
Abstract
Background
Standard bolus chase MR angiography (MRA) is increasingly replacing digital subtraction angiography (DSA) in the diagnostic evaluation of peripheral vascular disease. However, a major limitation of bolus chase MRA is the relatively poor visibility of the calf arteries.
Purpose
To evaluate the feasibility of visualizing the calf arteries and the visibility quality of an 8-channel cardiac phased array coil using time-resolved imaging of contrast kinetics (TRICKS) MRA compared with standard bolus chase MRA on a 1.5 Tesla MRI scanner.
Material and Methods
MRA findings of 59 sequential patients (mean age 57.8 years, range 14-83 years; 41 men) were retrospectively evaluated. All examinations included preliminary TRICKS for the lower leg using a surface 8-channel cardiac coil, followed by a 3-step MRA of the abdominal aorta, thigh, and lower leg using a body coil. Images yielded by both methods were separately evaluated by consensus of two radiologists unaware of the patients’ clinical data. Visibility of the calf arteries (popliteal, tibialis anterior, tibialis posterior, tibioperoneal trunk, and peroneal) for both sides was subjectively classified as ‘diagnostic’ or ‘non-diagnostic’. Descriptive statistics for image diagnostic quality were assessed.
Results
A total of 575 calf arterial segments were evaluated. Visibility of all calf arteries was significantly better with TRICKS than with the standard bolus chase MRA (P < 0.001). The improvement of calf artery visibility with TRICKS was more pronounced in patients with peripheral vascular disease compared to those with arteritis, vascular malformation and popliteal entrapment syndrome.
Conclusion
Using a cardiac coil for MRA of the lower extremities resulted in visibility comparable to that of a dedicated leg coil, with diagnostic superiority for the TRICKS method compared to the standard bolus chase method.
Standard bolus chase MR angiography (MRA) is increasingly replacing digital subtraction angiography (DSA) in the diagnostic evaluation of peripheral vascular disease (1, 2). Unlike DSA, it offers a non-invasive approach to diagnosis and treatment planning, eliminating the need for ionizing radiation and substantially decreasing the risk of nephrotoxicity, especially in elderly patients with peripheral vascular disease (PVD) due to atherosclerosis or various other causes and impaired renal function. One major limitation of bolus chase MRA, however, is the relatively poor visibility of the calf arteries, a drawback that mainly results from bolus timing problems that cause venous contamination of the images (3-5). Time-resolved imaging of contrast kinetics (TRICKS) MRA is a method of data acquisition designed to sample the center of the K-space more frequently than its peripheral zones, thus permitting a high temporal resolution and avoiding venous phase contamination (6, 7). The improved temporal resolution of TRICKS makes this technique a potentially well-suited method for the evaluation of the arteries below the knee. Indeed, some studies have shown favorable diagnostic performance of TRICKS in comparison to standard bolus chase MRA (8), with a degree of visibility compatible to that of DSA (9, 10). These studies, however, used a dedicated peripheral vasculature coil which is heavy and painful, especially for patients with PVD and associated ischemic leg and ulcerated wounds. An 8-channel phased array cardiac coil is smaller, lighter, and much easier and faster to use for patients such as these.
The purpose of the current study was to evaluate the feasibility and the quality of visualizing calf arteries by an 8-channel cardiac phased array coil using the time-resolved technique compared with standard bolus chase MRA on a 1.5 Tesla MRI scanner, and to assess these two features specifically in patients with PVD. To the best of our knowledge, this is the first attempt to test the combination of TRICKS and an 8-channel cardiac coil.
Material and Methods
MRA findings of 59 sequential patients (41 men and 18 women; mean age 57.8 years, range 14-83 years) were retrospectively evaluated. All examinations were conducted in our institution on a 1.5 Tesla scanner (Signa, HDx; GE Healthcare, Milwaukee, WI, USA). The local ethics committee approved this retrospective study.
Scanning protocol
The protocol for all examinations, which is routinely used in our institution for lower extremities MRA, included a preliminary time-resolved scan (Time-Resolved Imaging of Contrast Kinetics, TRICKS) for the lower leg using a surface 8-channel cardiac coil (GE Healthcare, Milwaukee, WI, USA), followed by a three-step MRA of the abdominal aorta, thigh, and lower leg using a standard body coil. TRICKS and 3-step MRA were always performed in the same session and in the same order, first the TRICKS for the calf arteries and then the 3-step MRA.
