
Abstract
Background
Severe acute hepatic failure (SAHF), which progresses to fulminant form in some cases, is a life-threatening disease.
Purpose
To assess the technical feasibility and the efficacy of transcatheter arterial steroid injection therapy (TASIT) for SAHF.
Material and Methods
Twenty-seven patients with SAHF, 10 of whom had variant anatomy of the hepatic artery, underwent radiologic placement of an indwelling catheter in the hepatic artery, and TASIT was subsequently performed for three days. The tips of the catheters were inserted as follows: common hepatic artery (n = 18), proper hepatic artery (n = 4), and replaced right hepatic artery (n = 5). The clinical success rate of TASIT and the prognosis after TASIT were evaluated.
Results
In one patient, intimal injury of the left hepatic artery was encountered; however, TASIT could be resumed and completed via intrahepatic arterial collaterals. In two patients, the catheter tip placement was corrected on the following day because of dislocation. Finally, TASIT could be carried out in all patients. Twenty-two patients (81.5%) responded to TASIT but five patients (18.5%) did not. Among the five non-responders, two patients were transferred to liver transplantation and survived, and three patients died. There was no significant difference in the response rates to TASIT among locations of catheter tip (P > 0.05) and extent of drug distribution in the liver (P > 0.05).
Conclusion
TASIT is a feasible and efficient treatment option for SAHF regardless of the anatomic variation of the hepatic artery. Careful manipulation during the procedure to prevent injury of the hepatic artery may be the most essential factor not only for successful TASIT but also for liver transplantation, which may be performed on TASIT non-responders.
Keywords
Severe acute hepatic failure (SAHF) is a disorder in which liver damage rapidly progresses with jaundice, ascites, encephalopathy, and coagulopathy (1, 2). In a few cases of SAHF, the disease is self-limiting. However, in some cases, the disease may progress to the fulminant form of SAHF, which has a high mortality rate (2). Intravenous steroid injection and plasma exchange, the traditional therapies for SAHF, are often ineffective (3–5). Liver transplantation is, therefore, the only effective treatment for patients with the fulminant form of SAHF (6). It is difficult to predict the disease progression from the non-fulminant form to the fulminant form of SAHF. In addition, there are few effective treatments that can prevent the progression of SAHF to the fulminant form.
In our institution, transcatheter arterial steroid injection therapy (TASIT) has been performed in patients with fulminant and non-fulminant forms of SAHF for 3 years. TASIT is a novel method that efficiently suppresses the increased intrahepatic macrophage activity in damaged livers. In this procedure, an indwelling catheter is percutaneously placed in the hepatic artery using an interventional technique so that 3-day intra-arterial steroid injection therapy can be administered. Better prognoses have been reported in patients who underwent TASIT than in patients who did not (7). The purpose of this study was to assess the technical feasibility and efficacy of hepatic artery catheter placement for TASIT.
Material and Methods
Patients
Between January 2005 and December 2006, 27 patients (19 men and 8 women; age range 18–78 years; mean 45 years) underwent indwelling catheter placement in the hepatic artery and TASIT. Cause disorders were viral hepatitis type A (n = 4), viral hepatitis type B (n = 7), drug-induced hepatitis (n = 2), Wilson disease (n = 2), and unknown origin (n = 12). Laboratory data were as follows: AST 542–16346 IU/L (mean 5212 IU/L); ALT 585–9615 IU/L (mean 3888 IU/L); prothrombin time (PT) 10–69%. Eleven of 27 patients with severe acute hepatic failure (SAHF) were diagnosed with the fulminant form, having hepatic coma of grade II and higher, and a PT value less than 40%.
SAHF patients who seemed at high risk of progression to the fulminant form and patients with fulminant hepatitis were considered candidates for TASIT. Severe liver atrophy on computed tomography and/or the passage of too much time from the onset of the disease were considered contraindications for TASIT.
Our hospital's ethics committee approved this protocol, and written informed consent was obtained from all patients.
