
Abstract
Background
Left ventricular (LV) function is a vital parameter for prognosis, therapy guidance, and follow-up of cardiovascular disease. Dual-source computed tomography (DSCT) provides an accurate analysis of global LV function.
Purpose
To assess the performance of DSCT in the determination of global LV functional parameters in comparison with cardiovascular magnetic resonance (CMR) and two-dimensional transthoracic echocardiography (2D-TTE) in patients with valvular heart disease (VHD).
Material and Methods
A total of 111 patients (58 men, mean age 49.9 years) with known VHD and who underwent DSCT, 2D-TTE, and CMR a period of 2 weeks before undergoing valve surgery were included in this study. LV end-systolic volume (ESV), end-diastolic volume (EDV), stroke volume (SV), and ejection fraction (EF) were calculated by DSCT using the threshold-based technique, by 2D-TTE using a modified Simpson's method, and by CMR using Simpson's method. Agreement for parameters of LV global function was determined with the Pearson's correlation coefficient (r) and Bland-Altman analysis. All the DSCT and CMR data-sets were assessed independently by two readers.
Results
Fifty of the total 111 patients had aortic VHD, 29 patients had mitral VHD, and 32 patients had mixed aortic and mitral VHD. An excellent inter-observer agreement was seen for the assessment of global LV function using DSCT (r = 0.910–0.983) and CMR (r = 0.854–0.965). An excellent or good correlation (r = 0.93, 0.95, 0.87, and 0.71, respectively, P < 0.001) was noted between the DSCT and 2D-TTE values for EDV, ESV, SV, and EF. EDV (33.7 mL, P < 0.001), ESV (12.1 mL, P < 0.001), SV (21.2 mL, P < 0.001), and EF (1.6%, P = 0.019) were significantly overestimated by DSCT when compared with 2D-TTE. An excellent correlation (r = 0.96, 0.97, 0.91, and 0.94, respectively, P < 0.001) between DSCT and CMR was seen in the evaluation of EDV, ESV, SV, and EF. EDV (15.9 mL, P < 0.001), ESV (7.3 mL, P < 0.001), and SV (8.5 mL, P < 0.001) were significantly underestimated, but EF (1.1%, P = 0.002) was significantly overestimated by DSCT when compared with CMR.
Conclusion
Our study showed that DSCT measurements of global LV function using the threshold-based technique were highly reproducible and compared more favorably with CMR measurements using Simpson's method than those of 2D-TTE using the modified Simpson's method. DSCT enables accurate quantification of global LV function in patients with VHD.
Keywords
The precise and reproducible evaluation of global left ventricular (LV) function is fundamental for the clinical diagnosis, risk assessment, therapeutic strategy, prognosis, and follow-up of cardiovascular disease (1). Of the various non-invasive imaging modalities, echocardiography has been considered to be the first non-invasive tool to assess LV function. However, echocardiography is operator-dependent, has relatively low reproducibility, and might be impaired by a poor acoustic window (2–6). With the rapid technical advancements in the last decade, cardiovascular magnetic resonance (CMR) has been very useful in clinical practice and is now considered to be the reference standard for assessment of LV function with high accuracy and reproducibility because of excellent temporal resolution, superior tissue contrast, and a 3-dimensional (D) approach for asymmetric LV. However, the safety of CMR remains controversial for patients with implanted electronic devices such as pacemaker or defibrillator (7–9). The improved temporal resolution of dual-source computed tomography (DSCT) reduces cardiac motion artifacts particularly during systole, and therefore enables an accurate assessment of LV volumes and allows a clear depiction of cardiac anatomy including the coronary artery and cardiac valves (10–14). Recently, some studies have demonstrated that evaluation of LV function by DSCT revealed a good correlation with that by CMR (15–17). Image quality of multidetector CT (MDCT) decreased with increasing heart rate (HR) (15). Kim et al. have reported that DSCT is the method available for global LV function evaluation in patients with severe arrhythmia, with results comparable to those of transthoracic echocardiography (TTE) (18). However, so far, no study has been conducted on correlation of global LV function by DSCT using the threshold-based technique, by CMR using Simpson's method, and by 2D-TTE by using a modified Simpson's method in a large population. The purpose of this study was to assess the performance of DSCT in the determination of global LV functional parameters in comparison with CMR and 2D-TTE in patients with valvular heart disease (VHD).
