
Abstract
Background
Metaplastic carcinomas are ductal carcinomas that display metaplastic transformation of the glandular epithelium to non-glandular mesenchymal tissue. Metaplastic carcinoma has a poorer prognosis than most other breast cancers, so the differential diagnosis is important. Although many clinical and pathologic findings have been reported, to our knowledge, few imaging findings related to metaplastic carcinoma have been reported.
Purpose
To investigate whole-breast imaging findings, including mammography, sonography, MRI, and pathologic findings, including immunohistochemical studies of metaplastic carcinomas of the breast.
Material and Methods
We analyzed 33 cases of metaplastic carcinoma between January 2001 and January 2011. Mammography, ultrasonography, and MRI were recorded retrospectively using the American College of Radiology (ACR) breast imaging reporting and data system (BI-RADS) lexicon. Immunohistochemical studies of estrogen receptor (ER), progesterone receptor (PR), p53, and C-erbB-2 were performed.
Results
The most common mammographic findings were oval shape (37%), circumscribed margin (59%), and high density (74%). The most common sonographic findings were irregular shape (59.4%), microlobulated margin (41%), complex echogenicity (81%), parallel orientation (97%), and posterior acoustic enhancement (50%). Axillary lymph node metastases were noted for 25% of the sonographic examinations. On MRI, the most common findings of margin and shape were irregularity (57% and 52.4%, respectively). High signal intensity was the most common finding on T2-weighted images (57%). Immunohistochemical profile was negative for ER (91%, 29/32) and PR (81%, 26/32).
Conclusion
Metaplastic carcinomas might display more benign features and less axillary lymph node metastasis than IDC. High signal intensity on T2 MRI images and hormone receptor negativity would be helpful in differentiating this tumor from other breast cancers.
Metaplastic carcinomas are ductal carcinomas that display metaplastic transformation of the glandular epithelium to non-glandular mesenchymal tissue (1–6). Metaplastic carcinoma is a rare form of breast cancer, accounting for less than 5% of all breast cancers (1–5). Wargostz et al. (7) reported five types of metaplastic carcinomas: matrix-producing carcinoma, squamous cell carcinoma, spindle cell carcinoma, carcinosarcoma, and metaplastic carcinoma with osteoclastic giant cells. Oberman (8) suggested that all tumors with metaplastic components of mesenchymal or epithelial origin should be categorized as metaplastic carcinomas. The common types of metaplastic carcinomas are squamous, spindle cell, and matrix-producing. The rare types involve osseous or sarcomatous changes (1, 9, 10).
Metaplastic carcinoma has a poorer prognosis than most other breast cancers; the differential diagnosis is important (1–4). The distinction between metaplastic carcinoma and sarcoma is important because of the considerable differences in their natural histories, surgical treatments, and chemotherapy plans (1, 4). In breast sarcoma, axillary lymph node involvement is rare, whereas axillary lymph node involvement is not rare in metaplastic carcinoma (1, 4).
Although many clinical and pathologic findings have been reported, to our knowledge, few imaging findings related to metaplastic carcinoma have been reported (1–4, 6, 11, 12). The purpose of this study was to investigate whole-breast imaging findings, including mammography, sonography, MRI, and pathologic findings, including immunohistochemical studies.
Material and Methods
A search of our computerized pathology database identified 45 metaplastic carcinoma patients seen between January 2001 and January 2011. Seven patients were excluded because the pathologic diagnosis of the specimen was invasive ductal carcinoma (IDC) or ductal carcinoma in situ (DCIS), despite confirmation as metaplastic carcinoma by a core-needle biopsy. Five patients were excluded because the images were not retained.
