
Abstract
Spinal cord injury is a rare complication of chiropractic treatment. This case report describes a 50-year-old man who developed neurological symptoms a few hours after manipulation (high velocity low amplitude [HVLA] technique) of the cervical spine. Magnetic resonance (MR) imaging of the cervical spine revealed intramedullary high signal at the C2/3 level of the right side of the cervical cord on the T2-weighted images. The potential mechanism of injury and causes of the radiological appearance are discussed.
Cervical manipulation is one of the tools frequently used by chiropractors. Some concerns about the safety of the procedure have been expressed in the literature (1–5). We report on an unusual case of spinal cord injury that followed chiropractic manipulation to the neck.
Case report
A 50-year-old man was referred by his general practitioner for an urgent neurological assessment. He described a one-week history of an electric shock sensation and numbness in the left lower limb, spreading up to the left pectoral region. No bladder or bowel disturbances were reported. The patient was not aware of any obvious trigger for the symptoms, but he was receiving chiropractic treatment for low back pain and had undergone neck manipulation a few hours before the onset of symptoms.
Neurological examination of the cranial nerves and the upper limbs was unremarkable. In the lower limbs bulk, tone, strength, and coordination were normal, and the plantar responses were flexor. On sensory testing there was left-sided hyperaesthesia to pinprick and impaired temperature sensation involving the left lower limb extending to the pectoral region of the trunk. Joint position sense in the hands and feet was preserved. His gait was normal.
The patient was referred for MR imaging of the cervical and thoracic spine. This showed loss of the cervical lordosis with multi-level degenerative changes, with posterior disc and osteophytic bars from the C3/4 to the C7/T1 levels. There was indentation of the anterior thecal sac, but no evidence of cervical cord compression. Intramedullary high signal on the right side of the cord was shown at the C2 and C3 levels on the T2-sagittal and axial-weighted images. Mild swelling of the cord at this level was also demonstrated (Figs. 1 and 2). No other intramedullary high signal was seen elsewhere in the cervical or thoracic spinal cord. An MR brain performed four months after the initial onset of symptoms did not reveal any abnormality.