Material and Methods
Patient population
Between May 2009 and June 2010, we enrolled 176 consecutive patients (90 men, 86 women; mean age 51.4 ± 14.3 years; range 20–78 years) with VHD and who underwent DSCT, 2D-TTE, and CMR before undergoing valve surgery. DSCT was performed for the preoperative evaluation of coronary artery anatomy including coronary artery origin and stenosis, valve morphology, the presence and extent of valve calcification, and ascending aorta diameter. CMR was performed for the preoperative assessment of VHD severity, valve morphology, global LV function, the presence and extent of LV myocardial fibrosis, and ascending aorta diameter.
Of the 176 patients enrolled, 65 patients were excluded from the study. Thirty-one patients underwent 2D-TTE, DSCT, and CMR in a duration of over 2 weeks; 19 patients had insufficient image quality (CMR only [n = 15), DSCT and CMR [n = 4]) due to severe atrial fibrillation (AF) (mean HR > 61 beats per minute [bpm]); eight patients had a poor acoustic window on TTE, and seven patients had insufficient CT image quality due to severe respiratory motion artifacts (n = 4) and poor contrast opacification of the LV cavity related to AF and severe mixed VHD (n = 3). Finally, 111 patients with known VHD (58 men, 53 women; mean age, 49.9 ± 14.2 years) were included in the study. Among 111 patients, 87 patients had sinus rhythm, 12 sinus bradycardia, eight premature atrial or ventricular contraction, and four sinus tachycardia. The exclusion criteria for DSCT were as follows: unstable clinical status, acute coronary syndrome, asthma, deterioration of renal function (serum creatinine > 1.5 mg/dl), known allergy to iodinated contrast agents, and New York Heart Association class IV congestive heart failure. The institutional ethics committee approved this retrospective study protocol and stated that the informed consent was not required.
DSCT scanning protocol, reconstruction and analysis
Before the DSCT, HR of each patient was measured. If a patient had a pre-scan HR of more than 65 bpm and did not have severe aortic stenosis, the patient was administered 50–100 mg of metoprolol orally 1 h before the scan for reducing the chances of cardiac motion artifacts. All patients received sublingual administration of 0.6 mg nitroglycerin 1 min before the examination for the dilatation of coronary arteries.
All CT examinations were performed on a DSCT scanner (Somatom Definition, Siemens Medical Solutions, Forchheim, Germany). DSCT was performed using the following imaging parameters: detector collimation 2 × 32 × 0.6 mm; slice acquisition 2 × 64 × 0.6 mm using the z-flying focal spot technique; gantry rotation time 330 ms; pitch 0.20–0.43 (adapted to the HR); tube voltage 100 kVp or 120 kVp (depending on age and body mass index); and tube current-time product 80 mAs per rotation for calcium scoring and 330 mAs per rotation for CT. With the scout image, the anatomical range extended from 2 cm above the carina to the diaphragm in a craniocaudal direction. A non-enhanced CT scan for calcium burden of the AV and coronary artery was performed with electrocardiography (ECG)-based tube current modulation before DSCT. The full tube current was applied at 70% of the R-R interval, and the tube current outside the 70% R-R interval was reduced to 4% of the nominal output (MinDose, Siemens Medical Solutions). For DSCT, ECG-based tube current modulation was not implemented. Data acquisition was performed during an inspiratory breath-hold, while the ECG was recorded simultaneously for retrospective gating of the data.
Contrast agent application was controlled by a bolus tracking technique. A region of interest was positioned into the aortic root, and image acquisition was started 7 s after the signal density level reached the predefined threshold of 120 Hounsfield units (HU). For all CT examinations, a dual-head power injector (Stellant D; Medrad, Indianola, PA, USA) was used to administer a three-phase bolus at the rate of 4.5 mL/s: first, 70–80 mL of iopromide (Ultravist 370®; Bayer Healthcare, Berlin, Germany) was administered. Afterwards, 45 mL of a 70%–30% blend of contrast medium and saline was administered and finally, 45 mL of saline was administered.