For the mammograms, standard craniocaudal and mediolateral oblique views were obtained using a Mammomat 3000 (Siemens Medical Solutions, Solna, Sweden) and a Lorad M3 mammography unit (Hologic, Inc., Boston, MA, USA). The ultrasound images were acquired using a 5–12 MHz linear probe (HDI 5000, Advanced Technology Laboratories; Bothell, WA, USA/ IU22 Ultrasound System, Philips Ultrasound; Bothell, WA, USA). All mammograms and sonograms were retrospectively reviewed by one radiologist with 5 years' experience in breast imaging. Parenchymal patterns on mammograms were categorized; almost entirely fatty, as pattern 1; scattered fibroglandular tissue, as pattern 2; heterogeneously dense, as pattern 3; extremely dense, as pattern 4. Each mammographic lesion was analyzed according to mass characteristics (shape, margin, density), presence and architectural distortion, mass and type of microcalcifications according to the American College of Radiology (ACR) breast imaging reporting and data system (BI-RADS) lexicon. According to the ACR BI-RADS, the margin of a mass is described as circumscribed when over 75% of margins are sharply demarcated with an abrupt transition between the lesion and the surrounding tissue, as indistinct when the poor definition of the margins raises concern that there may be infiltration by the lesion and this is not likely due to superimposed normal breast tissue, and as obscure when one which is hidden by superimposed or adjacent normal tissue and cannot be assessed any further. Asymmetry is defined as a density that cannot be accurately described using the other shapes and especially when asymmetry of tissue density is visible with similar shape on two views, but completely lacking borders and the conspicuity of a true mass.
Sonographic images were reviewed for features such as shape, orientation, margin, boundary, echo pattern, posterior echo features, and associated calcifications, and were categorized using the ACR BI-RADS lexicon. We diagnosed positivity for metastasis in the axillary lymph node when it displayed focal hypoechoic cortical lobulation and a completely hypoechoic node with no hilum (13).
MRI was performed with a 1.5 T scanner (Signa Excite, GE Healthcare, Milwaukee, WI, USA) equipped with a breast coil. Images were acquired in axial and sagittal planes with the following sequences: axial T2-weighted fat-suppressed fast spin echo imaging (TR/TE = 5000/86, a flip angle of 90°, a field of view [FOV] of 300 mm, a matrix of 256 × 256, number of excitations [NEX] of 1, 4.5-mm slice thickness); pre- and post-contrast axial spin-echo T1-weighted images (TR/TE = 6.5/3.1, flip angle of 10°, FOV of 300 mm, matrix of 350 × 350, 0 NEX, and 1.1-mm slice thickness). The presence of abnormal enhancement was classified according to the BI-RADS MRI lexicon (14). Time-signal intensity curves of the lesions were recorded by visual analysis and were classified on the basis of their shape as steady (type I), plateau (type II), or wash-out (type III) (15).
Histopathologic diagnosis was confirmed by core-needle biopsy, excision biopsy, lumpectomy, and mastectomy. When both core-needle or excision biopsy and surgery were performed, surgery was considered the gold standard. When surgery was not performed, excision biopsy and core-needle biopsy were considered the gold standard, in that order. The microscopic slides of patients were reviewed in consensus by two pathologists who are specialists in breast pathology. Axillary lymph node metastasis was evaluated at the dissected lymph node specimen, which included the sentinel axillary lymph node. Immunohistochemical studies of estrogen receptor (ER), progesterone receptor (PR), p53, and C-erbB-2 were performed in 32 patients.
Results
All 33 patients were aged 33–71 years (mean age 52.7 years). The presenting complaint was palpable mass in 25 patients. One patient underwent a routine follow-up after surgery for breast cancer, and seven patients were submitted due to screening mammograms.
Mammograms were available for 30 patients. The breast parenchyma was shown to comprise solely fatty breast tissue in three patients, scattered fibroglandular tissue in 11 patients, heterogeneously dense breast tissue in 13 patients, and extremely dense breast tissue in three patients. The characteristics of these masses are described in Table 1. The most common findings according to the ACR BI-RADS are oval shape (37%), circumscribed margin (59%), and high density (74%) (Fig. 1a). Microcalcifications were noted in 23% of specimens, with pleomorphic shape in 5/7 (Fig. 1a), linear shape in 1/7, and round shape in 1/7.