Procedure and therapy protocol
Under local anesthesia at the right inguinal region, a 3-F (n = 2), 4-F (n = 24), or 5-F (n = 1) sheath (Super sheath, Medikit, Tokyo, Japan) was transfemorally inserted using Seldinger's method. Arteriograms of the celiac and superior mesenteric artery (SMA) were performed using a 3-F, 4-F, or 5-F catheter (FASUS catheter (8), Medikit, Tokyo, Japan) to identify the anatomy of the hepatic artery.
When the hepatic artery showed a normal anatomy, the catheter tip was placed in the common hepatic artery (CHA) or proper hepatic artery (PHA) where the catheter could be stabilized. When the hepatic arteries showed anatomical variation, we placed the catheter at the proper portion with reference to the CT liver volume and angiographic hemodynamics so that the drug could be distributed over the widest possible area of the liver parenchyma. For example, in a patient with a replaced right hepatic artery (RHA), drug distribution to the whole liver via one route using one catheter was impossible; thus, the catheter was placed at that part of the hepatic artery where the drug could be distributed through as much of the liver as possible.
In many cases (21 of 27 patients), hepatic artery catheter placement was undertaken using a catheter (FASUS catheter: 3-, 4-, or 5F) normally used in diagnostic angiography because the placement was short-term. In patients for whom hepatic artery catheter placement using a FASUS catheter was difficult because of curvature, stenosis, or extensive spasm of the hepatic artery, the coaxial method (n = 2) using a 2.5-F microcatheter (Sniper Cobra, Clinical Supply, Tokyo, Japan) was used. We used catheters with anti-thrombogenic coating in all patients.
After hepatic artery catheter placement, one gram of methylprednisolone per day was infused for 2 hours via the indwelling catheter using the syringe pump at the bedside. A total of 3 g of methylprednisolone was infused over 3 days (7). In the periods when transcatheter drug infusion was not being performed, the catheter system was filled with 3000 IU of heparin to prevent catheter obstruction. Sedatives were used on a case-by-case basis. During TASIT, most patients concurrently underwent plasmaphoresis.
After the scheduled regimen of TASIT for 3 days, was finished, the catheter–sheath system was removed, and we pressed the inguinal region manually. Complications such as puncture site bleeding or subcutaneous hematoma were periodically checked after catheter removal. Then, the patient was started on 30–40 mg oral steroid per day. The amount of the oral steroid was tapered down to a small amount while the hepatic function was monitored.
Assessment
On the basis of angiographic findings, follow-up CT findings, intraoperative findings and outcomes of the patients, the clinical success rate of TASIT, complications related to the procedures of catheter placement, and response rates to TASIT were evaluated.
We defined the effective treatment group as patients who were alive and in remission after TASIT. We defined the ineffective treatment group as patients who died or got worse and underwent liver transplantation after TASIT. Degrees of SAHF, locations of catheter tip, and patterns of drug distribution to the liver were compared between the two groups. The Kruskal-Wallis coefficient and Mann-Whitney U-test were used for the statistical analysis. A P value less than 0.05 was judged statistically significant.
Results
Anatomy of the hepatic artery and locations of the catheter tip
According to the angiographic findings of the celiac artery and SMA, the anatomy of the hepatic artery was classified as normal (n = 17), replaced RHA (n = 5), replaced LHA (n = 5), accessory RHA (n = 1), and hepatomesenteric trunk (n = 1). Locations of the tip of the indwelling catheter were as follows: CHA (n = 18), PHA (n = 4), and replaced RHA (n = 5).
In the 18 patients who had a normal anatomy or a hepatomesenteric trunk, the catheter was placed in the CHA or PHA, and the drug was distributed to the whole liver.
In the five patients who had a replaced RHA, two of whom concurrently had a replaced LHA, the catheter was placed in the replaced RHA, and the drug was distributed only in the right lobe of the liver. In the three patients who had a replaced LHA only, the catheter was placed in the CHA or PHA, and the drug was distributed only in the right lobe of the liver. In one patient who had an accessory RHA, the catheter was placed in the CHA, and the drug was distributed into both the left lobe and right anterior segment of the liver.