A monosegment reconstruction algorithm that uses data from a quarter rotation of both the detectors was used for image reconstruction. Reconstruction parameters were as follows: image matrix was set at 512 × 512 pixels; field of view was adjusted according to the individual's structure in order to capture the heart exactly, and a medium-smooth convolution kernel (B 26f). For a functional analysis using the raw data, 10 transaxial data-sets were reconstructed at every 10% (0–90%) of the cardiac cycle using a retrospective monosegment ECG gating algorithm; the specifications used were an effective slice thickness of 1.0 mm and reconstruction increment of 1.0 mm. Axial data-sets were then transferred to an external workstation (Cardiac Functional Analysis, Vitrea® 2, Version 4; Vital Images Inc., Plymouth, MN, USA) using a commercially available software. After loading a multiphase CT data-set, the software automatically generated horizontal and vertical long-axis reformations, as well as short-axis images of the heart.
The contrast-enhanced LV lumen was automatically segmented for all cardiac phases according to differences in attenuation values (HU). To determine the LV volume, we selected the end-diastolic phase, which was the phase with the largest LV cavity, and the end-systolic phase, the phase with the smallest LV cavity among 10 cardiac phases (0–90%), and then delineated the endocardial and epicardial LV contours with manual editing on the short-axis cine images. Papillary muscles were excluded during computation of the LV volume by attenuation-based segmentation. LV end-diastolic volume (EDV), end-systolic volume (ESV), stroke volume (SV), and ejection fraction (EF) were calculated directly using the software (Fig. 1a). Analysis and measurement of LV function using the DSCT data-sets was performed by two experienced radiologists who were blinded to all patient clinical information and the results of CMR and 2D-TTE examinations.
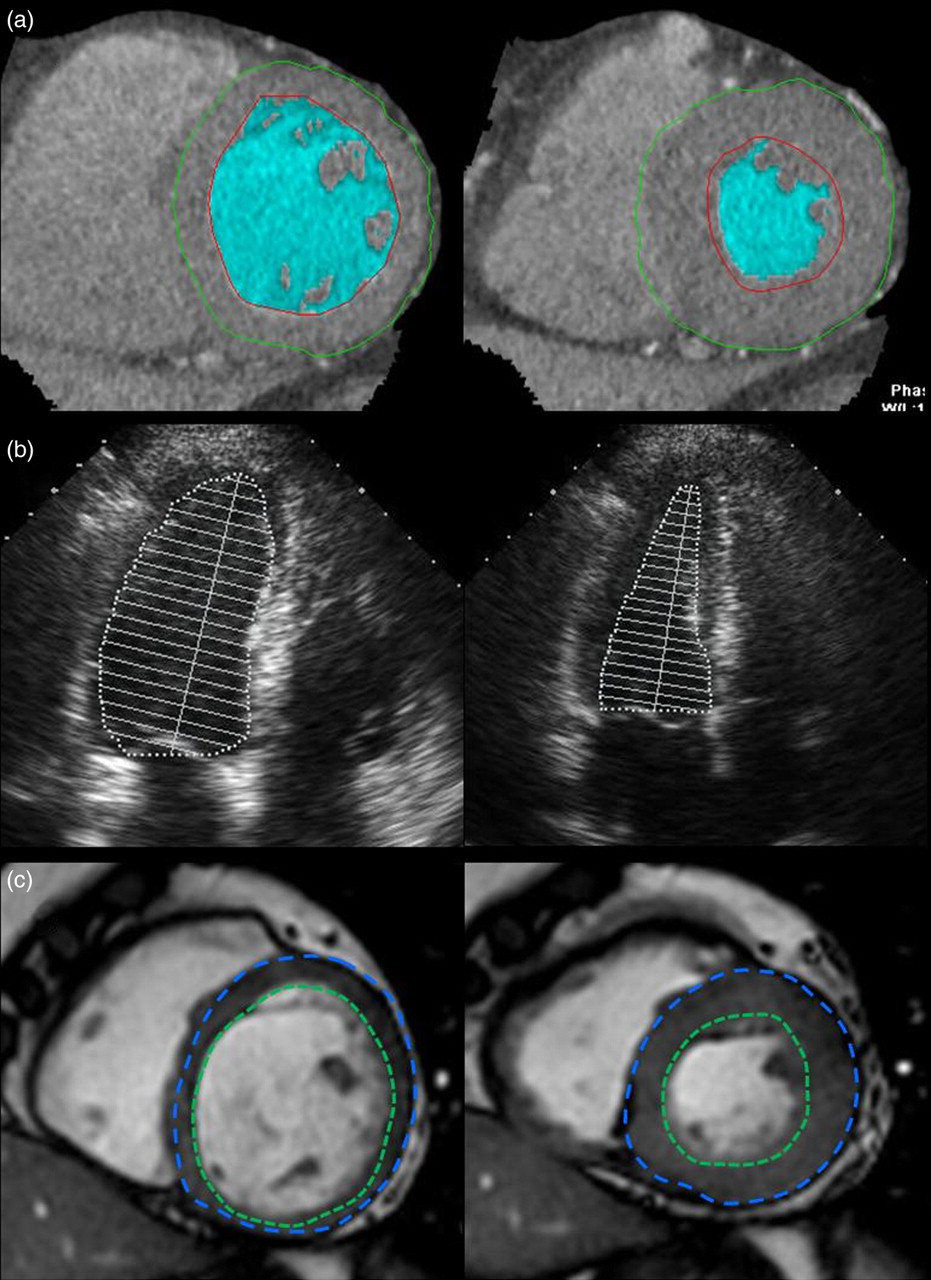
