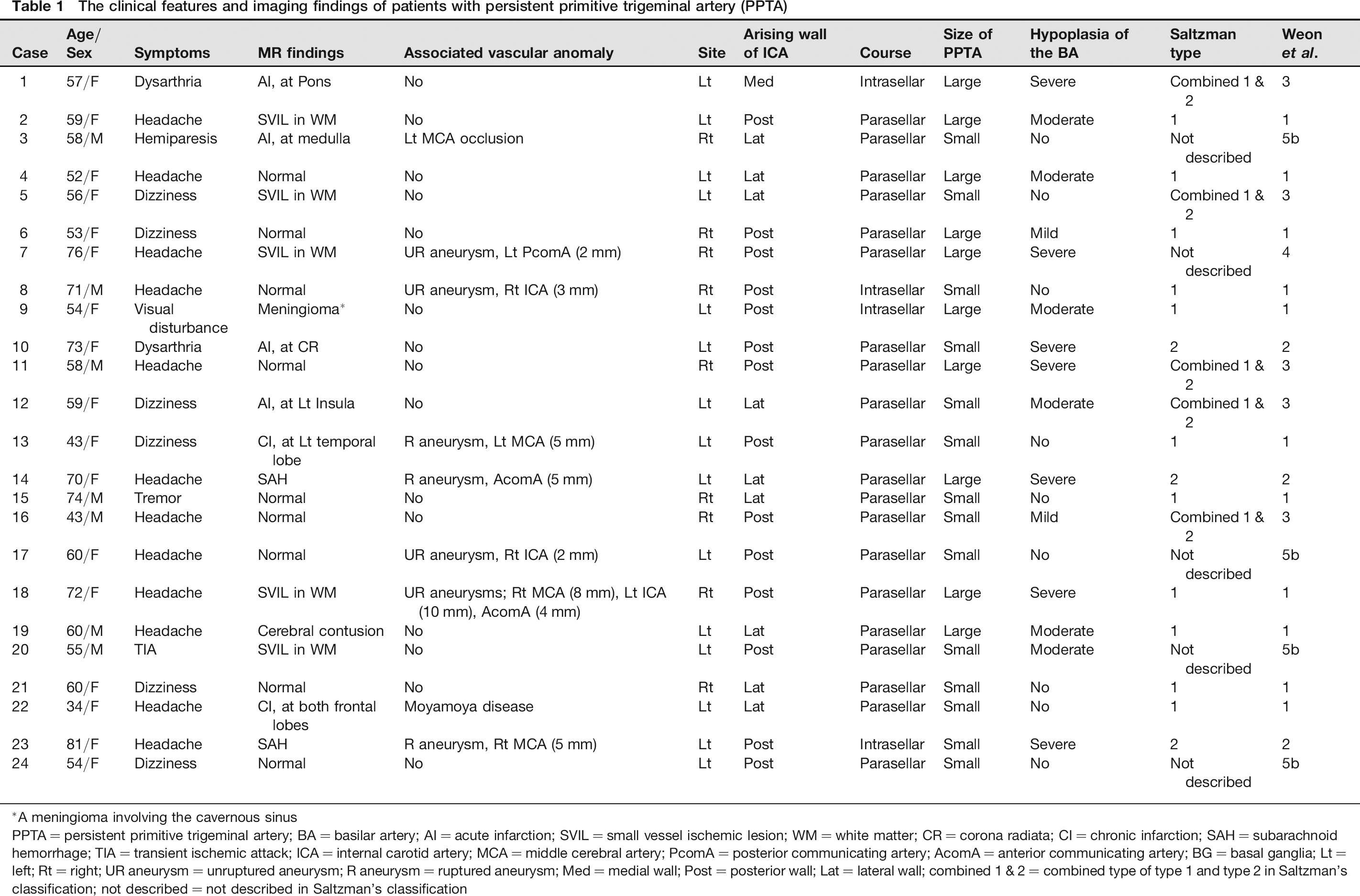
Type 1 (case 4), 3D-TOF-MRA (a, b) shows a large, persistent, primitive trigeminal artery (PPTA) arising from the cavernous portion of the left internal carotid artery (large arrow). The PPTA supplies the distal basilar artery (BA), posterior cerebral artery (PCA), and the superior cerebellar artery (SCA). This type of PPTA has the adult type of both PCAs (small arrows). The proximal portion of the BA reveals mild hypoplasia (arrow heads)
Type 2 (case 14), 3D-TOF-MRA (a, b) shows a small PPTA arising from the left internal carotid artery (large arrow). The PPTA is the main blood supply of the SCA territories (arrow heads), and the PCAs (small arrows) receive their blood supply primarily through the patent posterior communicating artery (PComA)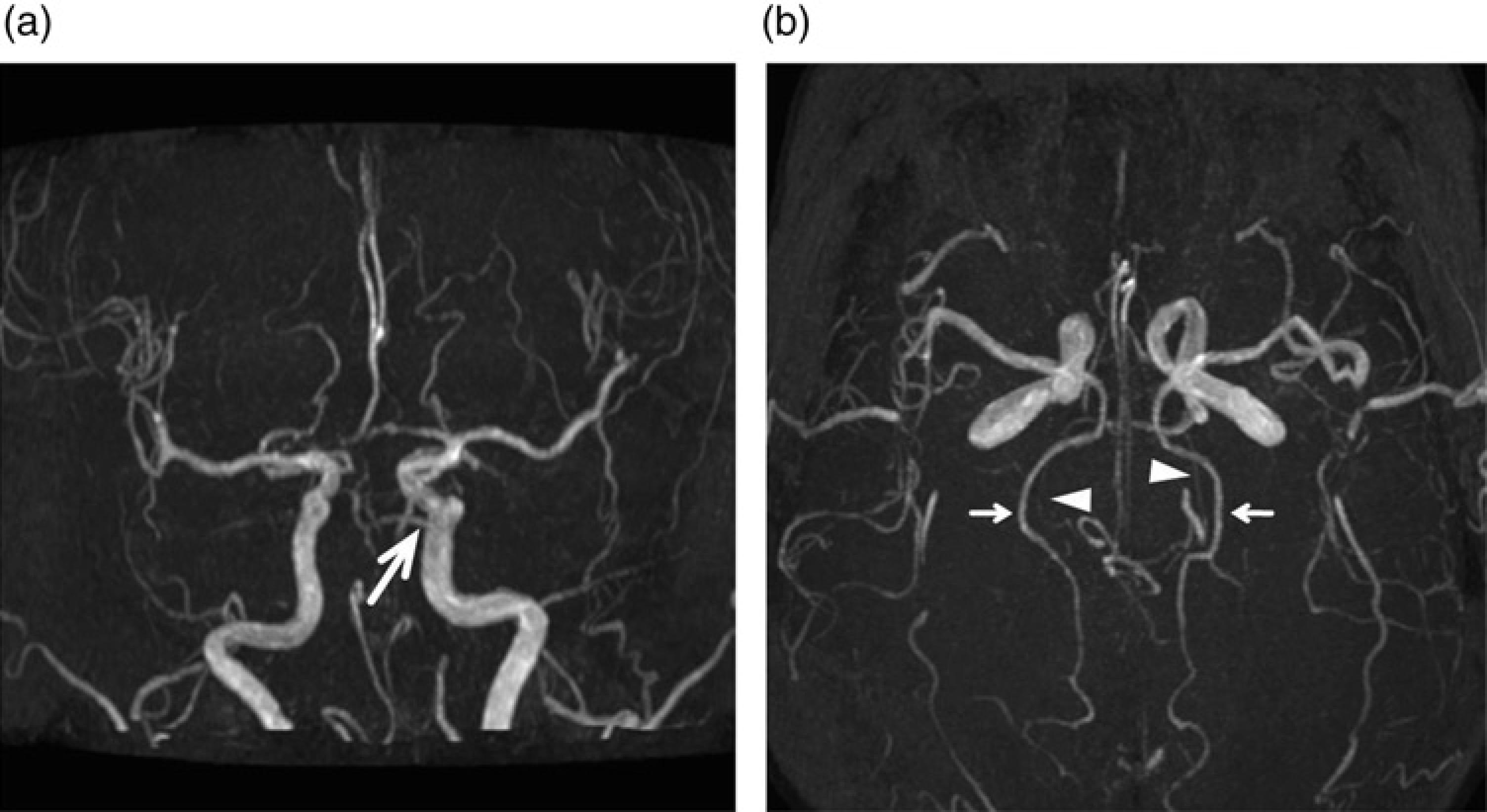