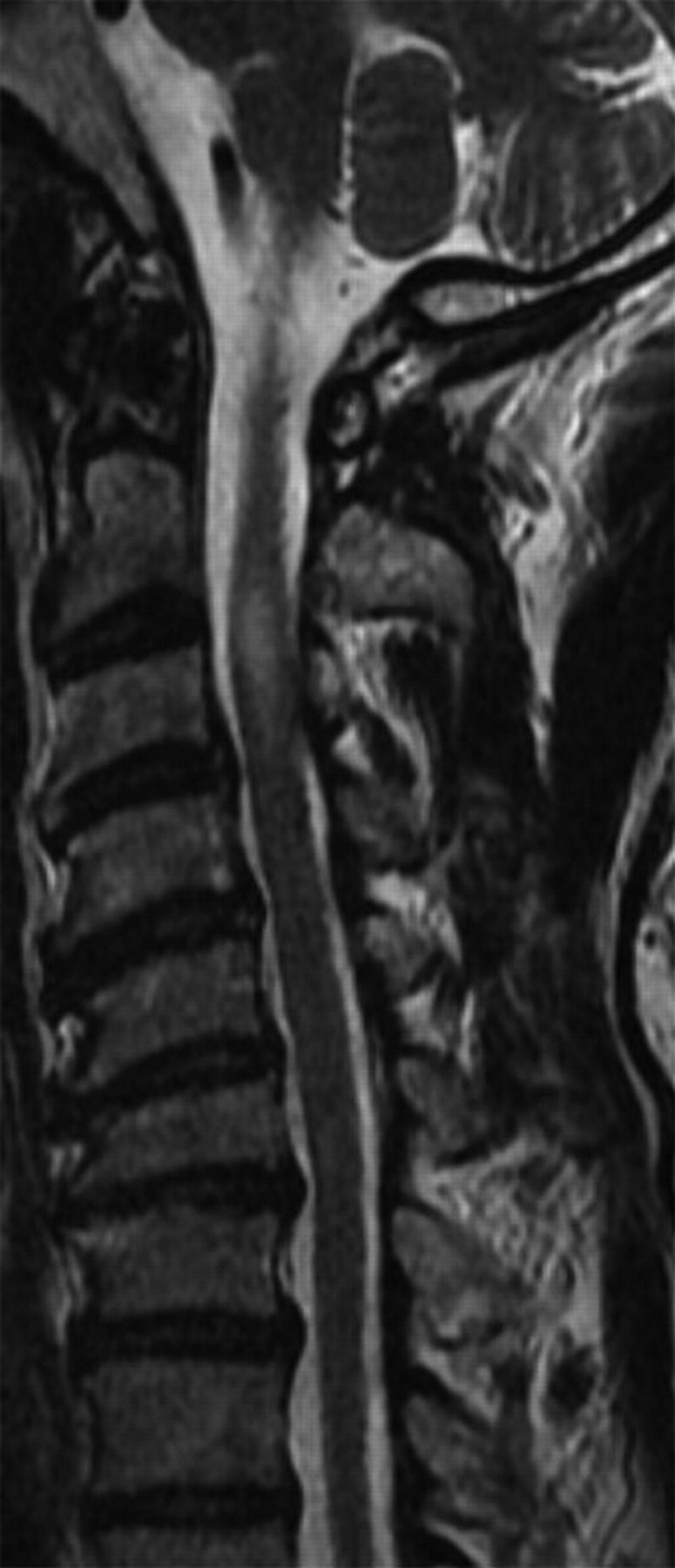
T2 sagittal image of the cervical spine showing high intramedullary signal at C2/3 level and degenerative change from C3/4 to C7/T1
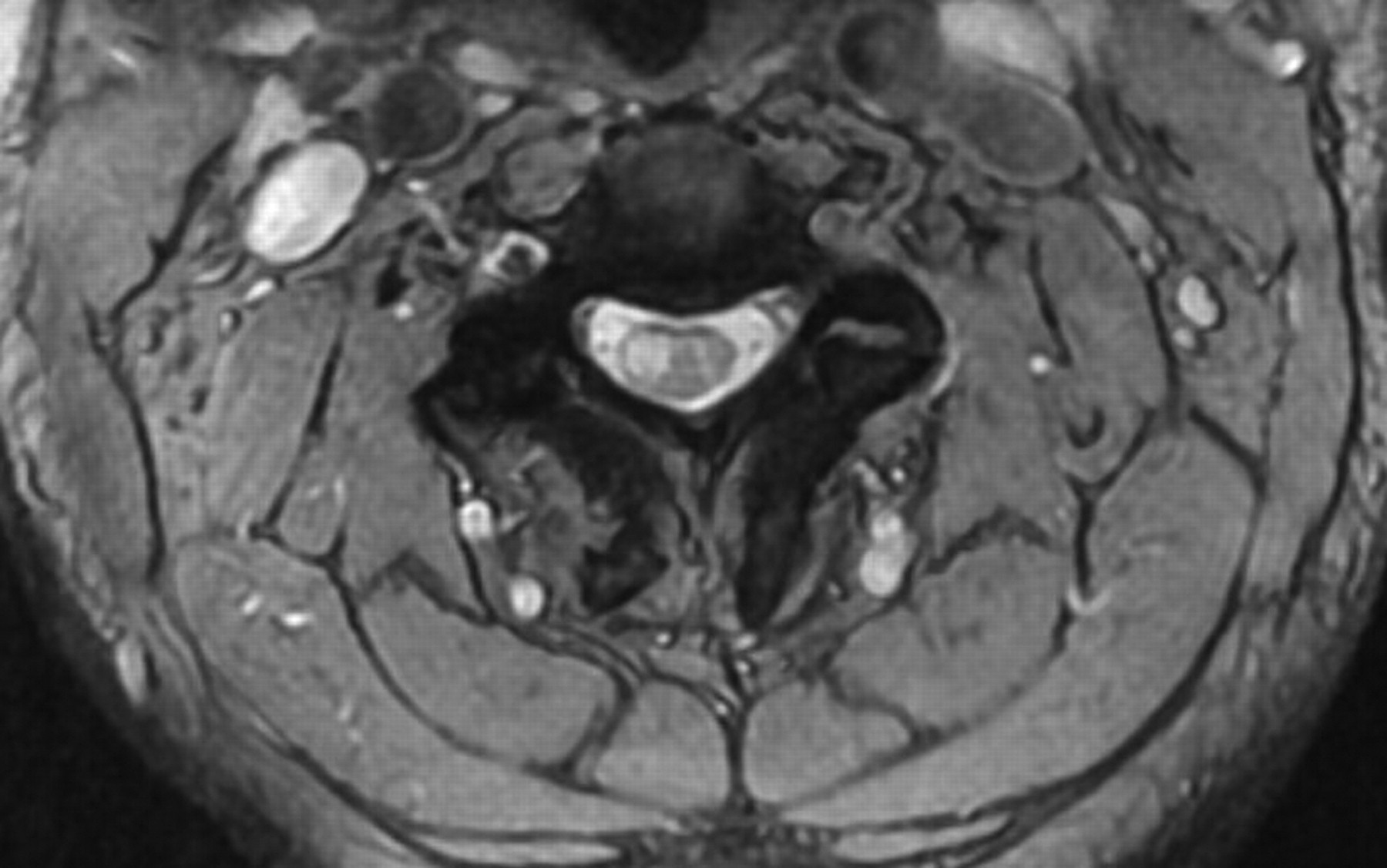
T2* axial image at C2/3 showing high intramedullary signal in the right hemicord
Discussion
Chiropractic intervention is a popular alternative therapy for musculoskeletal pain and approximately 12% of the population receive treatment each year in the United States (4, 5). Chiropractors use the high velocity low amplitude (HVLA) thrust technique to treat patients who present with neck pain. Most patients do not experience adverse events but some concerns regarding the safety of the procedure have been expressed in the literature (1–5). A number of randomized controlled trials, with regard to efficacy have been performed, but the results are often inconclusive, due to poor methodological design (4, 5).
In our case the patient underwent HVLA treatment to the cervical spine. This involves composite movements of extension, lateral flexion, and rotation, with the rotation component exaggerated at the time of the ‘thrust’ maneuver. Gouveia et al., in their systematic review of chiropractic intervention, concluded that complications were frequent, but often mild or transitory (4). Of the more serious adverse events, cerebrovascular incidents have been well reported in the literature and form the basis of concern regarding HVLA treatment to the cervical spine (1–5). Non-vascular complications following chiropractic intervention are less well described (6).
This case illustrates an unusual complication following cervical HVLA treatment. Although the MR findings of high signal in the cervical hemicord are somewhat non-specific, the temporal association of the manipulative treatment and the onset of neurological symptoms suggest a causal link. The MRI of the brain did not reveal a clinically silent inflammatory or demyelinating process to suggest an alternative diagnosis.
There were no motor signs by the time the patient was seen in clinic but the clinical finding of pain and temperature loss contralateral to the side of the lesion would be consistent with an incomplete Brown-Séquard syndrome. To our knowledge, only three cases of Brown-Séquard syndrome following chiropractic care have previously been reported in the literature (7–9). Two of these cases resulted from an expanding epidural hematoma (8, 9) that was not evident in our case.