Clinical success rate of TASIT
In all 27 patients, TASIT was immediately started following the hepatic artery catheter placement procedure. TASIT was successfully carried out in all but one patient, who died of hepatic failure on the day after it began; the clinical success rate of TASIT in the remaining 26 was therefore 100%.
Complications related to the procedures
Specific complications were recognized in four of 27 patients during and after the catheter placement procedure.
As a complication during the catheter placement procedure, intimal injury to the LHA occurred in one case, possibly due to guide-wire manipulation. In this case, a hepatic arteriogram performed after the injury showed occlusion of the proximal portion of the LHA; however, arterial branches A2 and A3 were visualized via the intrahepatic anastomosis from the middle hepatic artery (MHA). Drug distribution in the whole liver was obtained from the indwelling catheter placed in the CHA, and TASIT was successfully resumed (Fig. 1).
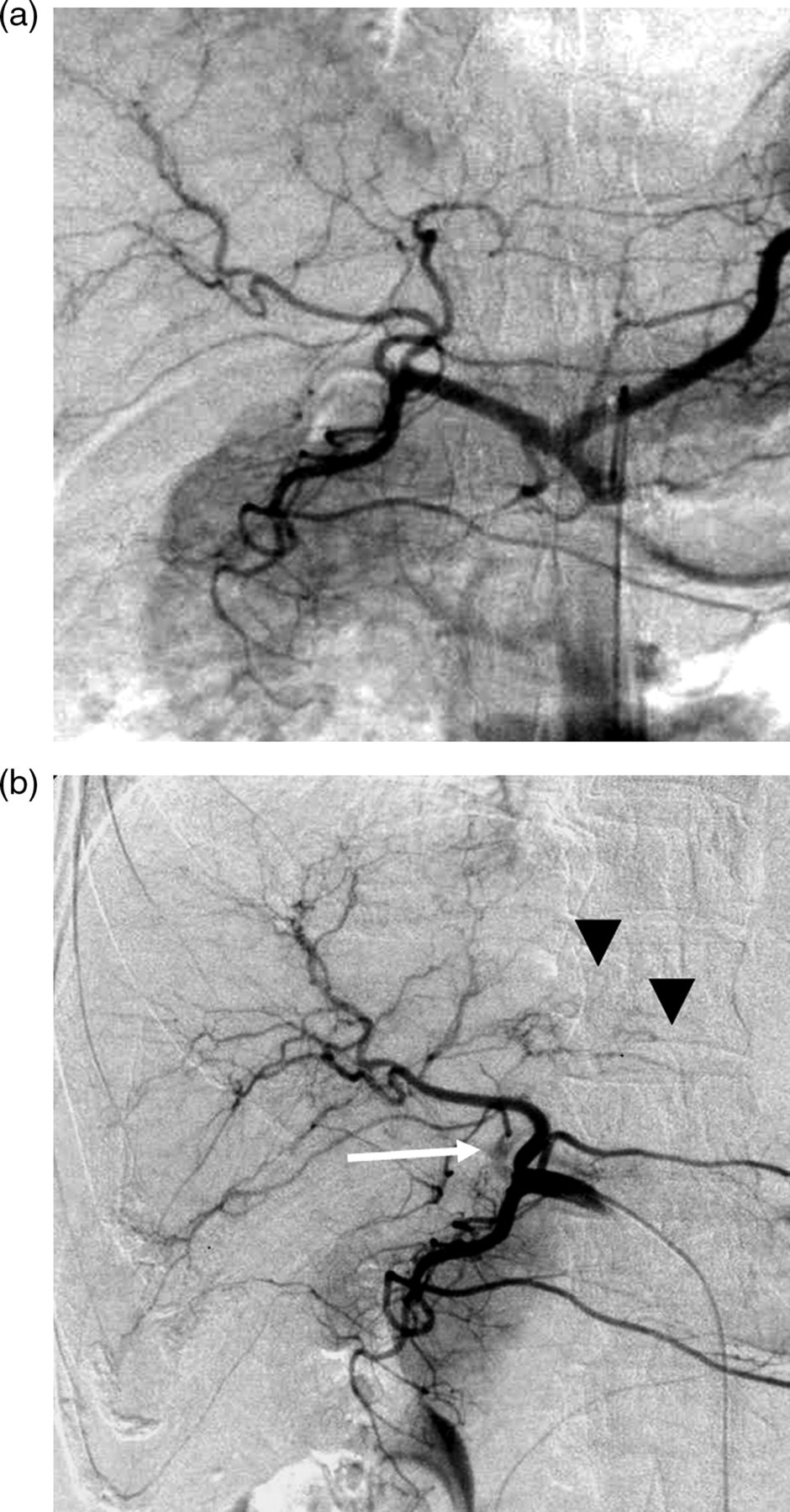
A 47-year-old woman with non-fulminant SAHF of unknown etiology. (a) Celiac arteriogram using a 4-F FASUS catheter shows normal anatomy of the hepatic artery; (b) Intimal injury of the left hepatic artery at the proximal portion occurred during the guide-wire manipulation. Angiogram using a 3-F FASUS catheter whose tip was placed in the common hepatic artery shows occlusion of the left hepatic artery (white arrows). However, the peripheral branches of the left hepatic artery (A2 and A3: arrowheads) were visualized via the anastomotic branches originating from MHA, and drug distribution throughout the whole liver was obtained
