
Abstract
Background
Recently developed digital tomosynthesis has shown improved detection of pulmonary lesions with a radiation dose comparable to conventional CR but with a much lower radiation dose than CT.
Purpose
To compare the diagnostic performance of digital tomosynthesis (DT) with that of chest radiography (CR) for the detection of aortic arch calcification (AAC).
Material and Methods
The study included 100 patients who underwent multidetector computed tomography (MDCT), DT, and CR (DT and CR were obtained within one week of CT examination). We evaluated and compared the diagnostic performances of DT and CR for the detection of AAC with MDCT as the reference standard. The extent (four grades 0–3) of AAC on DT and CR was also compared with CT calcium score. Inter-observer agreement was analyzed by using kappa statistics.
Results
On DT, overall accuracy for AAC was superior to that of CR (94% and 71%, respectively, P < 0.01). Inter-observer agreement was good with DT and CR (kappa values = 0.74 and 0.62, respectively) for the presence of AAC, and good with DT and moderate with CR (kappa value = 0.64 and 0.53, respectively) for AAC grading. The overall correlation coefficient on AAC grading between DT and CT (calcium score) was superior to that between CR and CT (0.90 and 0.60, respectively).
Conclusion
DT is superior to CR for detection and extent evaluation of AAC.
Arterial calcification is a kind of complication of advanced atherosclerosis. In particular, the arterial calcification results in progressed arterial stiffness and becomes an obstacle for the management of hemodynamics in the elderly (1, 2).
Several examinations have been employed for the detection and quantification evaluation of arterial calcification in routine clinical work. Lately, radiographically visible aortic arch calcification (AAC) and its grades has been suggested as a strong independent predictor for the presence of cardiovascular morbidity (3, 4). Nevertheless, radiographic assessment using AAC grading system has been relatively crude and reproducibility has been questionable. The advantages of electron beam computer tomography (EBCT) and multidetector computed tomography (MDCT) for the evaluation of aortic calcification have been demonstrated with their capability to quantify AAC severity and with their precision to assess AAC distribution (5–7). However, these high-technical examinations are expensive and are not suitable for repeated assessments in clinical practice due to high radiation doses.
Recently developed digital tomosynthesis (DT) refers to the principle of collecting low-dose projection radiography at different angles and using these projections to reconstruct sectional images for the improved detection of subtle lesions with a radiation dose comparable to conventional CR but with a much lower radiation dose than CT (8–10). Thus, the purpose of this study was to evaluate the diagnostic performance of DT and CR for the detection and extent evaluation of AAC in asymptomatic outpatients as compared with that of MDCT.
Material and Methods
Patients
Our institutional review board approved this study, and we got informed consent from all patients. From March to June in 2009, 100 patients who underwent MDCT, DT, and CR were enrolled for this study. These were asymptomatic outpatients who underwent the studies for the evaluation of pulmonary metastasis after colon cancer surgery. Fifty (mean age ± standard deviation 65 ± 8 years; range 46–79 years) subjects (32 men [65 ± 8 years] and 18 women [65 ± 9 years]) had AAC and the remaining 50 (mean age ± standard deviation, 57 ± 8 years; range 46–74 years) matching controls (33 men [57 ± 8 years] and 17 women [57 ± 6 years]) did not have any AAC on chest CT. Baseline characteristics of the population are shown in Table 1. All patients underwent DT and CR within one week from the CT examination; 92 patients underwent DT and chest CT examinations on the same day, and eight patients underwent DT within one week from the time of the CT examination.
Demographics and baseline characteristics of 100 enrolled subjects
*Mean values with standard deviations; numbers in parentheses are ranges
†Positive dyslipidemia with low density lipoprotein-cholesterol level of >140 mg/dL, high density lipoprotein-cholesterol level of <40 mg/dL, triglyceride of >150 mg/dL or use of lipid-lowering drugs
‡Two-group chi-squared test (two-sided)
§Two-sample t- test
Radiography
Chest radiographic examinations (Definium 8000; GE Healthcare, Chalfont St Giles, UK) were acquired using a CsI/a-Si flat-panel-detector, direct-digital radiography system, and included a posteroanterior view with an imaging parameter of tube voltage of 120 kVp and automatic exposure control (AEC) at a speed equivalent of 400. The effective dose of the imaging system was 0.02 mSv for a standard patient. The dose was determined by the use of an anthropomorphic chest phantom (Alderson Lung/Chest Phantom RS-320; Radiology Support Devices, Long Beach, CA, USA) and Monte Carlo-based software (PCXMC; V 1.5, STUK, Helsinki, Finland).