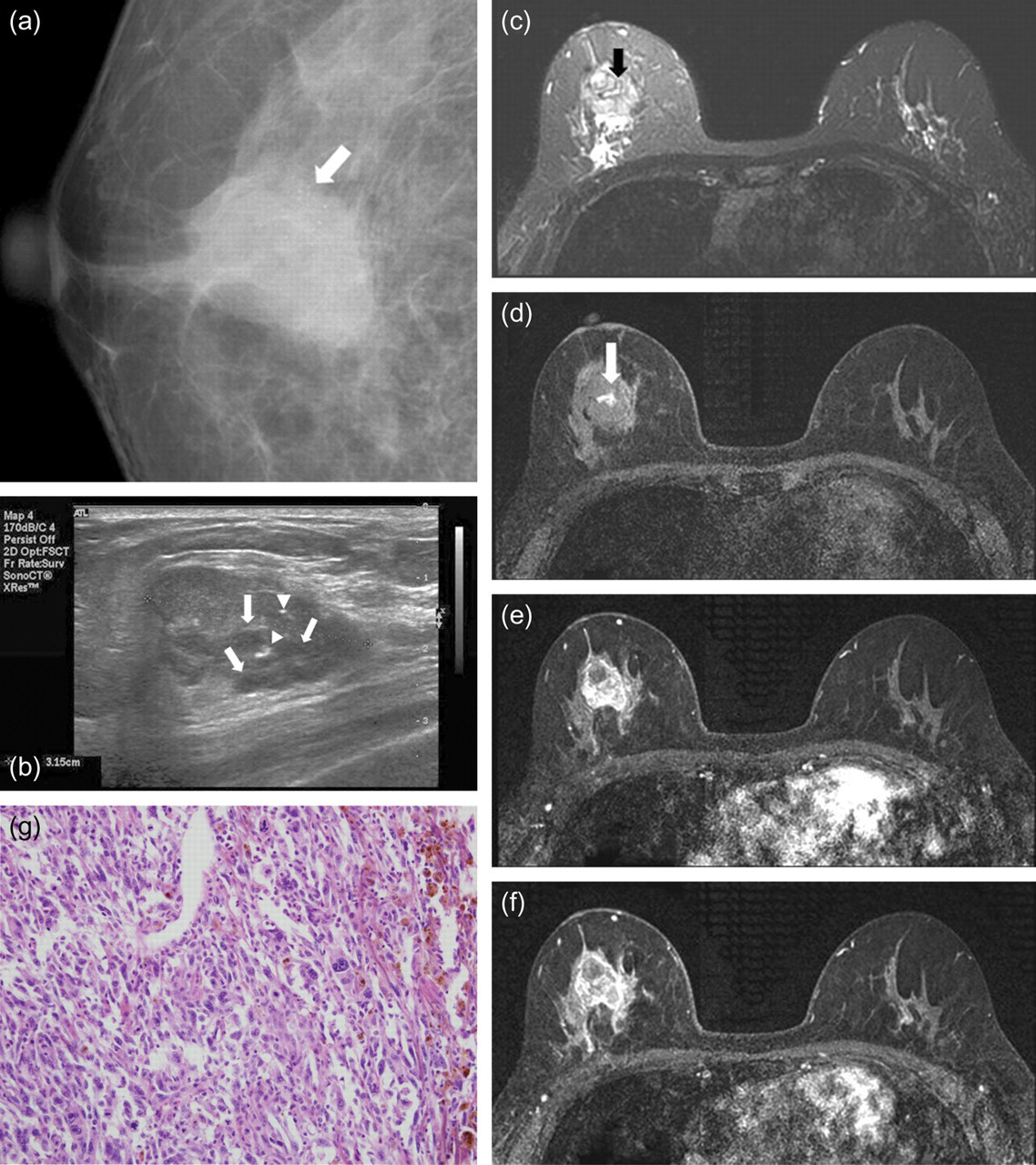
Metaplastic carcinoma of the right breast who presented a palpable lump in a 54-year-old woman. (a) Craniocaudal mammogram of the right breast shows a circumscribed oval high density mass in central portion. Multiple pleomorphic calcifications are seen in the mass (arrow); (b) Ultrasonogram of the right breast shows a 3 cm irregular microlobulated mass at the 12 o'clock direction. Note the presence of multiple small cystic spaces in the predominantly solid mass (arrows). Also multiple calcifications are seen in the mass (arrowheads); (c) Axial fat-suppressed T2-weighted MR image shows irregular mass with areas of high signal intensity (arrow); (d) Axial fat-suppressed T1-weighted MR image demonstrates mass isointense relative to surrounding fibroglandular tissue. Note the high signal intensity area in the mass, which suggests hemorrhage (arrow). (e, f) Axial fat-suppressed T1-weighted MR images with contrast injection after 2 min (e) and 6 min (f) show delayed washout kinetic pattern of enhancement; (g) Photomicrograph shows pleomorphic spindle cell differentiation areas composed in most of the mass (hematoxylin-eosin stain, × 200)
Correlation between mammographic findings and tumor types of 33 metaplastic carcinomas
The most common sonographic findings were irregular shape (59.4%), microlobulated margin (41%), complex echogenicity (81%), parallel orientation (97%), and posterior acoustic enhancement (50%) (Fig. 1b, 2 and 3b) (Table 2). The complex echogenicity consisted of a predominantly solid mass with eccentric cystic spaces (Fig. 1b) in 38% of the patients and a mixed cystic and solid mass (Fig. 2) in 4% of the patients. Most complex echogenicity (54%) consisted of multiple tiny cystic areas scattered throughout the mass, similar to phyllodes tumor (Fig. 3b).