Type 3 (case 1), 3D-TOF-MRA (a, b) shows a small PPTA arising from the left internal carotid artery (large arrow). The contralateral PCA supplied by the PPTA (arrow heads) and the ipsilateral PCA receive their blood supply from anterior circulation via PComA (small arrow)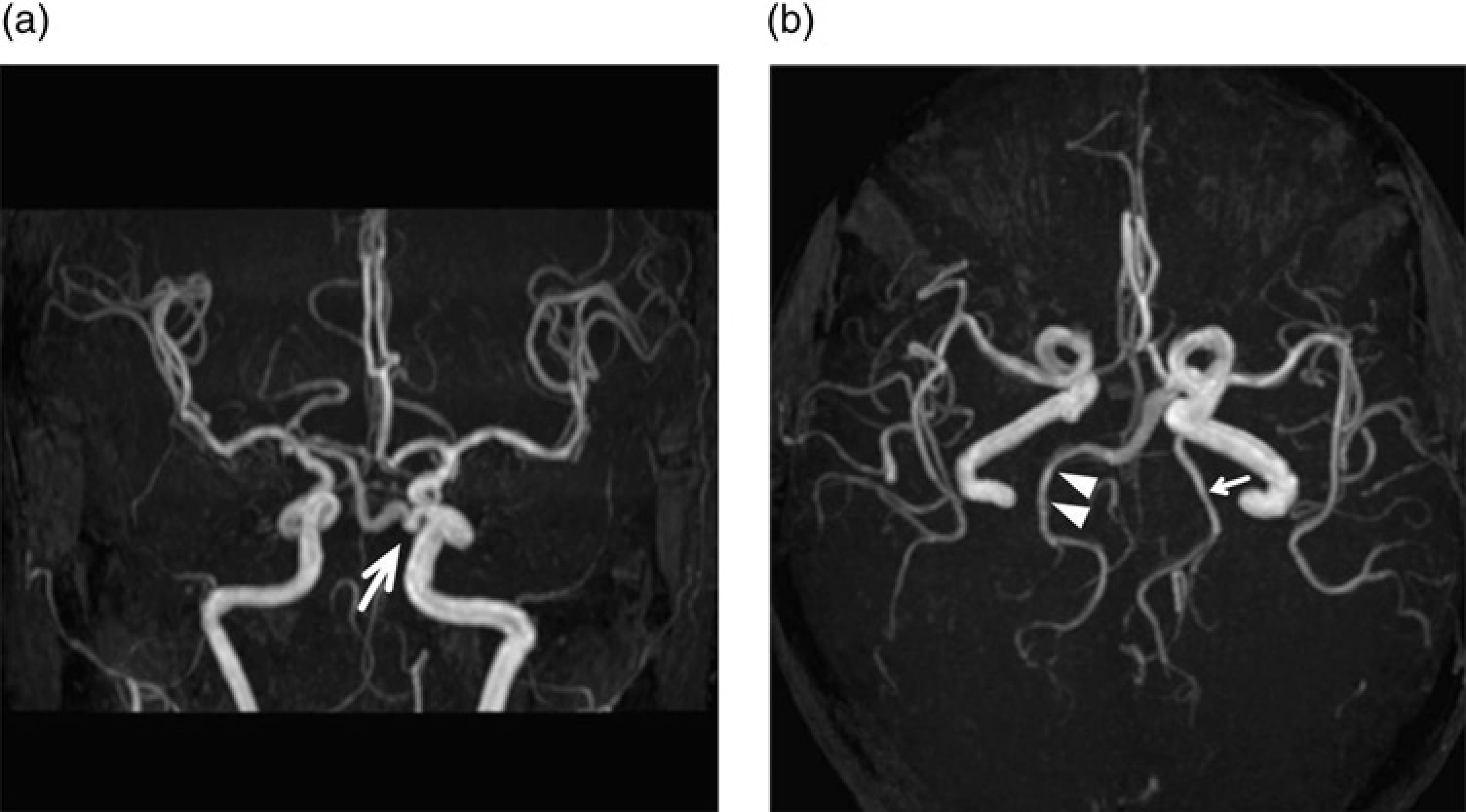
Type 4 (case 7), 3D-TOF-MRA (a, b) shows a large PPTA arising from the cavernous portion of the right internal carotid artery (large arrow). The ipsilateral PCA supplied by PPTA (large arrow) and the contralateral PCA receive their blood supply from anterior circulation via PComA (small arrow). The proximal portion of the BA reveals severe hypoplasia (arrow heads)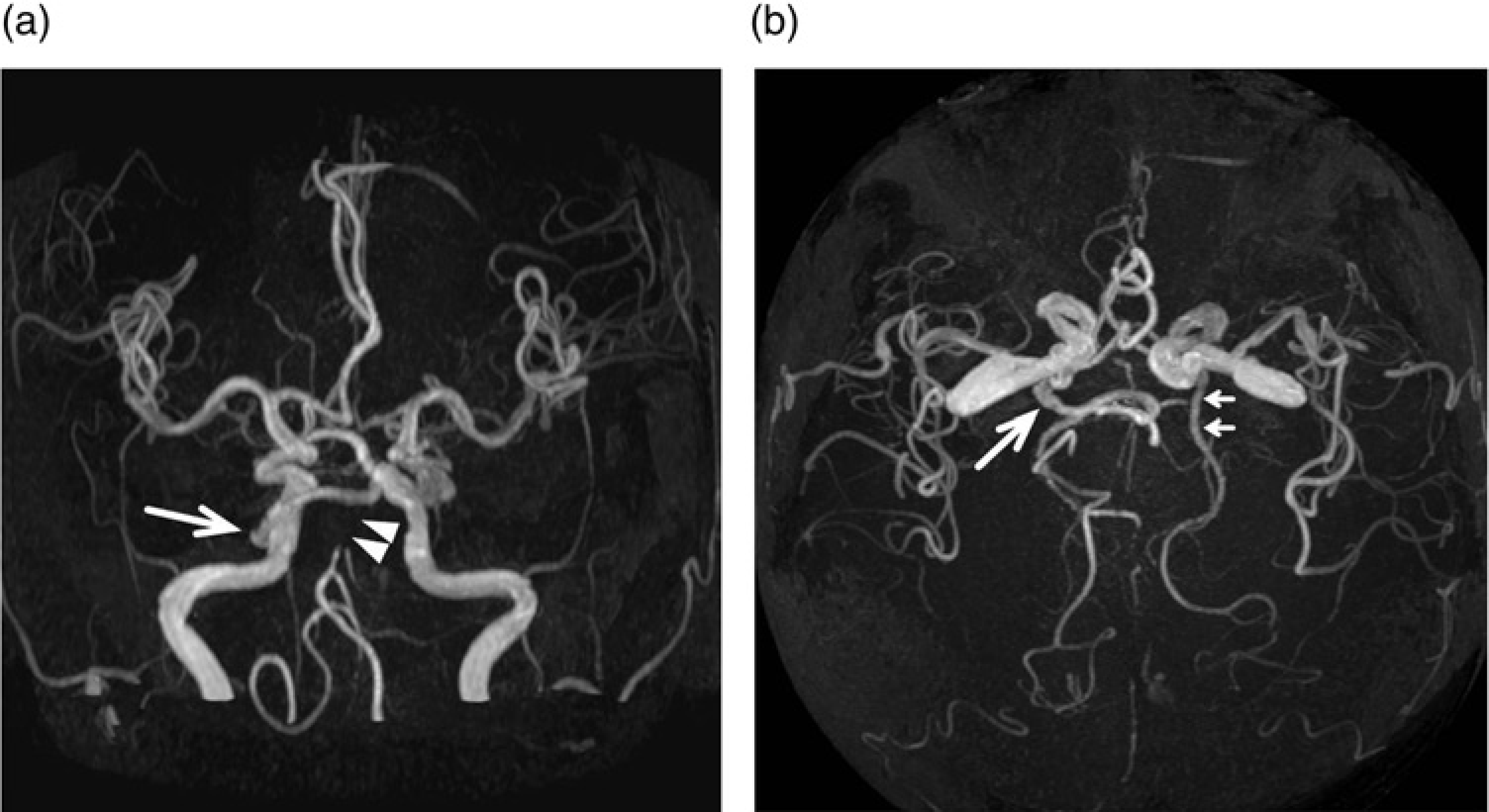
Type 5b (case 3), Oblique lateral MRA projection (a) shows a small PPTA arising from the right internal carotid artery (large arrow). The right internal carotid artery injection during digital subtraction angiograph (DSA) in the lateral projection (b), demonstrates that the right PPTA (large arrow) is feeding into the right hemispheric anteroinferior cerebellar artery territory (AICA), while the Townes projection of the left vertebral injection (c) demonstrates the lack of visualization of the right AICA territory, thus indicating the separate origin of this artery (small arrows)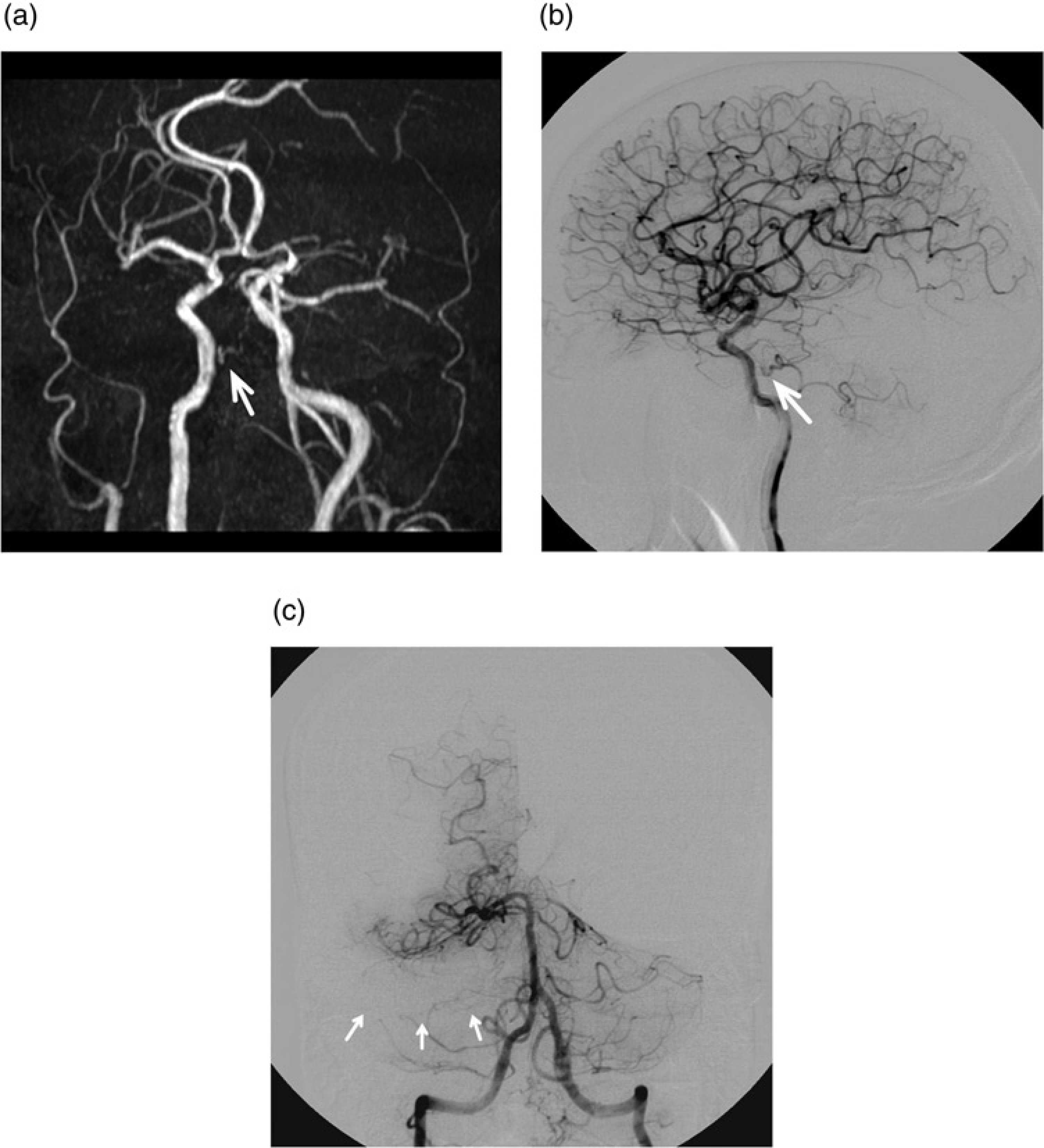
Associated vascular anomalies
Nine intracranial artery aneurysms were detected in seven (29%) of the 24 patients with PPTAs. In one patient, there were multiple aneurysms in three, different locations, i.e. the right MCA bifurcation site, AcomA, and the ICA bifurcation site. Three of the nine aneurysms were ruptured and the remaining six were incidentally noted during the MR studies. Moyamoya disease was found in one of the 24 patients with PPTAs. Other vascular abnormalities, such as AVM, arteriovenous fistula (AVF), or agenesis of the ICA, were not found in any of the study patients. Among the developmental variations, one patient had duplication of both distal VAs, one patient had duplication of the left VA with terminating posterior inferior cerebellar artery (PICA), one patient had BA fenestration, and one had two superior cerebellar arteries in both sides. One patient had occlusion of the proximal M1 of the left MCA.
Discussion
Embryogenesis of the PPTA
The persistence of primitive trigeminal artery (PPTA) is thought to result from regression failure during formation of the basilar artery (BA) and development of the posterior communicating artery (PComA). Four main fetal carotid-basilar anastomoses form on approximately the 24th day of fetal embryogenesis (in a 3- to 5-mm human embryo); these include the trigeminal, otic, hypoglossal, and the proatlantal intersegmental arteries, all of which progress caudally (7). These channels serve as the predominant blood supply to the developing hindbrain for approximately 7-10 days. With the formation of the PComA and fusion of the paired longitudinal neural arteries into the BA, the vessels begin to regress and disappear. The trigeminal artery is the largest of these arteries and persists for the longest embryonic period, usually being obliterated by the time of the 11.5- to 14-mm embryonic stage. Occasionally, these fetal carotid-basilar anastomoses persist after birth and even into adulthood, with the trigeminal artery being the most common and representing approximately 85% of these primitive persistent anastomoses (8).
The prevalence of PPTA
The prevalence of PPTA was estimated to be 0.33% using 3D-TOF MRA in this study and PPTA has been reported to be present in 0.06-0.6% of individuals (1-3). We retrospectively evaluated all of the 3D-TOF MRAs obtained in patients with a variety of clinical settings during a 33-month period in our hospital. In general, studies regarding the diagnosis of PPTA have been conducted using a small sample size or mainly analyzed based on direct cerebral angiography. As these angiography sessions often occur because of symptomatic vascular diseases, such as aneurysms, stroke, or vascular malformations, interpretation of the published literature may require careful attention in terms of prevalence of PPTA. This may also be responsible for the large variance in the reported prevalence of PPTA. In our study, the prevalence of PPTA was twice as high in women (0.42%) than in men (0.21%), with the reason why women have more PPTAs than men remaining unclear. PPTAs often exist unilaterally, and the frequency of the presence of left-sided PPTAs was slightly higher than those on the right side.