Cardiac images show an example of global left ventricular functional data obtained from the same patient during end-diastole and end-systole by dual-source computed tomography using the threshold-based technique (a), by 2-dimentional transthoracic echocardiography using a modified Simpson's method (b), and by cardiovascular magnetic resonance using Simpson's method (c)
Echocardiography
Echocardiographic examinations were performed using an Acuson Sequoia (Siemens Medical Systems USA, Mountain View, CA, USA) or a GE Vivid 3 (GE Healthcare, Milwaukee, WI, USA) echocardiography system, and two experienced echocardiographers performed the echocardiography. All data were recorded on an S-VHS videotape. As 2D measurement for EF calculation, a modified Simpson's method was used, and images were obtained in the standard apical and parasternal 2- and 4-chamber views (Fig. 1b) (19, 20). Images were optimized so that clear definition of the LV endocardial border was apparent. Chamber and wall dimensions were measured by consensus of two observers using standard recommendations for chamber quantification (19). For measurement of LV volume in end-systole and end-diastole, three beats were required to average the measurement of LV volume. Analysis and measurement of LV function were reviewed by two cardiologists in consensus.
Cardiovascular magnetic resonance (CMR)
All 112 patients underwent CMR which was performed with a 1.5-T whole-body system (Signa HD, GE Healthcare, Milwaukee, WI, USA) using an eight-element phased array surface coil (Cardiac coil, GE Healthcare). All examinations were carried out by experienced technicians and supervised by an experienced radiologist. Cine images were acquired with gradient echo FIESTA sequence (echo time 1.54 ms; repetition time 3.54 ms; flip angle 45°; slice thickness 8 mm without interslice gaps; field of view 36 × 36 cm; matrix 224 × 224; pixel size 0.16 × 0.16 cm). LV functional parameters were calculated using Simpson's method (Fig. 1c). Analysis and measurement of LV function using the CMR data-sets were performed by two observers (1 radiologist and 1 radiographer) who were blinded to the results of 2D-TTE and DSCT examinations.