Digital tomosynthesis
A commercially available product (Volume RAD; GE Healthcare, Chalfont St Giles, UK), with a commercial CsI/a-Si flat-panel-detector system was used for DT examinations. Sixty low-dose projection images were collected within a period of 10 s at a tube voltage of 100 kVp, 1:5 dose ratio, and 0.3 mm additional Cu filter. Image data from –15° to +15° were collected while the X-ray tube underwent vertical continuous movement from –17.5° to +17.5° around the standard orthogonal posteroanterior position, whereas the detector position was fixed. The obtained 60 projection images were used for the reconstruction of approximately 54 coronal images with a nominal thickness of 4-mm without overlap. We modified the DT parameters and developed a low dose condition for chest scans (11). The entrance incident air kerma for this protocol, including a posteroanterior radiograph as a reference image, was 0.3 mGy. The effective dose was calculated using PCXMC to estimate the absorbed and effective dose for each projection view. The effects of changes in source-to-image distance, collimation, and changes in the exposure of organs to the primary beam over the range of acquisition angles were included in the simulation (12). For a cumulative incident air kerma of 0.2 mGy for 60 projections of the digital tomosynthesis scan, the effective dose was determined to be 0.041 mSv for a standard patient following the ICRP 103 tissue weighting factors.
Multidetector CT imaging
In all patients, MDCT scans were obtained throughout the thorax at end inspiration, and by the use of 64-slice equipment (LightSpeed VCT; GE Healthcare, Milwaukee, WI, USA). Main chest CT scanning parameters were as follows: individual detector width, 0.625 mm; gantry rotation time, 400 msec; tube voltage, 120 kVp; tube current, 110–150 mAs; pitch of 0.97. Contrast material was not administered for CT examinations. Axial images were reconstructed with the following parameters: 2.5-mm-section thickness, high-spatial-frequency reconstruction algorithm (bone preset), and 34–38-cm field of view. Synthetic coronal planar images were reformatted with a 4-mm interval and fully covered the area from the anterior skin to the back of the chest. The effective dose for chest CT was 3.4 mSv, based on a standard patient model using the anthropomorphic phantom and a conversion factor from a dose-length product (E DLP) to an effective dose (ED) of 0.017 mSv/(mGy.cm) (13).
Image analysis
Two radiologists evaluated independently the presence and extent of AAC on DT and radiographic images without the knowledge of CT finding results. The extent of AAC was divided into four grades (3–3) in consideration of a previous categorization system of the ACC (3). It is visualized in Fig. 1. Briefly, the scoring system was as follows: (a) grade 0, no visible calcification; (b) grade 1, small spots or a single thin area of calcification; (c) grade 2, one or more areas of thick calcification; and (d) grade 3, circumferential calcification. In the terms of detection of AAC, score 0 was considered as ‘negative’ for AAC and scores 1, 2, and 3 were considered as ‘positive’ for ACC. In order to have blinded analysis results, imaging studies were divided into two groups (1st to 50th and 51st to 100th). Radiographs of the former group and DT of the latter group were regrouped into the same group and then reordered randomly; and vice versa for the remaining imaging studies. Randomization was achieved by using a standard random number generator for the determination of a random reading order. Observers were allowed to change window width and window level and to use function keys for pan and zoom. The interval between the two sessions was two weeks. Owing to large differences in appearance between on DT and on radiographs, this procedure was considered sufficient for the avoidance of recall bias.