Classification of PPTA
In 1958, Georg-Fredrik Saltzman evaluated eight cases of PPTA along with preceding reports; he then classified the angiographic appearance of PPTA into two major variants and a mixed type of these two variants (4). Saltzman described one type (Type 1) as a variation, in which the PPTA enters into the BA between the superior cerebellar artery (SCA) and anterior inferior cerebellar artery (AICA) and the vertebrobasilar system distal to the anastomosis is supplied by the PPTA. In these cases, there was poor filling of the PcomA, with the patients thus having the adult type of bilateral PCAs. Our type 1 is the same as the Saltzman type 1; it was the most commonly encountered type in our study and was seen in 11 (45.8%) of our 24 patients. Saltzman also described the other type (Type 2) in which the PPTA enters into the BA, but mainly supplies the SCAs bilaterally. In these cases, the PCAs receive blood flow through the PcomA. This type is the equivalent of our type 2 which have fetal type, bilateral PCAs with well-developed PcomA. Three (12.5%) of our 24 patients showed this type. Saltzman described one case with a different type in his group, the so-called combination of types 1 and 2 (Type 3) in which the anastomosis supplied the SCA bilaterally as well as supplying the contralateral PCA. In this case, the ipsilateral PCA is supplied by the PcomA, and the contralateral primitive trigeminal artery as well as the contralateral PcomA regressed during the embryonic period. Five of our 24 patients (20.8%) had this type. However, in our series, one of the 24 patients (4.2%) showed a combination of PPTA and PcomA which differs from that originally described by Saltzman; the anastomosis supplied the SCA bilaterally as well as supplying the ipsilateral PCA. In this case, the contralateral PCA was supplied by the PcomA, and the contralateral primitive trigeminal artery and the ipsilateral PcomA were regressed during the embryonic period. Therefore, the PPTA could be reclassified into different types according to whether it supplies the contralateral PCA (Type 3) or the ipsilateral PCA (Type 4).
Some authors have also included variants of the PPTA for which there is no interposition of the BA in Type 3 (5, 6). In this variant, the PPTA arises from the C4 portion of the internal carotid artery and terminates directly as the SCA, AICA or PICA without joining the BA. Ali et al. (5) further subclassified this variant as Types a, b, and c, respectively. Regarding the Type 3, however, there might be some confusion between the combination of Types 1 and 2 which was originally described by Saltzman and the variants of PPTA without interposition of the BA because both of these types have been termed Type 3 by some authors. As these types differ in that one is connected to the BA while the other is not, considering these two variations as Type 3 is not suitable and may cause confusion. Therefore, we considered these variants as Type 5 and which can be sub-classified into Types 5a, b, and c according to the terminative patterns of the PPTA, the SCA, the AICA or the PICA, respectively. Four of our 24 patients showed Type 5b (16.7%). Rarely, PPTA has been found on both sides of the internal carotid arteries (9). The bilateral PPTA was not found in our study.
Hypoplasia of the proximal BA
Demonstration of a proximal hypoplastic BA below the abnormal communication, with enlargement above, has been considered an ancillary finding of PPTA (10). According to the hemodynamic of the posterior circulation distal to the connecting point between the PPTA and the BA, the BA can show a varying degree of hypoplasia of the proximal BA with or without hypoplasia of vertebral arteries (11). In our study, the patients with Types 1, 3, and 4 showed more severe hypoplasia of the proximal BA when they had a large PPTA than when they had a small PPTA. However, all of our patients with Type 2 showed severe hypoplasia of the proximal BA even if they had a small PPTA, and most of our patients with Type 5 showed well-developed BA without hypoplasia. As hypoplasia of the BA may indicate an important functional contribution of the anterior circulation to the posterior circulation, the fetal type of PCA in addition to PPTA might explain these findings. If there is fetal-type PCA, the flow stimuli might be relatively weak for the development of the VA and the BA. Therefore, further studies may be required.