Radiation dose
An effective radiation dose for the DSCT examination was calculated for all patients. The dose-length product (DLP, measured in milligray-centimeters) is defined as the volume CT dose index multiplied by scan length and is an indicator of the integrated radiation dose of the entire CT examination. DLP is displayed on the dose report on the CT scanner and recorded. A reasonable approximation of the effective radiation dose of CT was calculated by multiplying DLP by a conversion coefficient for the chest (κ = 0.017 mSv·mGy−1·cm−1) (21).
Statistical analysis
In descriptive statistical analysis, continuous variables were expressed as means ± standard deviations. Categorical variables were expressed as frequencies or percentages. Comparison of global LV functional parameters obtained by DSCT, 2D-TTE, and CMR was performed by using the paired Student's t test, Pearson's correlation coefficient, and Bland-Altman analysis. The inter-observer agreement with regards to EDV, ESV, SV, and EF as obtained by DSCT and CMR was assessed with an intraclass correlation coefficient. Pearson's correlation coefficient values were as follows: 0 = poor; 0.01–0.20 = slight; 0.21–0.40 = fair; 0.41–0.60 = moderate; 0.61–0.80 = good; and 0.81–1.00 = excellent. For all data analysis, P < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS, version 11.5 software (SPSS, Chicago, IL, USA).
Results
Of 111 patients, 50 patients had aortic VHD, 29 patients had mitral VHD, and 32 patients had mixed aortic and mitral VHD. All patients underwent DSCT and CMR without any complications. Threshold-based 3D segmentation of the LV was feasible in all DSCT data-sets. The average HR during DSCT was 65.2 ± 10.8 bpm. Thirty-two patients (29%) were administered metoprolol. Patients who used metoprolol showed an average HR of 73.6 ± 8.1 bpm and the average HR after administration of metoprolol decreased by about 8 bpm (65.7 ± 8.7 bpm). The calculated effective radiation dose in each patient was 9.2 ± 2.7 mSv. Clinical characteristics of each patient are summarized in Table 1.
Patient characteristics
All data are expressed as mean ± SDs
DSCT = dual-source computed tomography, VHD = valvular heart disease
For inter-observer agreement analysis of each LV functional parameters from the DSCT and CMR data-sets, intraclass correlation coefficients for EDV, ESV, SV, and EF were 0.975, 0.983, 0.956, and 0.910 with DSCT, and 0.965, 0.884, 0.951, and 0.854 with CMR, respectively. Pearson's regression analysis showed an excellent correlation between DSCT and 2D-TTE for EDV, ESV, and SV. A good correlation was observed between the two modalities for EF (r = 0.71, P < 0.001; Table 2). Comparing DSCT with 2D-TTE, the Bland-Altman analysis revealed the over-estimation of EDV, ESV, and SV that proved to be significantly different (P < 0.001, respectively; Fig. 2). An excellent correlation was noted between the DSCT and CMR for EDV, ESV, SV, and EF (Table 2). Comparing DSCT with CMR, Bland-Altman analysis showed the under-estimation of EDV, ESV, and SV that proved to be significantly different (P < 0.001, respectively; Fig. 3). The difference in the mean EF by DSCT was statistically significant but minimal when compared to that by 2D-TTE (1.6 ± 7.0%, P = 0.019) and CMR (1.1 ± 3.5%, P = 0.002).