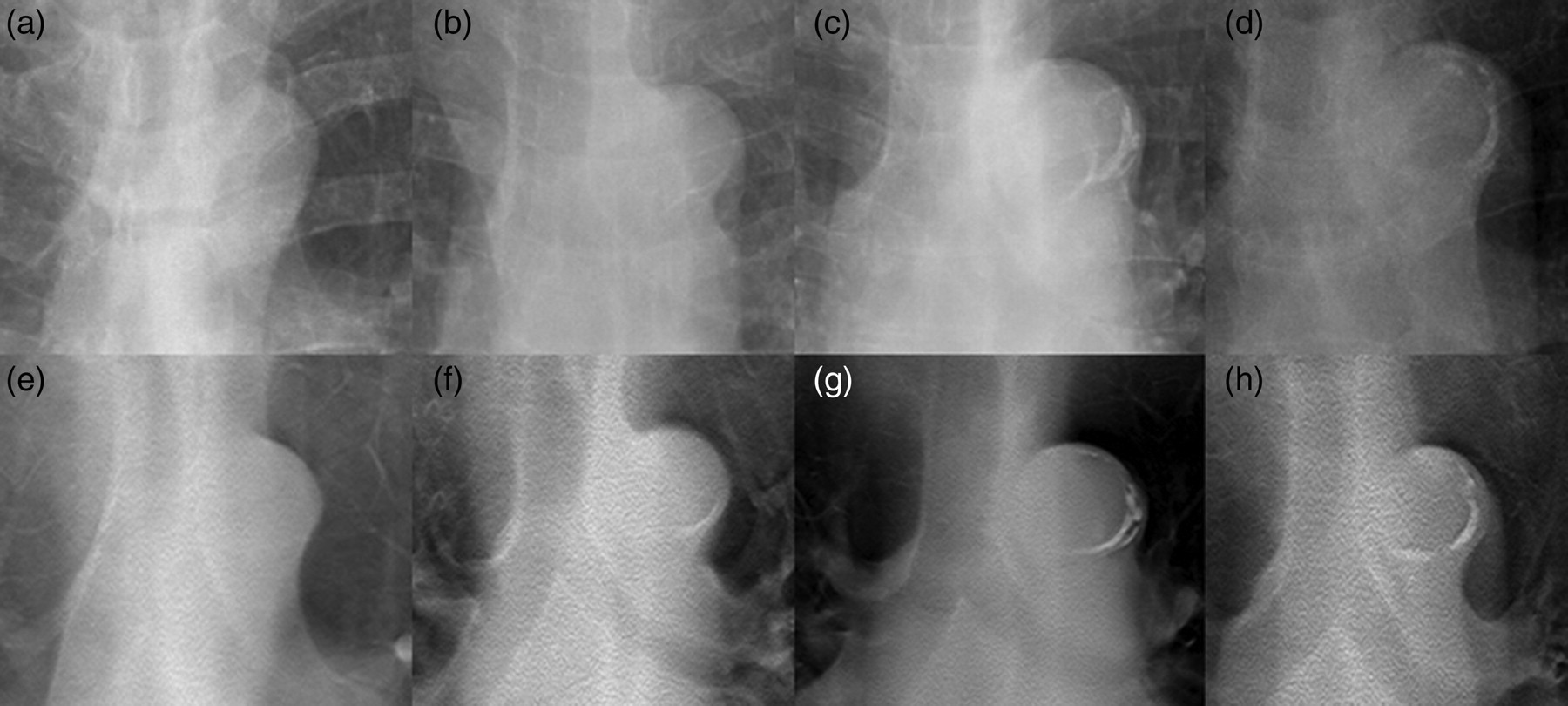
Image in 72-year-old man. Aortic arch calcification grades are shown on chest radiography (a–d) and digital tomosynthesis (e–h). Aortic arch calcification extent was divided into four grades (0–3): (a and e) grade 0, no visible calcification; (b and f) grade 1, small spots or a single thin area of calcification; (c and g) grade 2, one or more areas of thick calcification; (d and h) grade 3, circumferential calcification
Reference standard
MDCT served as reference standard method for the analysis. We evaluated thoroughly the aortic arch calcification on both transverse and coronal reformatted images of CT in order to minimize the anatomic discordance between transverse plane of CT and coronal planes of other modalities (CR, DT).
Based on MDCT images, we got the quantification of the calcium in the aortic arch by the use of a calcium scoring program (Terarecon 3.4.2.11, San Mateo, CA, USA).
Statistical analysis
Using a standard definition, diagnostic performances including sensitivity, specificity, and accuracy for the presence of AAC on DT and CR were calculated and compared with those on CT (CT served as a reference standard) (14). In addition, performance values of DT and CR were calculated and compared using the McNemar test. Inter-observer agreements for the extent of AAC between the two observers were analyzed by using Cohen's kappa statistics (15). Finally, the extents of AAC on DT and CR, respectively, were correlated with that of CT (CT calcium score) by employing the Spearman's correlation coefficient rank test. Statistical significance was calculated at the 95% confidence interval (P < 0.05). A commercially available software program was used for the performance of data processing and analysis (PASW, version 17.0; SPSS, Chicago, IL, USA).