Metaplastic carcinoma in a 53-year-old woman with palpable mass in right breast. Ultrasonography of right breast shows about 7.0 cm sized microlobulated hypoechoic mass with complex echogenicity at the 8 o'clock direction. The complex echogenicity consisted of mixed cystic and solid mass

Metaplastic carcinoma in a 52-year-old woman with palpable mass in her right breast. (a) Craniocaudal mammogram of right breast shows a lobular high density mass in outer portion; (b) Ultrasonography of right breast reveals an irregular microlobulated hypoechoic mass with complex echogenicity. The complex echogenicity consisted of multiple tiny cystic spaces scattered throughout the mass (arrows)
Correlation between sonographic findings and tumor types of 33 metaplastic carcinomas
MRI was performed in 21 patients, and all showed masses (Table 3). The most common findings of margin and shape were irregularity (57% and 52.4%, respectively). High signal intensity was the most common finding on T2-weighted images (57%) (Fig. 1c); 71.4% of the cases showed intermediate signal intensity on T1-weighted images (Fig. 1d). The most common internal enhancement pattern was heterogeneous in 71% of the cases. The most common delayed enhancement pattern on kinetic curve analysis was the wash-out pattern (67%) (Fig. 1e and 1f).
Correlation between MRI findings and tumor types of 33 metaplastic carcinomas
Final pathologic diagnosis was obtained by mastectomy in 23 patients, lumpectomy in eight patients, excision biopsy in one patient, and core-needle biopsy in one patient. The cell type of metaplastic carcinoma was squamous in 18 patients, matrix-producing in 10 patients, other heterogeneous (squamous + spindle-cell type in 1, spindle + osseous in 1, myxoid matrix + sarcoma in 1, spindle + neuroendocrine in 1 [Fig. 1g]) in four patients, and not defined in one patient. Axillary lymph node dissection was performed in 32 patients, and metastasis was reported in eight patients. Immunohistochemical profile was negative for ER (91%, 29/32) and PR (81%, 26/32), and positive for p53 (81%, 26/32) and C-erbB-2 (84%, 27/32).
Discussion
Most benign and malignant breast tumors originate from glandular epithelium. In some cases, glandular epithelium can differentiate to non-glandular mesenchymal tissue, a process called metaplasia. Metaplastic carcinoma is a type of ductal carcinoma displaying metaplastic changes including squamous differentiation, a spindle-cell pattern of growth, and/or heterogeneous mesenchymal morphological elements (2, 4). The most common metaplastic change is known as squamous metaplasia, with an incidence of 0.5–3.7% (2, 8). Spindle-cell and matrix-producing types are also frequently reported but osseous or sarcomatoid metaplasia are rarely observed (10–12). In our study, the most common metaplastic components were squamous metaplasia (45%), followed by the matrix-producing type (30%). The spindle cell type was noted in three cases (9%) with a mixture of squamous (1 patient), osseous (1 patient), or neuroendocrine (1 patient) cells. Therefore, the results of our study are similar to those of previous reports.
Metaplastic carcinomas present at approximately 50 years of age in women (1, 3, 5, 8). The ages of our patients ranged from 33 to 71 years (mean 53 years), which was similar to previous studies. Clinically, metaplastic carcinoma grows rapidly and presents as a palpable mass (3, 5, 9). In our study, 25 out of 33 patients (76%) complained of palpable masses.