As complications after the catheter placement procedure, occlusion of the hepatic artery occurred in one case (Fig. 2) and catheter dislocation in two. In the case with occlusion, the microcatheter was coaxially inserted in the replaced RHA arising from the SMA; then complete occlusion of the replaced RHA near the catheter tip was demonstrated by the angiogram through the indwelling catheter on the next day. Fortunately, a celiac arteriogram showed the right hepatic arterial branches via the intrahepatic anastomosis from the CHA. Therefore, another 4-F FASUS catheter was placed in the CHA, and TASIT was successfully resumed. In one of the two patients with catheter dislocation, a microcatheter coaxially inserted in the replaced RHA was dislocated into the SMA on the next day, and replacement of the microcatheter was performed. In the other case with catheter dislocation, a 4-F FASUS catheter inserted in the CHA was dislocated into the abdominal aorta on the next day. A new 4-F FASUS catheter was placed with its tip at the PHA. No bleeding at the puncture site, inguinal hematoma, skin infection, sepsis due to the catheter, or infection was observed.
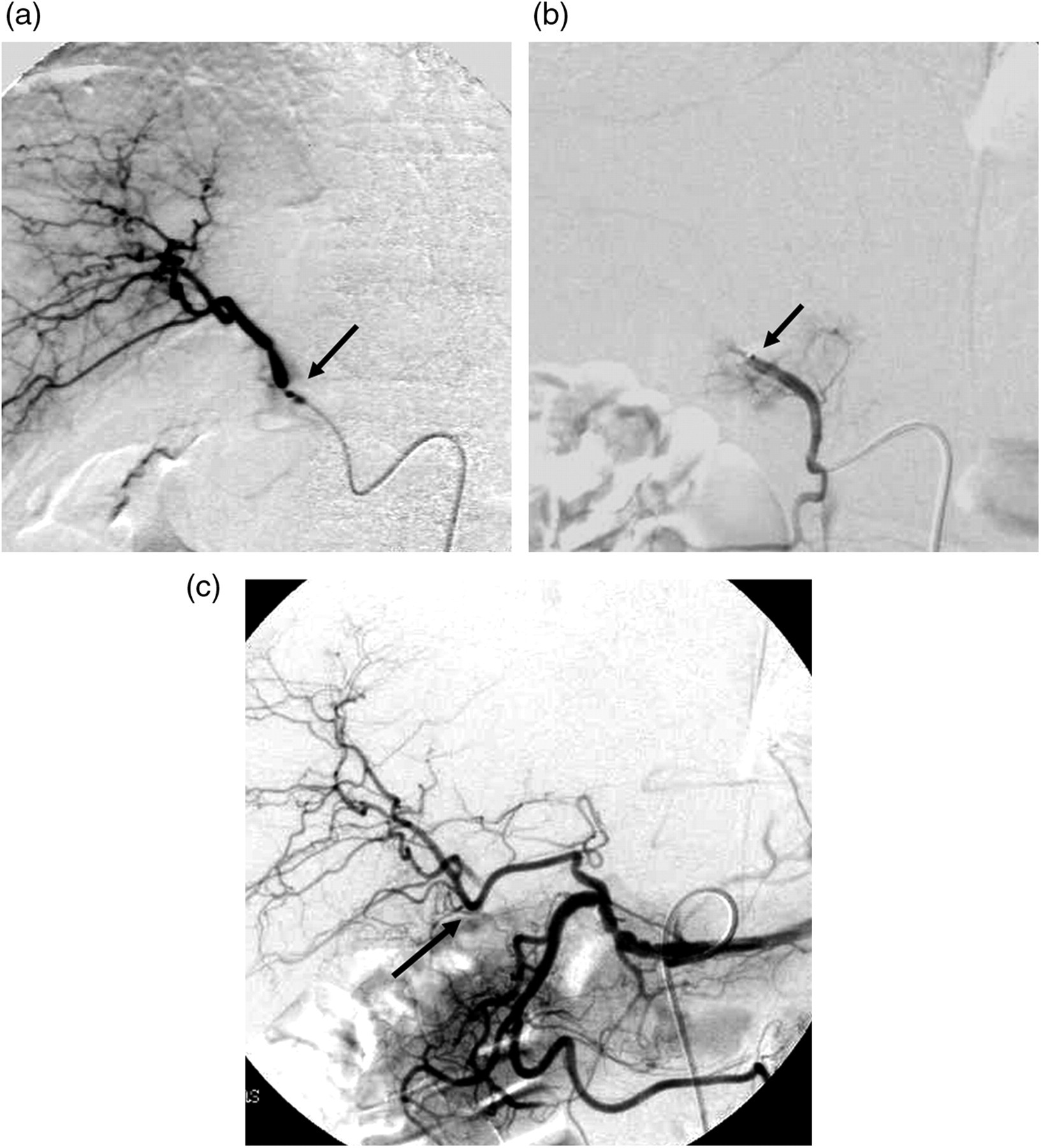
A 31-year-old woman with non-fulminant SAHF of unknown etiology. A 2.5-F microcatheter was coaxially placed in the replaced right hepatic artery arising from the superior mesenteric artery (arrow). (a) Hepatic arteriogram through the indwelling microcatheter immediately after the placement procedure shows drug distribution in the right lobe of the liver and focal