Results
Diagnostic performance of DT and CR for the detection of AAC
Table 2 gives an overview of the calculated sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of DT and CR for the detection of AAC. Overall sensitivity of DT was superior to that of CR (94% and 47%, respectively, P < 0.01) (Fig. 2). On DT, overall accuracy for the detection of AAC was 94% (97% for observer 1 and 90% for observer 2), which was superior to that of CR (overall accuracy, 71%; 71% for observer 1, and 70% for observer 2) (all Ps < 0.05). False-negative observations on CR (28 and 25 cases for two observers, respectively) for the detection of AAC were significantly more frequent than those on DT (2 and 4 cases for the observers, respectively) (all Ps < 0.01). False-positive interpretations were one and five cases for the observers, respectively, on CR and they were one and six cases for the observers, respectively, on DT.
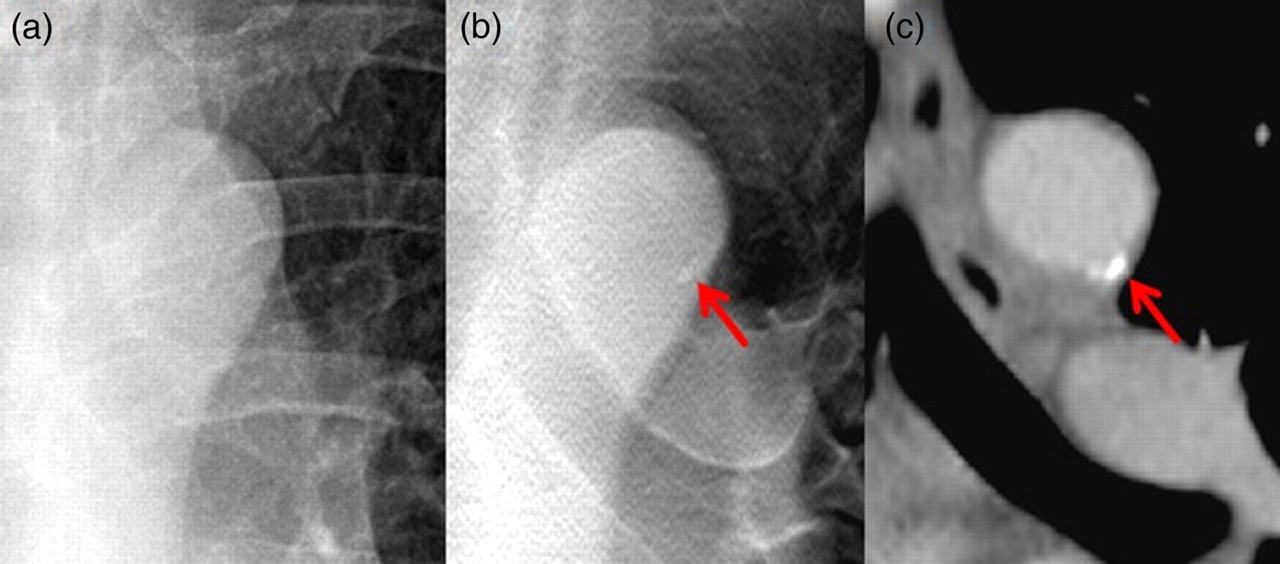
Image in 67-year-old woman. Chest radiography (a) shows no calcification in the aortic arch (grade 0). Digital tomosynthesis (b) shows focal calcifications in the aortic arch (grade 1). Chest CT (c) confirms same extent of calcification in the aortic arch (CT calcium score: 1076)
Diagnostic performance of DT versus CR for detecting aortic arch calcification
Numbers in parenthesis are percentages
DT = digital tomosynthesis, CR = chest radiography, PPV = positive predictive value, NPV = negative predictive value
Inter-observer agreement of DT and CR
Inter-observer agreement was good for DT (kappa value = 0.74) and CR (kappa value = 0.62) for detecting AAC. For the evaluation of AAC extent, DT showed good (kappa value = 0.64) agreement and CR demonstrated moderate (kappa value = 0.53) agreement between the two observers.