On mammography, metaplastic carcinomas show more circumscribed margins than invasive ductal carcinomas (IDCs), although metaplastic carcinomas may display irregular or spiculated margins (1, 2, 4, 16, 17). Sonographic features are oval, round, or lobular shaped, circumscribed or indistinct marginated masses, which display more benign features than IDCs (4, 18). Posterior enhancement is common; with such features, metaplastic carcinoma may be misinterpreted as a benign lesion (18). In our study, the most common mammographic features of metaplastic carcinoma were oval shape with a circumscribed margin and a high density; these characteristics are similar to previous reports. Without circumscribed margins, a spiculated margin was the most common finding (18%). Park et al. (4) and Gunhan-Bilgen et al. (3) reported that metaplastic carcinoma may be observed with an obscured or microlobulated margin. Those findings were also seen in our study (19%). Petterson et al. (1) said that metaplastic areas of metaplastic carcinoma are related to a circumscribed or lobular appearance and irregular or spiculated margins are considered the IDC component of metaplastic carcinoma if metaplastic and invasive ductal carcinomas are mixed. The authors reported that a circumscribed margin reflects the spindle-cell component of metaplastic carcinoma (1). In our study, two cases out of three of spindle cell carcinoma displayed circumscribed margins; the other case displayed an obscured margin on mammography. All three cases showed microlobulated margins on sonography, which was somewhat different from the results reported by Petterson et al. (1). The spindle cell type was observed in only three cases, mixed with other cell types, which prevented a comparison with other reports. Five cases of metaplastic carcinoma displayed spiculated margins on mammography and ultrasonography. Among these cases, four cases were mixed with IDC and one was not. As metaplastic carcinoma with mixed IDC was observed in 70% of the samples (23/33), the IDC component may be one of the reasons but not the only reason for the presence of a spiculated margin.
The most common findings on ultrasonography were irregular shape, microlobulated margin, and posterior acoustic enhancement. Previous studies have reported metaplastic carcinoma to display oval, round, or lobular shape, and circumscribed or indistinct margins; thus, our result are inconsistent with these previous findings (4, 18). Few signs of malignancy, such as spiculated or angular margin or posterior shadowing, were observed (19). Yang et al. (18) reported that suspicious malignant findings such as irregular shape, angular margin, and posterior acoustic shadowing were less common in metaplastic carcinoma samples than in IDC, and findings associated with benign growths, such as circumscribed margins or posterior acoustic enhancement, were frequent. Recent reports demonstrated that more circumscribed masses may be of a higher histologic grade, while lesions that appear benign may in be aggressive malignancy associated with poor prognoses and survival rates (9, 18, 20–23). Therefore, the benign features of metaplastic carcinoma may reflect tumor aggressiveness and a worse prognosis.
Metaplastic carcinomas show complex echogenicity with solid and cystic components (3, 4). The complex echogenicity of metaplastic carcinoma is typically reported as one of two types: predominantly solid mass with eccentric cystic spaces or mixed cystic and solid mass (3, 4, 8, 17). In our study, 81% of samples displayed complex echogenicity. The two types outlined above were seen in 38% and 4% of patients, respectively. The most common type in our study was solid mass with multiple tiny cystic spaces throughout the mass, similar to phyllodes tumor (54%). Cystic areas display necrosis, hemorrhage, or cystic degeneration (3, 4, 8, 17). Some authors have reported that cystic areas are associated with squamous components (24, 25). However, we did not find any relationship between a complex echo pattern and metaplastic components.
Microcalcification is less common than IDC, especially malignant calcifications that are pleomorphic or linear in shape (1, 4, 18). We found associated microcalcifications in 23% of patients, similar to the reports of Park et al. (4) (25%) or Yang et al. (18) (25%). The calcification is most commonly pleomorphic (71%, 5/7), in contrast to the report by Yang et al. (18). However, the case number is too small to correlate with previous studies or to generalize.