We suggest two plausible mechanisms of injury to explain the clinical and radiological findings in this case. Firstly, the thrust maneuver on the degenerative cervical spine may have produced an asymmetrical vector force load on the cervical spinal cord resulting in contusion. The posterior disc and osteophytic bar at the C3/4 level certainly corresponds to the intramedullary cord high signal and cord swelling shown at the level C2/3 on MRI.
Damage to the cervical radicular arteries resulting in spinal cord ischemia or infarction is an alternative explanation. The cervical radicular arteries arise from both the ascending cervical artery and the vertebral artery and are known to anastomose with the anterior spinal artery (10). The vertebral artery runs a particularly tortuous course once it exits the foramina in the transverse processes of the cervical spine at C2, and shear forces resulting from cervical manipulation have been associated with vertebral artery dissection (1–5). These same forces may also disrupt the cervical radicular arteries as they branch off the vertebral artery.
Although this case illustrates a rare complication, it is sufficiently serious to further question the safety of chiropractic manipulation of the neck. As with all medical interventions, the benefits for the patient must outweigh any perceived risk. Best practice dictates that chiropractors must be mindful of the requirement for obtaining informed consent prior to the application of this procedure. Some therapists already advocate screening patients for risk factors before treatment, e.g. vertebro-basilar arterial provocation testing prior to manipulation (11), but these protocols are neither reliable nor accurate (1). The role of imaging is also not clear, but arguably MR examination of the cervical spine, with its excellent soft tissue contrast resolution would constitute a suitable approach to the pre-manipulative assessment of the cervical spine, although this will be perceived by many to be both costly and impractical. Nevertheless, patients presenting with acute neurological deficit following chiropractic care should be referred for urgent MR imaging.