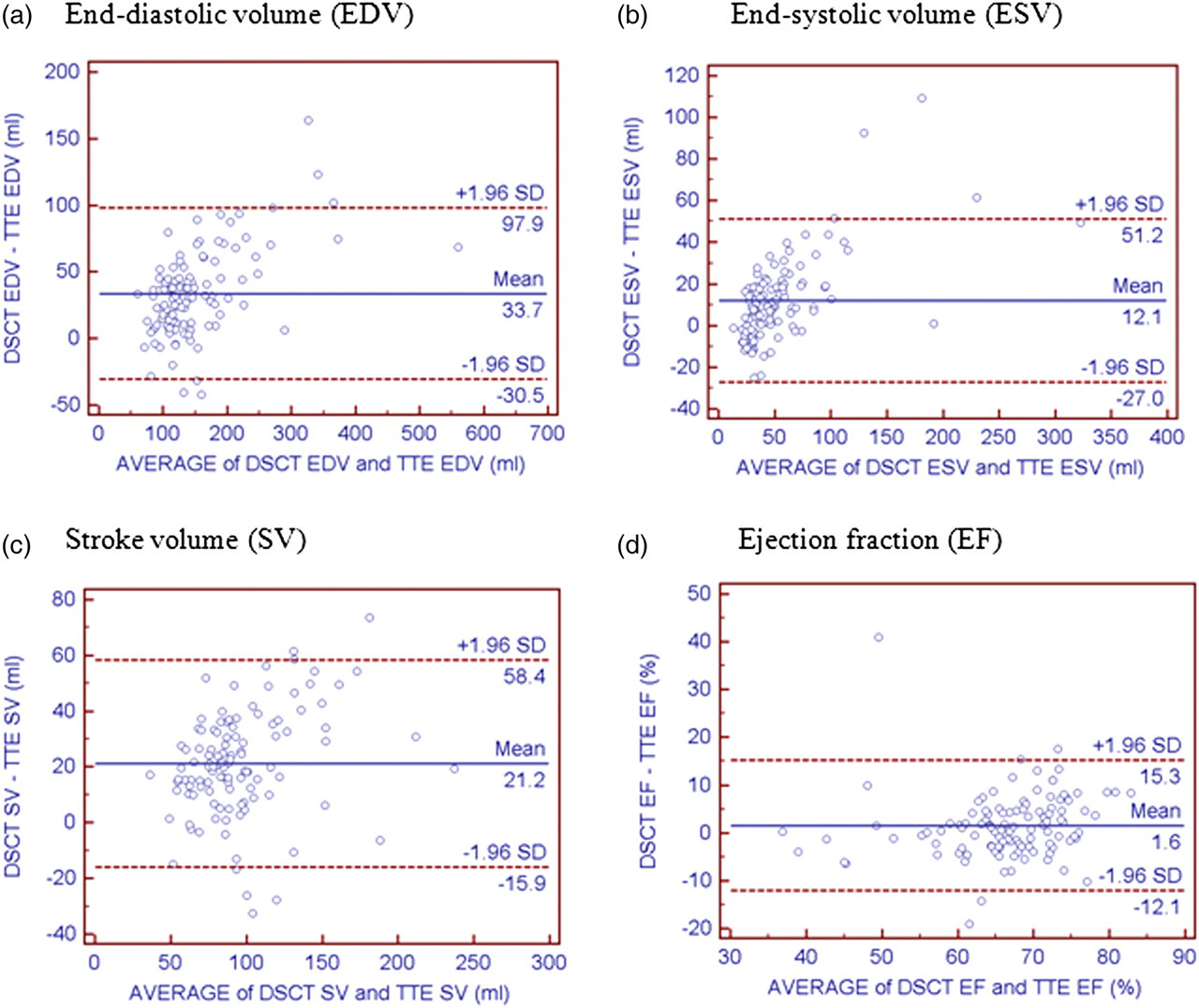
Bland-Altman plots show left ventricular end-diastolic volume (a), end-systolic volume (b), stroke volume (c), and ejection fraction (d) acquired from dual-source computed tomography in comparison with 2-dimentional transthoracic echocardiography, depicting agreement between the difference of the two measurements (y axis) and the average of the two measurements (x axis)
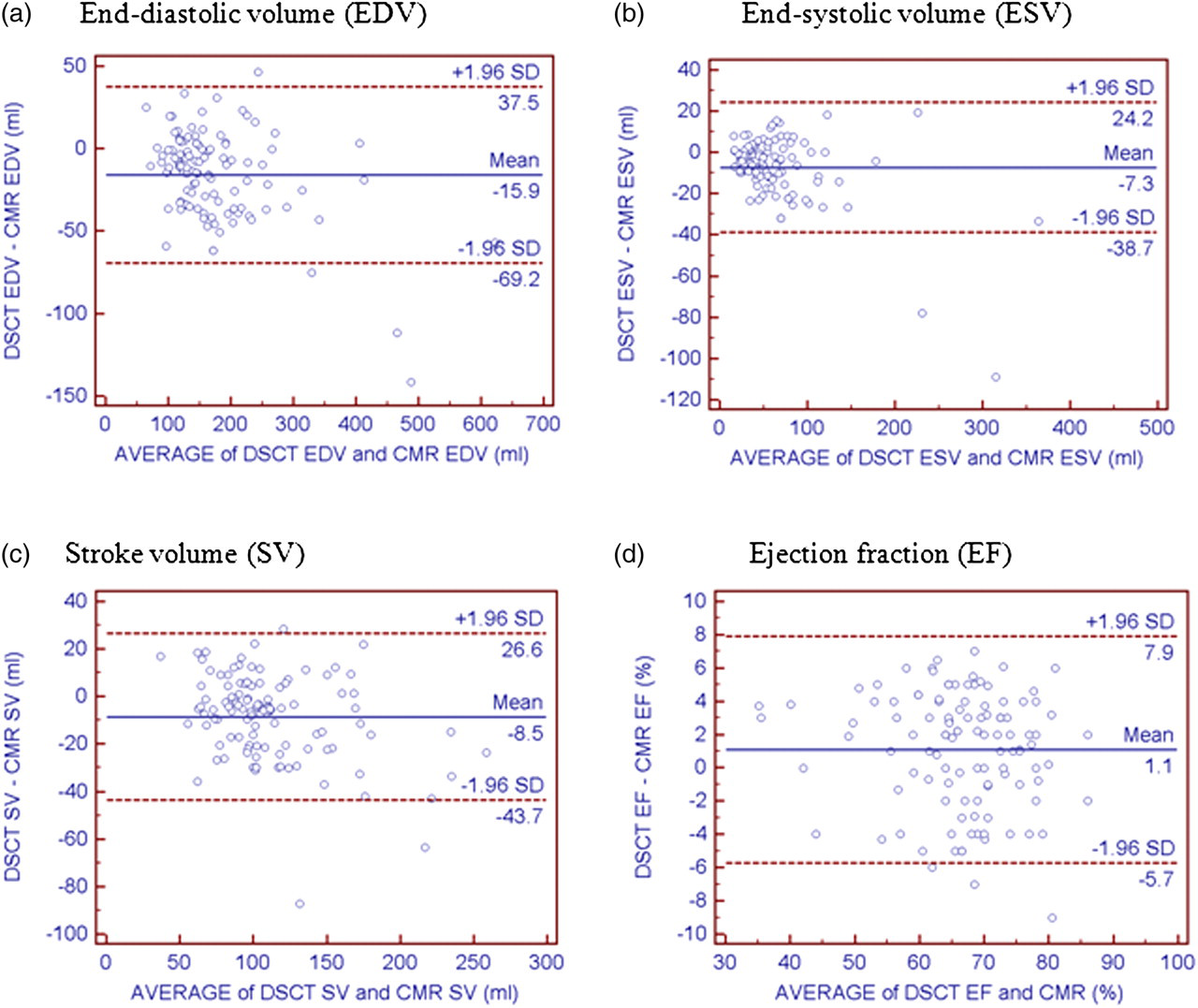
Bland-Altman plots show left ventricular end-diastolic volume (a), end-systolic volume (b), stroke volume (c), and ejection fraction (d) acquired from dual-source computed tomography in comparison with cardiovascular magnetic resonance, depicting agreement between the difference of the two measurements (y axis) and the average of the two measurements (x axis)
Global left ventricular functional parameters: comparison of DSCT with TTE and CMR
All data are expressed as mean ± SDs
SD = standard deviation, CMR = cardiovascular magnetic resonance, DSCT = dual-source computed tomography, TTE = transthoracic echocardiography, EDV = end-diastolic volume, ESV = end-systolic volume, SV = stroke volume, EF = ejection fraction
Discussion
In the present study, DSCT using a threshold-based technique provided highly reproducible measurements of global LV functional parameters, which were significantly smaller than the CMR values using Simpson's method except for the EF. DSCT measurements of global LV functional parameters compared more favorably with CMR measurements using Simpson's method than those of echocardiography using a modified Simpson's method.