Tricks
The following protocol was used: TR/TE/Flip/BW; 4.2/ 1.1/ <30°/41.67, field of view; 380 mm × 380 mm matrix; 320 × 224,10-12 frames per series with temporal resolution of 7-8 s. Spatial resolution of 1.2 × 1.2 × 1.0 was achieved after 512 × 512 zero-filling reconstruction. A total of 15 mL of Gadoterate meglumine (Gd) (Dotarem; Guerbet, Roissy, France) was administered by power injection at a rate of 0.5 mL/s followed by a normal saline flush of 20 mL at 1 mL/s, with a trigger delay of 20 s.
Standard three-station bolus chase MRA
First, three-plane non-enhanced localizer images of the abdomen and pelvis (first station), thighs (second station), and calves (third station) were performed, followed by a contiguous MRA using a ‘bolus-pro’ technique, software which allows an interactive start of scanning in real time. The contrast-enhanced MRA imaging was synchronized with a biphasic administration of 20 mL Gd (rate 1.2 mL/ s) combined with 20 mL saline flash (rate of 1.2 mL/s), followed by 12 mL Gd (rate of 0.6 mL/s) combined with 10 mL saline flash (rate of 1.2 mL/s) using an automated injector (MEDRAD Inc., Indianola, PA, USA). The parameters of the mask image and the contrast-enhanced images were identical for all three stations.
Image analysis
All scans were postprocessed on a commercial AW 4.2 station (GE Healthcare). Mask images were subtracted from the corresponding contrast-enhanced images and maximum-intensity projection (MIP) reformations were generated. The raw data images and the resulting MIP reformations were evaluated by consensus of two radiologists with dedicated experience of 16 years in conventional angiography (UR) and seven years in MRA (EK), both unaware of the patients’ clinical data.
Visibility of the following arteries for both sides was subjectively classified as ‘diagnostic’ or ‘non-diagnostic’: popliteal, tibialis anterior, tibialis posterior, tibioperoneal trunk, and peroneal. A segment was considered diagnostic if all clinically relevant diagnostic information could be obtained with good differentiation of arterial vasculature from background tissue. Segments were considered ‘non-diagnostic’ when visibility did not allow reliable diagnosis due to blurring of an arterial segment, inadequate vessel enhancement, motion or metal artifacts, or venous contamination.
Statistical analysis
The data were summarized using prevalence of significantly stenotic artery and percent of ‘diagnostic’ visibility of various arteries using both tests. Visibility of calf arteries’ segments on TRICKS was compared to the standard bolus chase MRA using the McNemar test, appropriate to matched paired design. We also compared results of standard bolus chase MRA in the group of PVD patients with the results of the same method in the group of patients with other indications, such as arteritis, vascular malformation, and popliteal entrapment syndrome.
For this comparison several variables were defined:
(1) TRICKS provided diagnostic visibility while standard bolus chase MRA did not. (0) Both methods provided the same results (e.g. both provided diagnostic visibility or neither provided). (-1) TRICKS did not provide diagnostic visibility but standard bolus chase MRA did.
The distribution of these variables was compared in the two groups.
Additionally, the d percent of improvement was compared in both groups by segments and in total. Fisher Exact test was used for these comparisons. Also, the relative rate of improvement was calculated and compared with the assumption of no improvement in each group and between groups.
