
Abstract
Background
Diffusion tensor imaging (DTI) is a form of functional magnetic resonance imaging (MRI) that allows examination of the microstructural integrity of white matter in the brain. Dementia is a neurodegenerative disease, and DTI can provide indirect insights of the microstructural characteristics of brains in individuals with different forms of dementia.
Purpose
To evaluate the value of DTI in the diagnosis and differential diagnosis of patients with subcortical ischemic vascular dementia (SIVD) and Alzheimer's disease (AD).
Material and Methods
The study included 40 patients (20 AD patients and 20 SIVD patients) and 20 normal controls (NC). After routine MRI and DTI, fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values were measured and compared in regions of interest (ROI).
Results
Compared to NC and AD patients, SIVD patients had lower FA values and higher ADC values in the inferior-fronto-occipital fascicles (IFOF), genu of the corpus callosum (GCC), splenium of the corpus callosum (SCC), and superior longitudinal fasciculus (SLF). Compared to controls and SIVD patients, AD patients had lower FA values in the anterior frontal lobe, temporal lobe, hippocampus, IFOF, GCC, and CF; and higher ADC values in the temporal lobe and hippocampus.
Conclusion
DTI can be used to estimate the white matter impairment in dementia patients. There were significant regional reductions of FA values and heightened ADC values in multiple regions in SIVD patients compared to AD patients. When compared with conventional MRI, DTI may provide a more objective method for the differential diagnosis of SIVD and AD disease patients who have only mild white matter alterations on T2-weighted imaging.
Keywords
In principle, the definitive diagnosis of dementia depends on an autopsy (1). The clinical diagnosis of dementia is based on symptoms, neuropsychological tests, and neuroimaging studies. Among these strategies, neuroimaging studies play an important role in the early diagnosis and differential diagnosis of the various types of dementia.
Considerable overlaps exist between Alzheimer's disease (AD) and vascular dementia in areas such as clinical features, pathological lesions, and the associated risk factors (2). Vascular dementia, the second most common cause of dementia, encompasses a heterogeneous group of cognitive impairments caused by various cerebrovascular lesions. SIVD is a subtype of vascular dementia where abnormalities are found by magnetic resonance imaging (MRI) in subcortical white matter regions (3). The proportion of SIVD among vascular dementias ranges from 36% to 67%. (4). The cognitive symptoms in patients with SIVD are characterized by dysexecutive syndrome with slowing of mental processing and relatively mild memory deficits (5, 6).
Patients with vascular dementia typically show high signal intensities in the periventricular or subcortical regions on T2-weighted imaging (T2WI). Furthermore, periventricular high signal intensity on T2WI is frequently observed in normal elderly subjects and AD, which makes it difficult to differentiate AD from vascular dementia by conventional MR imaging.
The aim of this study was to identify the distribution of microstructural alterations in the white matter in patients with different types of dementia with the use of diffusion tensor imaging (DTI), and to evaluate the value of DTI in the differential diagnosis of SIVD and AD patients who have only mild white matter alterations on T2WI.
DTI is a type of functional MR imaging that enables the examination of the microstructural integrity of white matter in vivo (7–10). This emerging technique combines MR diffusion weighted pulse sequences with tensor mathematics to measure molecular diffusion in three dimensions. Two complementary parameters obtained from DTI measurements are the apparent diffusion coefficient (ADC) and fractional anisotropy (FA), which are known to be influenced by changes in the tissue microenvironment, and the provision of quantitative measures of directionally averaged diffusion. DTI is even able to outline the white matter architecture and reveal structures that are usually hidden on conventional MRI scans. DTI studies have shown that microscopic white matter changes exist in patients with AD and mild cognitive impairment (MCI), which are not detected by conventional MRI (11–13).
Although DTI has been mainly used to investigate regional white matter changes, it is still not clear whether it can also be adopted to study microstructural alterations of subcortical white matter of SIVD. The aim of this study was to identify the distribution of microstructural changes in white matter in patients with different dementias using DTI, and whether DTI may be a more objective method for differentiating between SIVD and AD.