stenosis of the replaced right hepatic artery due to the angiospasm. Since adequate blood distribution in the right lobe of the liver was observed, no spasmolytic drugs were used; (b) Angiogram through the indwelling microcatheter on the next day of (a) shows complete occlusion of the main trunk of the replaced right hepatic artery (arrow); (c) Celiac arteriogram following (b) shows drug distribution in the right lobe of liver via the intrahepatic anastomosis (arrows). A new 4-F FASUS catheter was placed in the common hepatic artery, and TASIT was resumed
Response rate to TASIT
Among the 27 patients, the effective group included 22 patients (81.5%) and the ineffective group included five patients (18.5%); the latter group consisted of two patients who were transferred to liver transplantation and three patients who died of hepatic failure (Table 1). All five patients in the ineffective group were initially diagnosed with fulminant form SAHF. By contrast, all 16 patients initially diagnosed with non-fulminant form SAHF responded well to TASIT and were discharged: none of them deteriorated to fulminant hepatitis after induction of TASIT (Table 2).
Therapeutic effect of TASIT
Numbers in parentheses indicate percentages of patients
Relationship between the type of SAHF and rate of response to TASIT
Response rates according to location of catheter tip were as follows: CHA, 82.4% (14 of 17 patients); PHA, 100% (4 of 4 patients); and replaced RHA, 100% (4 of 4 patients). No statistically significant difference was shown in the response rates among the three locations (Kruskal-Wallis test, P > 0.05) (Table 3).