Results
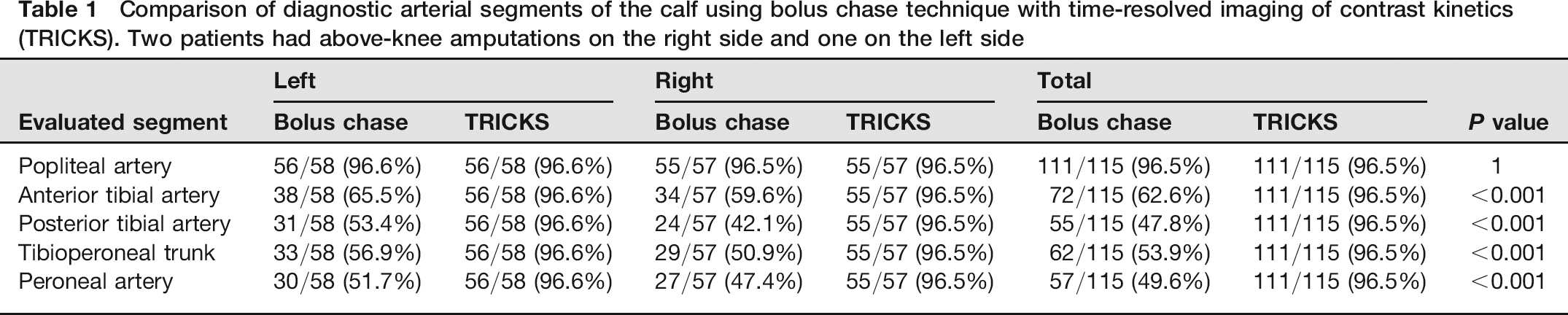
The indications for MRA were suspected PVD (45 patients), suspected arteritis (7 patients), evaluation of vascular malformation (6 patients), and popliteal entrapment syndrome (one patient). Three patients had undergone above-knee amputations, resulting in a total number of 575 calf arterial segments which were evaluated twice, once by standard bolus chase MRA and once by TRICKS (Table 1). An MRA examination with the 8-channel cardiac coil was technically feasible in all studies. The prevalence of significant stenosis (defined as >50%) or occlusion of each arterial segment in patients with suspected PVD and non-PVD patients is shown in Table 2. Visibility of all calf arteries was significantly better with TRICKS compared with the standard bolus chase MRA (Fig. 1). Out of 575 tests, 10 tests were ‘non-diagnostic’ in both methods, 10 were ‘diagnostic’ with standard method but ‘non-diagnostic’ with TRICKS, 208 were ‘diagnostic’ with TRICKS but ‘non-diagnostic’ with standard MRA, and 347 were ‘diagnostic’ with both methods (P < 0.001 with McNemar test). The visibility of the posterior tibial and peroneal arteries with the standard bolus chase MRA reached only 47.8% and 49.6%, respectively, each improving to 96.5% with TRICKS (Table 1). In fact, failure to visualize arteries with TRICKS happened only in two patients (due to movement), in both cases all calf arteries could not be