Material and Methods
From June 2008 to June 2010, 40 patients who were diagnosed with AD (n = 20) or SIVD (n = 20) were prospectively enrolled in this study. AD and vascular dementia were diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer Disease and Related Disorders Association (NINCDS-ADRDA) criteria (14) and the National Institute for Neurological Disorders and Stroke-Association Internationale pour la Recherche et l'Enseignement en Neuroscience (NINDS-AIREN) criteria (15), respectively. SIVD was diagnosed based on the criteria proposed by Erkinjuntti et al. (16). The inclusion criteria for SIVD were: (a) global cognition assessed with the 30-point Mini Mental State Examination (MMSE) ≤23 and a Montreal Cognitive Assessment (MoCA) score ≤14; (b) a Clinical Dementia Rating (CDR) (17) score >1; and (c) a Hachinski Ischemic Score (HIS) >4. The inclusion criteria for mild AD were: (a) diagnostic evidence of probable AD consistent with the NINCDS-ADRDA criteria (14); (b) MMSE score ≤23; MoCA score ≤14; (c) CDR score >1; and (d) HIS <4. The inclusion criteria for NC were: (a) ability to function independently; (b) a normal detailed neurological examination; (c) MMSE score ≥28; (d) MoCA score ≥25; and (e) CDR score = 0.
Aside from the exclusion criteria mentioned by Di Paola (7), some other criteria are as follows: (a) patients who could not comply with the recognition tests; and (b) patients with metal implants that contraindicated the use of MR imaging. To make the groups comparable for DTI, those patients with AD who had no white matter alterations and those patients with vascular dementia who had severe white matter alterations on T2WI were excluded. These criteria were based on a modification of those for subcortical vascular dementia described by Erkinjuntti et al. (15). Finally, 20 healthy normal control (NC) elderly individuals were recruited from the same geographical area, and were rigorously matched with the patient groups for age and gender.
The participants' demographic and clinical information is listed in Table 1. There were no significant differences between the three groups with respect to variables such as age, gender, and level of education. However, the groups differed significantly on their MMSE and MoCA scores. Pairwise comparisons indicated that SIVD and AD patients had significantly lower MMSE scores and MoCA scores than NC participants.
Summary of demographic characteristics
Each value shows the mean ± SD
ANOVA was used to compare the difference among three groups
Between patients and age-matched controls, *P < 0.05
NC = normal controls, AD = Alzheimer's disease, SIVD = subcortical ischemic vascular dementia, MMSE = mini-mental status examination, MoCA = Montreal Cognitive Assessment
All participants underwent the same imaging protocol, which included whole-brain T1-weighted, diffusion-weighted scanning, and standard clinical sequences (T2, fluid attenuated inversion recovery [FLAIR]) using a 3.0 Tesla Allegra MR imager (3.0T Achieva, Philips Medical System, Best, The Netherlands) with an 8-channel phased array head coil. The following MR images were obtained: flip angle 90°, thickness 6 mm. Other parameters were: (a) axial T1W turbo spin-echo (TSE) (repetition time (TR)/echo time (TE) 2000/20 ms, field of view (FOV) 220 × 220 mm, matrix 512 × 512); (b) axial T2W TSE (TR/TE 3000/80 ms, FOV 256 × 256 mm, matrix 512 × 512); (c) sagittal T1W SE (TR/TE 2000/20 ms, FOV 230 × 220 mm, matrix 296 × 200); (d) coronal T2W TSE (TR/TE 3000/80 ms, FOV 250 × 190 mm, matrix 436 × 300); and (e) axial FLAIR IR (TR/TE 11,000/120 ms, inversion time (TI) 2800 ms, FOV 220 × 220 mm, matrix 512 × 512). Single-shot spin echo-echo planar imaging (SE-EPI) was used in DTI. Scan layers were aligned parallel to the anterior/posterior line with the following settings: TR/TE 6518/60 ms, FOV 256 × 256 mm, thickness 2 mm, matrix 256 × 256, SENSE factor 2, 15 non-linear directions, b value of 0 and 800 s/mm2, respectively. To increase signal-to-noise ratio, scanning was repeated three times (total time = 4 min 13 s).
The postprocessing Fiber Trak software was used to measure FA and ADC values in different layers of B0 map and color-coded map on the axial images in three groups. We placed 10 rectangular ROIs (size ranged from 30 to 40 mm2, containing 6–10 pixels) in subcortical regions (Fig. 1) that included the prefrontal lobe, temporal lobe, parietal lobe, occipital lobe, hippocampus, and various association tracts (Fig. 2). These latter included the inferior-fronto-occipital fascicles (IFOF), genu, and splenium of the corpus callosum (GCC, SCC), superior longitudinal fasciculus (SLF), and the cingulate fasciculus (CF). The non-midline regions were measured on both sides. An experienced neuroradiologist, blinded to the diagnosis, performed the placements of the ROI for FA and ADC. Each ROI was controlled under two voxels in all tracts.