Relationship between location of catheter tip and rate of response to TASIT
*P values were calculated by Kruskal-Wallis coefficient
†One patient was excluded in whom the indwelling catheter was replaced in the CHA after occlusion of the replaced RHA
‡One patient was excluded in whom the indwelling catheter was replaced in the PHA because of catheter dislocation
Next, the patients were divided into two groups according to drug distribution: namely, partial liver and whole liver. Of the 18 patients with whole-liver drug distribution, 14 patients (77.8%) responded to TASIT. Of the eight patients with partial-liver drug distribution due to anatomical variations such as replaced RHA, replaced LHA, and accessory RHA, seven patients (87.5%) responded to TASIT. There was no statistically significant difference in the response rates between the two drug-distribution groups (Mann-Whitney U-test, P > 0.05) (Table 4).
Relationship between pattern of drug distribution in the liver and rate of response to TASIT
*P values were calculated using Mann-Whitney U coefficient
†One patient was excluded in whom the indwelling catheter was replaced in the CHA because of occlusion of replaced RHA
Discussion
Transcatheter arterial infusion therapy, which allows concentrated drugs to be distributed throughout a target organ, is expected to improve therapeutic effects while reducing adverse reactions of other organs to the drug (9, 10). In recent years, transcatheter arterial infusion therapy has been performed for various diseases such as severe pancreatitis using protease inhibitor and antibiotics (11), inflammatory bowel disease using steroids (12), and malignant tumors of the liver (13–17), urinary bladder (18), uterus (19), and head and neck (20) using anticancer drugs. TASIT is a novel method, designed for treating SAHF by Koto et al., based on the finding that intrahepatic macrophage activity in patients with SAHF is suppressed by corticosteroids (21, 22). To our knowledge, there are few case reports other than the initial report (7) (23).
SAHF is usually a disease state with emergency and fatality. For patients with SAHF, immediate induction and initiation of the treatment is required because of its rapid progression. Since this treatment is often performed as an unscheduled emergency procedure, prompt and authentic catheter placement is necessary. Therefore, the catheter placement procedure should be simple as possible. Celiac and hepatic arteriograms were obtained using an antithrombogenic catheter ranging from 3-F to 5-F, and the catheter was placed just within the hepatic artery, in most cases without fixation (24). Some preshaped catheters have been used in cases with anatomically unstable locations for catheter placement or in cases in which catheter placement is technically difficult for other reasons. We did not use blood flow redistribution (25) or catheter placement in the gastroduodenal artery or right gastroepiploic artery with the tip fixed using metallic coils (fixed catheter-tip method (26–28)) or a W-Spiral catheter with shape-memory alloy (gastroepiploic method (29)), although these techniques are often used for continuous hepatic artery infusion of anticancer drugs for the treatment of advanced hepatocellular carcinoma and metastatic liver tumor.
Koto et al. reported that there was a significant difference in patient outcomes between their TASIT (n = 17) and non-TASIT groups (n = 17) (7), suggesting that TASIT is an effective therapy for SAHF. The response rate of TASIT in our series exceeded 80%, and patients also showed good treatment outcomes (Table 1). Some previous reports have described the outcomes of patients with acute hepatic failure: the rates of overall survival referring to liver transplantation and mortality were 29–43%, 34–48%, and 25–67%, respectively (30–32). All these values show worse results compared with that in our study.
The response rate in the non-fulminant group was 100%, much higher than that in the fulminant group (54.5%) (Table 2). Therefore, it was suggested that early induction of TASIT, before the liver deteriorates to the fulminant stage, should be a high priority. Koto et al. suggested that indication for TASIT was determined by classifying the degree of macrophage activity in SAHF (23). Further study will reveal the most appropriate indication for TASIT including liver transplantation.