On MR images, masses may show high signal intensity on T2-weighted images. This result is due to the necrotic component of the mass (26, 27). In our study, high T2 signal intensity was seen in 57% of specimens, an incidence rate much lower than that reported by Velasco et al. (26) (91%). Velasco et al. (26) subdivided T2 high signal intensity patterns as homogeneous intra-tumoral high signal intensity (e.g. simple cyst) (Fig. 3) and mottled high signal intensity showing hyper-signal areas mixed with hypo- or iso-signal areas (Fig. 1). The corresponding incidences were reported as 16% (2/12) and 75% (9/12), respectively. As our results were 24% (5/21) and 33% (7/21), respectively, there was some discrepancy between our results and those reported by Velasco et al. (26). Furthermore, intermediate signal intensities were observed on T2-weighted images more frequently in our study than reported by Velasco et al. (26) (43% vs. 8%). This discrepancy is because of the increased number of cases in our study as well as the differences in the complex echogenic patterns visualized using sonography. In our study, complex echogenicities showing diffusely scattered tiny cystic areas were dominant pattern, and those patterns were presented as intermediate signal intensity on T2-weighted images in 42% of patients (5/12). In our study, high signal intensity on T2-weighted images was a more frequent finding than indeterminate signal intensity. Breast cancers showing high T2 signal intensity are known as mucinous carcinoma, IDC with infarction or necrosis, intracystic papillary carcinoma, and invasive papillary carcinoma, in addition to metaplastic carcinoma (28). Differentiation of such tumors on images would be difficult, and immune study might be helpful. We will discuss the immune study of metaplastic carcinoma below.
The most common internal enhancement pattern was heterogeneous enhancement (71%). Rim enhancement was noted in 19% of the cases; these masses were complex echoic masses with large cystic portions on sonography. As reported by Im et al. (27), rim enhancement was due to non-enhancing central necrosis or hemorrhagic components and enhancing solid portions in the peripheral areas of the tumor. Many complex echoic masses with tiny scattered cystic areas displayed heterogeneous enhancement because multiple rim enhancements of tiny cystic walls may appear as heterogeneous enhancement overall. The most common patterns on kinetic curve analysis were wash-out and persistent patterns. Velasco et al. (26) reported plateau and wash-out patterns as common findings, but the kinetic curve analysis of metaplastic carcinoma performed in that study was not specific for this tumor.
Metaplastic carcinomas display different biological behavior from IDC (18). Metaplastic carcinomas tend not to express estrogen and progesterone receptors and display less regional LN involvement (2, 8, 18). Reported axillary lymph node metastasis is observed in about 25–40% of patients, which is less than IDC (2, 4). Negativity for estrogen and progesterone receptor is related to prognosis, and expression of the p53 mutation and C-erbB-2 protein is related to prognosis and survival rate (29). In our cases, most metaplastic carcinomas did not express estrogen or progesterone receptors, and over 80% of metaplastic cancers were positive for the p53 mutation and C-erb-B. Those results are similar to reports by previous studies and suggest poor prognosis. Surgical specimen axillary lymph node metastases were noted in 25% of specimens, as in previous reports. The reason for reduced axillary node metastasis in spite of poor prognosis of metaplastic carcinoma is that metaplastic carcinomas tend spread hematogenously, rather than through the lymphatic system, to lung or bone (2, 7, 8, 9). During follow-up, local or distant metastases were seen in more than 50% of cases (2, 7, 8, 9). Therefore, systemic evaluation in addition to local recurrence evaluation is needed for follow-up studies.
Aspiration cytology and core needle biopsy might be possible for the preoperative diagnosis of metaplastic carcinoma, but in the presence of hemorrhage or necrosis the possibility of inadequate sampling is high (1, 3, 16, 24). In most cases, transition foci between invasive ductal carcinoma and metaplastic element were noted after excision biopsy (1). Therefore extensive sampling such as excision biopsy should be performed in order to avoid misleading from small sample.
In conclusion, metaplastic carcinomas might display more benign features and less axillary lymph node metastasis than IDC. However, the prognosis is poor, and tumors spread hematogenously. Even though metaplastic carcinomas look like benign masses on mammography and ultrasonography, high signal intensity on T2 MRI images and hormone receptor negativity would be helpful in differentiating this tumor from other breast cancers. Therefore, multimodality image studies including immunohistochemical studies are necessary in the diagnosis of metaplastic carcinoma. In addition, active systemic evaluation for hematogenous metastasis is necessary during the follow-up period.