visualized. The improvement of calf artery visibility with TRICKS was more pronounced in patients with PVD compared with the patients who had other indications. Those differences were most significant for the peroneal, tibioperoneal and posterior tibial arteries (Tables 3 and 4).
MRA of a 60-year-old woman with suspected peripheral vascular disease. (a) Maximum-intensity projection (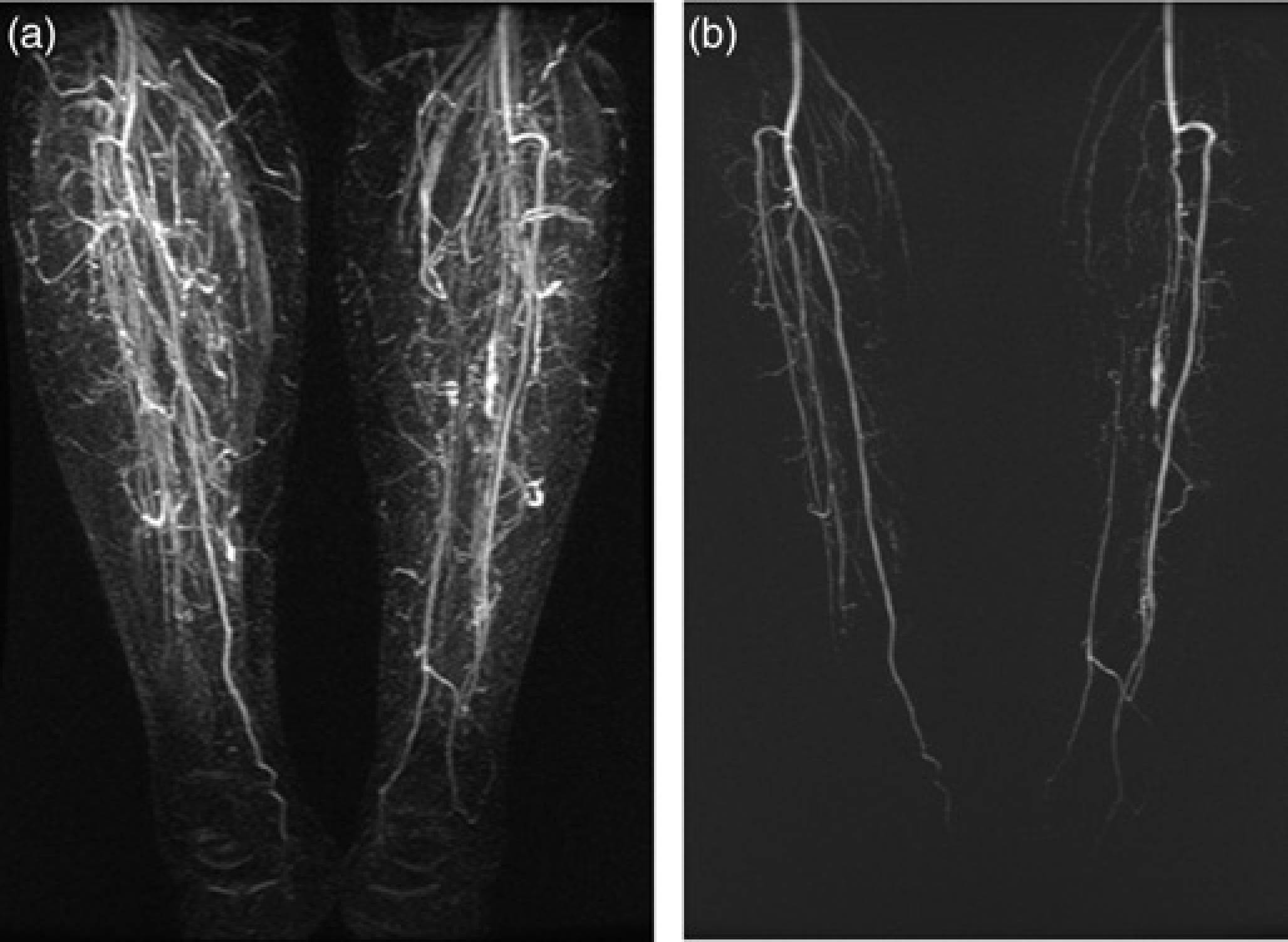
Comparison of diagnostic arterial segments of the calf using bolus chase technique with time-resolved imaging of contrast kinetics (TRICKS). Two patients had above-knee amputations on the right side and one on the left side
Prevalence of significantly stenotic arteries * in patients with suspected peripheral vascular disease (PVD) and patients with other indications
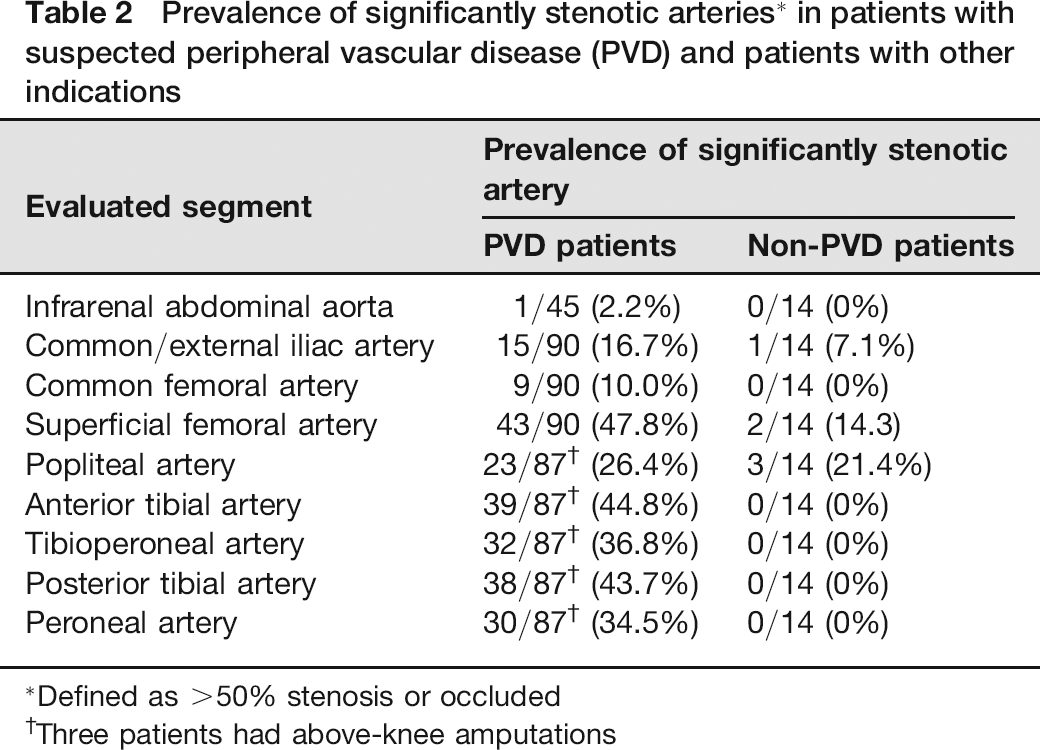
Defined as >50% stenosis or occluded
Three patients had above-knee amputations
Visibility of calf arterial segments using bolus chase technique and time-resolved imaging of contrast kinetics (TRICKS) in patients with peripheral vascular disease (PVD) vs. patients with other indications *
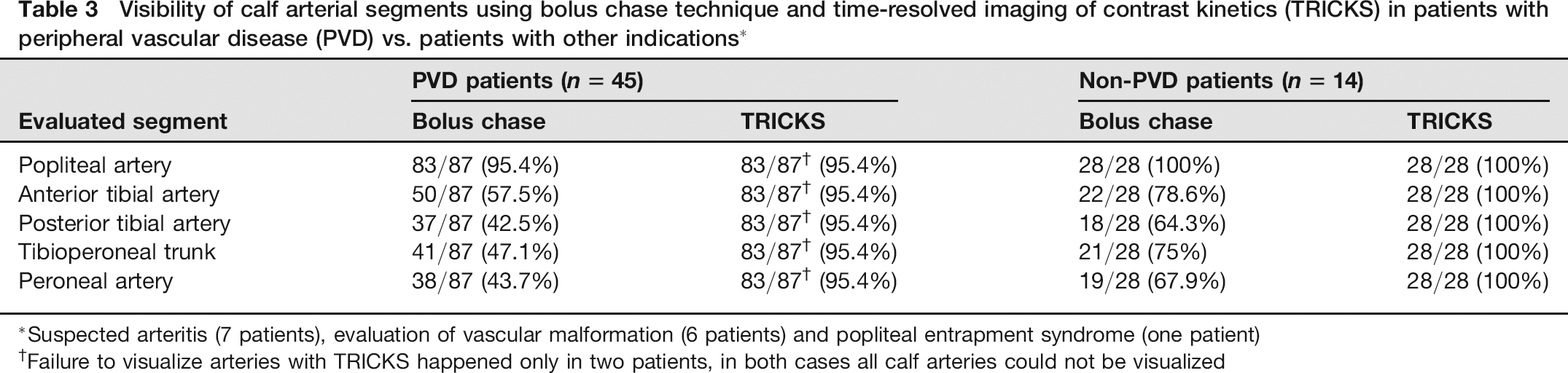
Suspected arteritis (7 patients), evaluation of vascular malformation (6 patients) and popliteal entrapment syndrome (one patient)
Failure to visualize arteries with TRICKS happened only in two patients, in both cases all calf arteries could not be visualized
Number of tests when TRICKS was worse (-1), same (0) or better (+1) than bolus chase MRA by segments and group of diseases (numbers in second line in each cell are percents of the total number of tests of the segment in the group)

P value for testing the hypothesis that there is the same number of test when TRICKS was worse (21) and better (+1) than standard bolus chase MRA
RR – ratio of proportion of improvement in the PVD group to proportion of improvement in the non-PVD group
P value testing the hypothesis that the distribution of worse/same/better results was the same in both groups
P value for the test that the proportion of improvement (+) was the same in both groups
A. – Artery, Ant. – Anterior, Post. – Posterior
Discussion
Optimal radiological demonstration of the popliteal and calf arteries is crucial for treatment planning in patients with severe PVD (11). Catheter angiography can be avoided or performed for target-specific treatment with lower amounts of contrast if the vascular anatomy is known in advance. Due to the high prevalence of impaired renal function in patients with PVD, examinations that use iodine contrast media, such as invasive angiography and CT angiography, should be avoided whenever possible. MRA is an attractive non-invasive alternative modality for those patients. A previous study in which a dedicated peripheral coil had been used showed improved visibility of calf arteries when TRICKS MRA was used compared with standard MRA (8).