Comparison of AAC grade categorization among DT, CR, and CT quantification of AAC
The mean CT calcium score was 559.5 (median = 219.3, range = 7–3940) for a total of 50 patients who had AAC. According to the AAC grade categorization on CR, median (± standard deviation) CT calcium score of AAC was as follows; 0 (±214.7) for grade 0 (n = 77), 228 (±445) for grade 1 (n = 15), 1784 (±1402) for grade 2 (n = 7), and 1550 for grade 3 (n = 1) by observer 1, and 0 (±208) for grade 0 (n = 70), 219.5 (±616.5) for grade 1 (n = 24), 1378 (±1590) for grade 2 (n = 4), and 2537.5 (±1396.5) for grade 3 (n = 2) by observer 2. According to the AAC grade categorization on DT, median (± standard deviation) CT calcium score of AAC was as follows; 0 (±10) for grade 0 (n = 51), 121.5 (±214.8) for grade 1 (n = 32), 628 (±561) for grade 2 (n = 13), and 3047 (±1065) for grade 3 (n = 4) by observer 1, and 0 (±17.4) for grade 0 (n = 48), 72 (±166.1) for grade 1 (n = 31), 494 (±580) for grade 2 (n = 16), and 2569 (±1414) for grade 3 (n = 5) by observer 2. The overall correlation coefficient score between the grades of AAC on DT and CT (CT calcium score) was 0.90 (observer 1, R = 0.98, P < 0.01; observer 2, R = 0.86, P < 0.01), which was superior to that between the grade of calcification on CR and CT (CT calcium score) (overall correlation coefficient score, 0.60; 0.62 for observer 1, and 0.58 for observer 2, all P < 0.01) (Fig. 3).
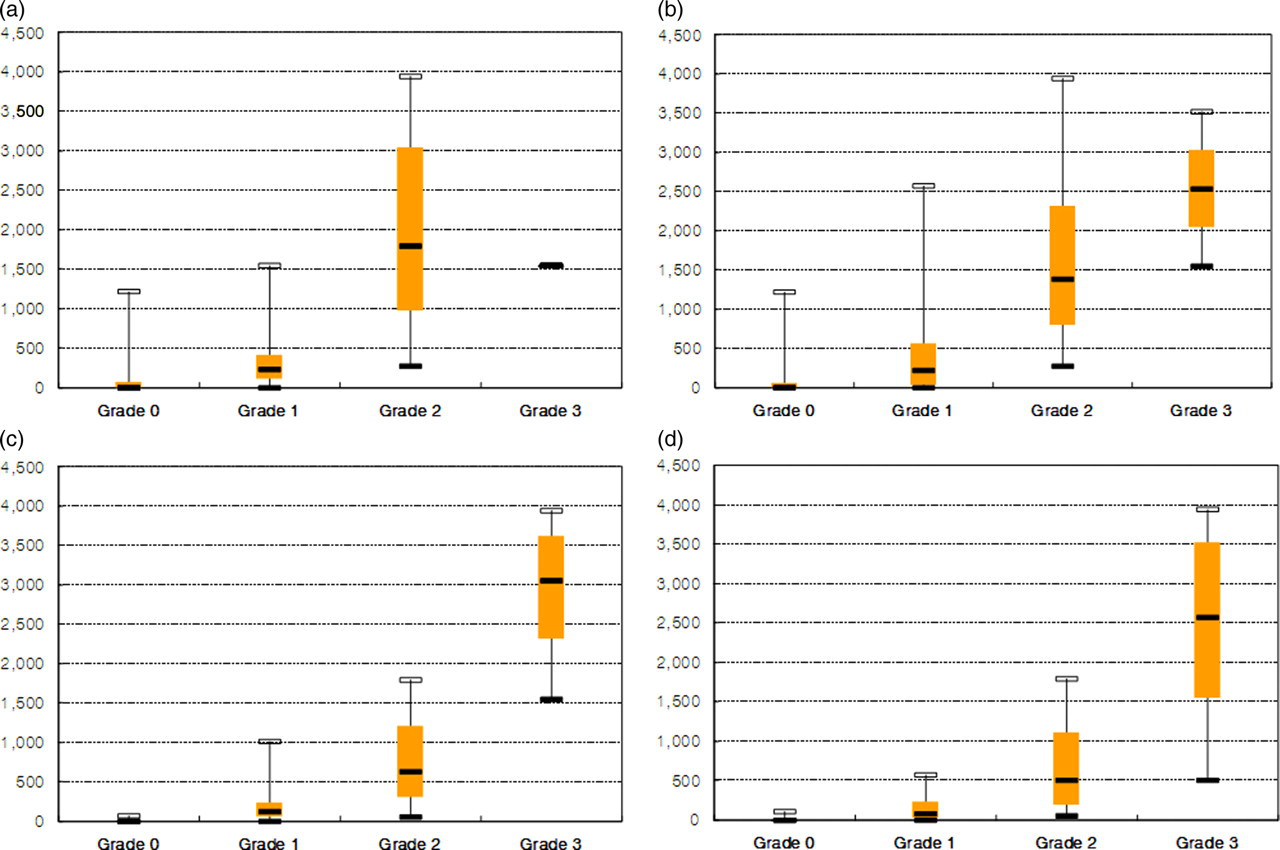
Graph shows correlation between the grades of aortic arch calcification on radiography and calcium score determined by CT for observer 1 (a) and for observer 2 (b). Graph shows correlation between the grades of aortic arch calcification on tomosynthesis and calcium score determined by CT for observer 1 (c) and for observer 2 (d)
Discussion
Given that calcium within the aorta is related to the systemic process of atherosclerosis, it is not surprising that its presence is associated with traditional coronary risk factors (16, 17). Aortic calcification has been associated with coronary artery disease and stroke in the general population, and the presence of aortic calcification is associated with a 3–4-fold higher risk for mortality and cardiovascular event (18, 19). To put it the other way around, age, hypertension, cigarette smoking, low density lipoprotein-cholesterol and high density lipoprotein-cholesterol levels, systolic blood pressure, and glucose levels are all predictors of aortic calcification (16, 17, 20). The presence of aortic calcification is also related to more extensive coronary artery disease and a higher coronary artery calcium score (16, 20, 21). These findings suggest that the evaluation of AAC presence and its extent might provide additional prognostic information to that obtained from coronary calcium scoring alone.