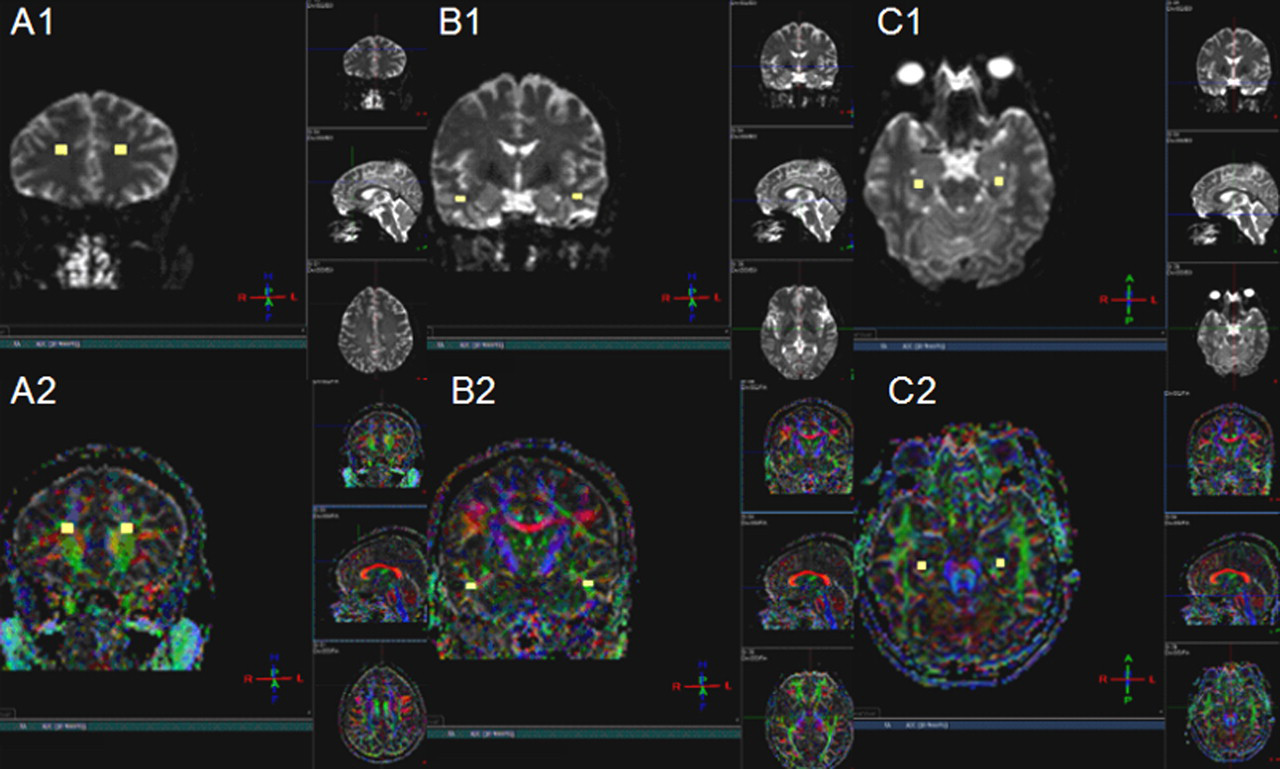
The ROIs B0 image (A1–C1) and color-coded map (A2–C2) in the white matter of the prefrontal lobe, temporal lobe and hippocampus in the SIVD group
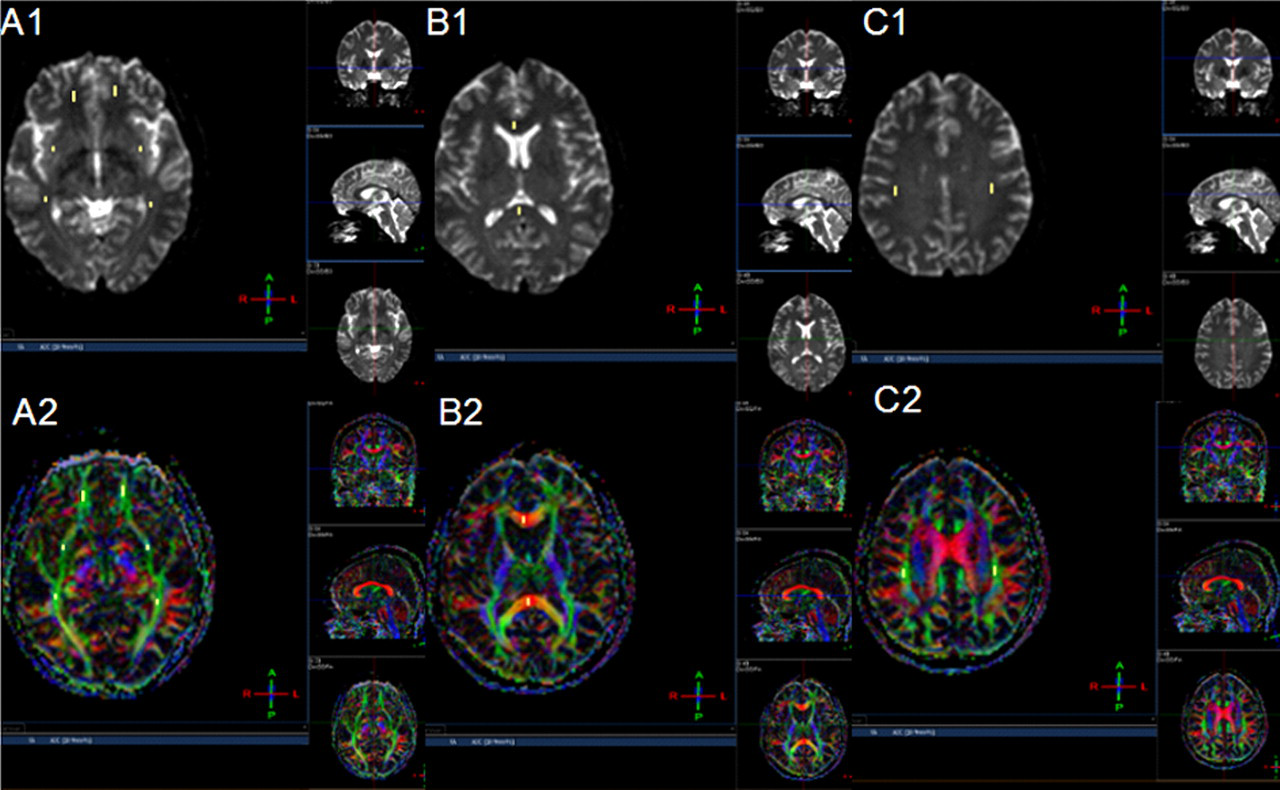
The ROIs B0 image (A1–C1) and color-coded map (A2–C2) in the association fiber tracts of the inferior-fronto-occipital fascicles, genu and splenium of corpus callosum and superior longitudinal fasciculus in the SIVD group
Data were analyzed using the Statistical Package for Social Sciences (SPSS for Windows, Version 15.0, SPSS, Chicago, IL, USA). Statistical analyses were performed on FA and ADC values by one-way analysis of variance (ANOVA) followed up with post hoc LSD (least significant difference) tests for multiple comparisons. For all the analyses, statistical significance was accepted at P < 0.05.
Results
There were no significant differences in FA and ADC values in the symmetrical regions within each group. Compared to controls, patients with SIVD had reduced FA values and increased ADC values in the IFOF, GCC, SCC, and CF (P < 0.05). Compared to controls, AD patients showed reduced FA values in the anterior frontal lobe, temporal lobe, hippocampus, IFOF, GCC and CF, and increased ADC values in the temporal lobe and hippocampus (P < 0.05). Compared to the AD group, SIVD patients showed a diffuse increase of ADC values in some areas, including the IFOF, GCC, SCC, and SLF, while increased ADC values were found in the AD group in the temporal lobe and hippocampus (P < 0.05) (Tables 2 and 3).