LV function is an important indicator for clinical decision-making and prognostic value in patients with VHD. For example, in patients with mitral regurgitation (MR), a decreased EF should be an indication for MR surgical correction. However, if LVEF is 50–59%, the structure and functional remodeling of the ventricle can be reversible after surgery (22, 23).
In our study, an excellent correlation was observed between DSCT and CMR for LV volumes and LVEF, though EDV and ESV were significantly underestimated by DSCT when compared with CMR. On the contrary, EDV and ESV were significantly overestimated by DSCT when compared with 2D-TTE but there was an excellent correlation between DSCT and 2D-TTE. DSCT measurement of LVEF was more highly correlated with CMR (r = 0.94) than 2D-TTE (r = 0.71). The LVEF was significantly different but minimal in difference among the three modalities. Automated threshold-based 3D-segmentation enables a precise and reliable measurement of global LV functional parameters from the DSCT data-sets with an excellent correlation to CMR with Simpson's method (17).
Several possible causes may account for the differences in LV volume measurement by the use of multi-imaging modalities. The difference of LV volume can be explained by a different handling of the papillary muscles. In 2D-TTE, the delineation of the endocardial border of the LV was performed by manual tracing. Therefore, inclusion or exclusion of papillary muscle was dependent upon operator interpretation (24). Soft-tissue density structures such as papillary muscles were excluded from the LV volume by attenuation-based segmentation in CT and included into the LV cavity in CMR. Papillary muscles account for 8.9% of the LV volume as determined by CMR (25). Accuracy of 2D-TTE is limited by a foreshortened apical view or difficulty of LV geometric assumptions (26). Different DSCT and CMR measurements are possible due to injection of a large volume of iodine contrast agent, which can cause a transient change of preload and a negative inotropic effect. In addition, acute changes in blood pressure in response to the rapid injection of contrast agent need to be considered (3). The relatively low temporal resolution of DSCT compared with CMR contributed to the estimation of LV function. In general, beta-blockers have been widely used to acquire sufficient image quality for estimation of coronary arteries because beta-blockers can reduce artifacts from the motion of the coronary artery by reducing HR (27–30). Jensen et al. have reported that intravenous beta-blocker administration prior to CT examination resulted in a statistically significant reduction in the HR, LVEF, and cardiac output and an increase in the ESV due to the negative inotropic effect (31). In the present study, 32 patients (29%) were administered metoprolol. Thus, the inotropic effect of metoprolol could result in change in LV functional parameters.
Some limitations existed in our study. First, LV functional parameters could be affected by artificially reduced HR by premedication with beta-blockers. Second, this study design had selection bias. We excluded 26 patients with non-diagnostic image. Most of them were due to severe AF which was associated with VHD, particularly mitral valve disease. Our 1.5-T MR scanner did not have a function called ‘Arrhythmia Rejection’, and we could not assess LV volume in 19 patients with severe arrhythmia. Despite severe arrhythmia, we tried to assess LV volume using DSCT with ECG editing (18) but failed to measure LV volume (n = 4), In addition, threshold-based 3D segmentation could not be applied because of banding artifact related to severe respiratory motion artifacts and poor contrast opacification of the LV cavity. Third, general disadvantages of CT are the use of potentially nephrotoxic contrast and high radiation exposure. ECG-dependent tube current modulation is the effective modality for reducing patient dose by up to 50% (32–34). However, ECG-dependent dose modulation was not used in this study. Fourth, most of the patients did not undergo DSCT, CMR, and 2D-TTE examinations on the same day. During this period, there was a possibility of change in the LV function in patients due to their respective medications.
In conclusion, our study showed that DSCT measurements of global LV function using a threshold-based technique were highly reproducible and compared more favorably with the CMR measurements using Simpson's method than those of 2D-TTE using the modified Simpson's method. DSCT enables accurate quantification of LV volume and LVEF and can serve as an alternative to CMR and 2D-TTE for the assessment of global LV function in patients with VHD.
Footnotes
Acknowledgments
This work was supported by the Konkuk University Medical Center Research Grant 2010.