Despite the fact that CT scans provide information that is more precise in terms of the extent and distribution of AAC, high radiation doses imposed on patients can be potentially hazardous. Moreover, the natural history of aortic calcification (its clinical implication and how it evolves over time) has not been adequately studied by CT imaging. The majority of studies on AAC have been conducted by employing CR until now (22, 23). Moreover, AAC grade as determined by CR reflects the magnitude of calcified change in the whole aorta, and its evaluation may provide supportive information for atherosclerotic risk stratification. Moreover, the grade is a strong independent predictor of cardiovascular events beyond traditional risk factors (3, 4).
The recently developed DT technique is an interesting alternative method for the detection of pulmonary nodules and parenchymal lesions in patients with pulmonary mycobacterial disease, because the technique provides a low-radiation dose (compared to chest CT) and improved detectability (compared to CR) (8–10). The reported effective dose of DT is approximately 0.12 mSv, which is approximately 10 times higher than that used for a radiographic examination (0.01–0.02 mSv); however, the dose is approximately 30 times lower than that of a chest CT examination (3–8 mSv) (8, 9). Furthermore, our institution has used ‘low-dose DT (0.04–0.05 mSv)’ technique by altering DT parameters, which amounts to one-half or less of conventional-DT radiation dose (10).
To the best of our knowledge, this is the first report elaborating on the usefulness of DT for the detection and extent evaluation of ACC. In our study, we showed superior sensitivity, negative predictive value, and accuracy for the detection of AAC on DT to those on CR. The superiority of DT may have been rendered with better depth resolution and much less overlap of anatomical features as compared with CR. As for inter-observer agreements, both DT and CR showed good agreements for the detection of AAC, and good and moderate agreements for the evaluation of AAC extent, respectively. These might reflect the reliability of DT and CR for the detection and follow-up progression evaluation of AAC.
There are several limitations to the present study. First, we did not evaluate cardiovascular events for patients. However, the primary objective of this study was to compare the diagnostic performances of DT and CR for the detection of and the extent evaluation of AAC by the use of chest CT as a reference. The study was not designed to evaluate the diagnostic performance of DT for predicting cardiovascular events. A large prospective study using diverse imaging modalities (such as CT and DT) is needed to correlate the detected ACC quantification and long-term clinical follow-up results. Second, our CT quantification methods for AAC might have resulted in under-estimation, because CT was performed as a non-cardiac-gated, routine chest CT for the surveillance of postoperative pulmonary metastasis in patients with a colon cancer. Third, we did not include lateral chest radiographs for image analyses, which might have contributed to enhancing radiographic sensitivity for AAC detection and quantification. However, in our department, we usually recommend posterior-anterior CR only for patients in whom chest CT study is scheduled to evaluate further the CR-detected thoracic lesions.
In conclusion, DT has superior sensitivity, negative predictive value, and accuracy for the detection of ACC to those of CR. It also demonstrates good inter-observer agreement for the detection and extent evaluation of AAC. Moreover, DT shows stronger correlation in terms of AAC extent evaluation with CT calcium score than CR.
Footnotes
Acknowledgements
The author would like to acknowledge John M Sabol (GE Healthcare, Global Diagnostic X-Ray, Mailstop W-702, 3000 North Grandview Boulevard, Waukesha, WI 53188, USA) for technical support.