FA across the three groups
Each value shows the mean ± S.D
ANOVA was used to compare the difference among three groups
Between patients and age-matched controls, *P < 0.05
Between AD patients and SIVD patients, † P < 0.05
NC = normal controls, AD = Alzheimer's disease, SIVD = subcortical ischemic vascular dementia, IFOF = inferior fronto-occipital fascicles, GCC = corpus callosum genu, SCC = corpus callosum splenum, SLF = superior longitudinal fasciculus, CF = cingulate fasciculus
ADC across the three groups
Each value shows the mean ± S.D
ANOVA was used to compare the difference among three groups
Between patients and age-matched controls, *P < 0.05
Between AD patients and SIVD patients, † P < 0.05
NC = normal controls, aMCI = amnestic mild cognitive impairment, AD = Alzheimer's disease, SIVD = subcortical ischemic vascular dementia, IFOF = inferior fronto-occipital fascicles, GCC = corpus callosum genu, SCC = corpus callosum splenum, SLF = superior longitudinal fasciculus, CF = cingulate fasciculus
Discussion
Making the differential diagnosis may be difficult in patients with SIVD or AD who show only mild signal intensity alterations in the white matter on T2WI. Thus, in the present study, we used sophisticated image processing algorithms to identify and compare the regional pattern of FA changes between patients with different types of dementia and normal controls.