However, patients with PVD may suffer from edematous lower legs, ulcerated skin lesions and rest pain. Our clinical experience was that the adjustment of their calf into a dedicated peripheral coil as described above was generally inconvenient and sometimes very painful, posing a challenge for the team as well as being time-consuming. Visibility of the calf arteries in the current study on standard and TRICKS MRA was evaluated by means of a light and easy to use 8-channel cardiac phased array coil.
The visibility of calf arteries using this unique combination of coil and TRICKS MRA was excellent, reaching 97% of the 575 evaluated segments. These results are in concordance but not identical with those of a previous series that evaluated the visibility of arteries with TRICKS using a dedicated peripheral coil (8). Andreisek et al. compared the visibility of lower limb arteries in 31 patients on TRICKS MRA and standard bolus chase MRA with the gold standard of DSA using a dedicated peripheral coil: one reader interpreted the results as showing an improvement from 82% to 88% and the second reader from 79% to 85% (8).
Archambault et al. also compared the two MRA methods by using a similar type of scanner but with a body coil (10). In their study, from 63% to 66% of arterial segments were considered diagnostic with TRICKS compared to 41% to 47% with the standard bolus chase. Although these values reflect the same tendency of improved diagnostic readability for TRICKS, the visibility of both methods was lower compared to results of the present study.
The visibility rates with standard MRA obtained in the present work were lower than those of Andreisek et al. (between 47.8% and 62.6%, depending on the segment) (8) and higher with TRICKS MRA (96.5%) than their and Archambault's (10) studies. Such differences can be explained by different injection protocols, the different coils that were used, improvement of the TRICKS technique (a newer version of the scanner was used in the current study), different mixture of severity of disease and indications, and due to subjective differences between readers. Nevertheless, the significant improvement in image visibility when using TRICKS that was shown in the present study, even with a non-dedicated coil (such as an 8-channel cardiac coil), further emphasizes the advantage of using TRICKS for the calf arteries in combination with the standard three-step MRA. Our results also show that the use of TRICKS in patients with PVD is more advantageous than when used for other indications such as vasculitis or vascular malformation. This is not surprising since patients with PVD tend to have a higher prevalence of significant stenotic lesions which might not be symmetrical and thus require different optimal acquisition time delay between the two calves. In such cases, TRICKS allows several repeated acquisitions and arterial imaging of each leg in different timing.
The disadvantage of an additional scan is longer scanning time and a second IV gadolinium injection. Although there has been increasing concern about the development of nephrogenic systemic fibrosis in patients with renal failure, and although renal impairment is not uncommon in patients with PVD who require peripheral MRA, the results in the current study suggest that the clinical benefit of this additional sequence overrides a potential risk. This reasoning is further supported by the evidence of an even higher improvement of arterial visibility of calf arteries when using TRICKS in patients who have PVD compared with patients with other indications. To reduce the risk of nephrogenic systemic fibrosis in patients with chronic renal failure who require peripheral MRA, we prefer to use in all our patients Gadoterate meglumine (Dotarem), which is cyclical in structure and least likely to release free gadolinium ions into the body (12).
A major limitation of the present study is that the TRICKS MRA results were not compared with angiographic findings, and so the strength of the conclusions relies on previous studies which showed the diagnostic capabilities of standard bolus chase MRA. In addition, due to its retrospective nature, it was not possible to compare the quality of images obtained with a dedicated peripheral coil with those of a cardiac coil in the same patients. Instead, the visibility results were compared with those obtained in previous studies using a peripheral dedicated coil.
In conclusion, using a cardiac coil for MRA of the lower extremities results in comparable visibility to those obtained by means of a dedicated leg coil and with diagnostic superiority for the TRICKS method compared to the standard bolus chase.
Footnotes
None