Clinical significances of PPTA and associated vascular anomalies
The circulatory effects of a PPTA should be thoroughly investigated in order to evaluate the clinicopathological significance in case of vertebrobasilar insufficiency. As blood flow primarily from the carotid artery to the vertebrobasilar system, there is a risk of ischemic stroke of the brainstem, the cerebellar hemispheres, and the posterior lobes when there are emboli caused by ulcerated plaque in the common carotid bifurcation (12). In addition, poor antero-grade flow from a hypoplastic VA may also have a role in the presence of ischemia of the brain stem and cerebellar hemispheres (13). Two of our patients had acute stage cerebral infarction located in the posterior circulations, i.e. the pons and the medulla. Therefore, being aware of the existence of a PPTA as well as the various types could be essential for understanding the causes. Furthermore, prior recognition of a PPTA is important in surgical procedures involving the cavernous sinus or the posterior fossa, as this knowledge may prevent injury or disruption of the PPTA. Endovascular procedures for vascular malformations or aneurysms should also be appropriately modified in order to avoid ischemia of the posterior lobe, the brain stem, or the cerebellum. As a PPTA runs close to the Meckel's cave, a risk of hemorrhagic complications during a percutaneous gasserian ganglion procedure (gasserian ganglion alcohol block, radiofrequency gangliolysis, or ret-rogasserian glycerol injection) for treatment of trigeminal neuralgia, should be expected according to the various types of PPTA (14, 15).
PPTA is also associated with the increased prevalence of aneurysms. Saccular aneurysms can be found in as much as 14-32% of patients with PPTA or its variants (16, 17).
A study including 34 patients with PPTA demonstrated that the aneurysm prevalence by transfemoral cerebral angiography (TFCA) is approximately 3%, which is similar to that in the general population (18). In our study, seven of the 24 patients (29%) had aneurysms. This high prevalence is probably associated with the increasing detect-ability of aneurysms by MRA. Six of nine aneurysms were unruptured and four were less than 4 mm in size. Cerebral aneurysms associated with PPTA have been reported to occur in relation to the bifurcations formed by the PPTA and the carotid or basilar arteries in that the presence of structural defects in the wall has been suggested as the underlying cause (16, 19). We did not find an unusual distribution of aneurysms in our study patients with PPTA, and none of the nine aneurysms was detected anatomically associated with the PPTA. PPTA may also be associated with other vascular anomalies such as AVMs, AVFs, Moyamoya disease as well as with the absence of cervical arteries including the internal carotid artery and the common carotid artery (3, 5, 20-22). We did not find such vascular anomalies in the study patients except one that had Moyamoya disease.
The limitation of this study is that we did not compare all cases using DSA. Even though 3D-TOF MRA can show details of the distal branches of the cerebral arteries, it is still difficult to define anastomosis between small, distal branches. Moreover, we did not have any case of the two, other subtypes of Type 5. Thus, detailed subclassification of Type 5 might require DSA as well as further reinforcement with additional studies of whole subtypes of Type 5.
In conclusion, this study revealed five types of PPTA and necessitates an adjustment of the previous classification of PPTA on the basis of our results of MRA examinations. Although these anatomic variations are rarely observed, recognition is important for planning the surgical approach to treat the parasellar lesions and the posterior fossa, for performing percutaneous gasserian ganglion procedures, and for modifying endovascular procedures in order to avoid ischemia of the cerebellum, brain stem, and occipital lobes. A PPTA should be considered by both the clinician and the radiologist who interpret MR imaging studies, including MR angiography.
Footnotes
Acknowledgment
This work was funded by Ulsan University Hospital (Biomedical Research Center Promotion Fund). The authors would like to thank Bonnie Hami, MA (USA) for her assistance in preparing the manuscript.
None