Distinct patterns of white matter abnormalities were found in the patients in each of the three groups. Compared to elderly individuals with normal cognitive function, SIVD patients had diffusion tensor changes in both the anterior and posterior cerebral white matter, including the IFOF, GCC, SCC, and SLF. Multiple lesions in the corpus callosum can cause memory impairment and personality changes. Furthermore, the abnormal integrity of the SLF can cause impairments in spatial attention and spatial working memory. The subcortical thalamic-basal-prefrontal circuits are particularly important as dysfunction in these might result in the main cognitive, behavioral, and clinical neurological features of SIVD (4). An attractive hypothesis to explain cognitive impairment in patients with cerebral small vessel disease is that white matter tract damage results in a ‘disconnection syndrome’, owing to the interruption of large tracts of cerebral nerve fibers. Our results, in line with previous hypotheses, provide additional evidence that damage to white matter projections is an important mechanism of cognitive impairment, and they are consistent with the ‘disconnection’ hypothesis of cognitive impairment in patients with small vessel disease.
The results of our study show that SIVD patients have significantly different average ADC values and average FA histograms of the brain compared with control groups. These findings are consistent with the results of other studies (3, 11). Sugihara et al. reported that FA values of the anterior white matter tended to be lower than those of the posterior white matter in patients with vascular dementia (18). The discrepancy between this finding and our own might be due to differences in the study group selection, and the fact that different diagnosis criteria were adopted. However, the multiple diffusion tensor changes were specific for SIVD, which highlighted its clinical and neuropsychological features, characterized by extensive arteriole occlusions and micro-atherosclerosis, which can cause multiple lacunar infarcts and white matter lesions, extensive demyelination, and axonal loss. Beyond the findings from traditional imaging and neuropsychological testing, DTI can serve as a sensitive technique for early detection of cognitive decline in SIVD patients.
Our DTI study has also provided evidence of white matter anisotropy decline in the anterior frontal lobe, temporal lobe, hippocampus, IFOF, GCC, and CF in AD patients, which correlates with the results of previous studies (3, 10, 11, 13, 19). Reduced FA values in the anterior frontal lobe, temporal lobe and hippocampus in AD patients indicates a net loss of barriers that normally restrict the movement of water molecules and can be explained by temporal-frontal disconnections (13). Increased ADC values in the temporal lobe, and hippocampus in AD group were also observed. This may have been the result of a decreased number of neurons and a consequently enlarged tissue space. In particular, although the precise neural correlates of altered diffusivity measurements have not been previously described with respect to neurodegeneration, increased ADC values most likely result from the loss of neurons, axons, and dendrites, which is thought to produce an increased extracellular space and elevated water diffusivity within these regions (8). It has been suggested that the pathological processes of AD begin in medial temporal structures (entorhinal cortex and hippocampus), advance to the temporal cortex, and then affect posterior parietal lobes, and finally the different levels of frontal lobe of the cerebral cortex. Our results are consistent with this paradigm.
In order to eliminate subjective errors, an experienced neuroradiologist, who was blinded to the clinical diagnosis of participants, placed the ROIs following strict criteria. However, our study had several limitations. First, we used anisotropic voxels for the DTI, and this might have biased the FA calculation. A histogram-based approach or a voxel-based statistical approach can be used to reduce some of the problems of ROI analysis. Second, the SIVD patients with severe T2 hyperintensities were excluded from in this study. This may have generated some bias for the results. However, the aim of this study was to evaluate the value of DTI in making the diagnosis of dementias and differentiating between SIVD and AD. In order to eliminate the influence of the subjective, patients with similar T2 hyperintensities were enrolled. Finally, our study was limited by the relatively small number of enrolled patients. Future studies should adopt larger sample sizes for groups of patients.
In conclusion, there were significant regional reductions of FA values and heightened ADC values in multiple neural regions in SIVD patients compared to AD patients. DTI may thus provide a more objective method for the differential diagnosis of SIVD and AD.
Footnotes
Acknowledgments
This work was supported by grants from the Science and Technology Commission of Shanghai Municipal Health Bureau (No. 2008094), and in part from the Science and Technology Commission of Shanghai Municipality grant (No. 08411951200).