Hepatic artery catheter placement and TASIT were technically successful in all the patients although 10 of 27 patients (37.0%) had anatomic variations of the hepatic artery. TASIT following the hepatic artery catheter placement was successfully accomplished in all cases except one in which the patient died on the second day due to progression of liver failure.
In addition, there was no significant difference in the response rates of TASIT between the PHA group (the catheter is placed in the PHA and the infused drug is distributed to the whole liver) and the CHA group (the catheter is placed in the CHA and the infused drug is distributed not only to the liver but also to the stomach, duodenum, and pancreas) (Table 3). From these results, hepatic artery catheter placement and subsequent TASIT can be applied to all patients with SAHF regardless of the anatomical variations of the hepatic arteries. Placement of the catheter at the CHA or PHA did not influence the therapeutic effect of TASIT. The catheter should be placed in whichever position it will be most stable, based on the vascular anatomy.
The patients were also divided into a whole-liver distribution group (infused drug is distributed to the whole liver) and a partial-liver distribution group (infused drug is distributed only to part of the liver), the latter due to the presence of anatomical variations of the hepatic artery. There was no significant difference in the response rates of TASIT between the whole-liver and the partial-liver groups (Table 4).
In summary, even in the cases in which the infused drug could not be distributed to the whole liver, we could place a catheter in the vessel where the drug could be distributed over the greatest possible area of the liver. It appeared that selective catheter placement in order to let the drug distribute only to the liver or to the whole liver is unnecessary; further, a selective insertion that violates arterial anatomy and the arterial caliber may cause arterial injury.
Most of the published reports on complications related to continuous transarterial infusion therapy have pertained to infusion chemotherapy of anticancer drugs using a port catheter system for hepatocellular carcinoma and metastatic liver carcinoma (24, 29, 33, 34). From these reports on port catheter systems, complications during and after the placement procedure are as follows: vascular injury during the procedure, 0–1%; dislocation of the catheter tip, 3–10%; hepatic artery occlusion, 3–13%; and catheter obstruction, 5–11%.
Hepatic artery occlusion during and after the catheter placement was recognized in two cases (7.4%) in our study. In both cases, fortunately, TASIT was successfully resumed via the intrahepatic anastomotic vessels after replacement of the indwelling catheter or correction of the location of the catheter tip. In one of the two cases, severe angiospasm occurred during the catheter placement procedure, and the hepatic artery was completely occluded on the next day even though a microcatheter was carefully inserted in the hepatic artery. Extensive angiospasm has been reported in patients with severe pancreatitis (35). In our series of SAHF, some cases were complicated with angiospasm of the hepatic arteries, and more careful catheter manipulation was required in these cases. In patients with SAHF, preservation of the hepatic artery was very important; paying better attention to hepatic artery injury or occlusion is necessary, not only for undergoing efficient TASIT, but also for considering liver transplantation, which might be applied in non-responders.
In this study, catheter dislocation after catheter placement was recognized in two cases (7.4%). The indwelling catheters were dislodged on the day after the catheter placement in both cases. The dislocation rate in our study was relatively high compared with that in the port catheter system (24, 29, 33, 34); the cause was considered to be the technique of catheter placement, with our emphasis on simple and convenient means. Blood flow redistribution using metallic coils was not performed in this study; thus, the infused drug might have been partially distributed to the stomach, duodenum, and pancreas. However, no adverse drug reaction was seen.
There was no catheter occlusion in this study while a certain degree of catheter occlusion has been reported in placement of the port-catheter system (24, 29, 33, 34). We were able to easily perform short-term placement and treatment for three or four days (which differs from the long-term placement of a port catheter system for the treatment of advanced liver cancer) along with sufficient catheter maintenance. Neither hematoma nor infection at the puncture site was seen although the sheath and the catheter were only fixed with skin at the inguinal region using thread and surgical tape, and without using an indwelling port. However, patients with SAHF are often complicated with coagulopathy. In patients with extensive coagulopathy, we should take proactive efforts to select a small-caliber catheter, such as 3-F system.
This study has some limitations. First, the study population was small. In the group in which a catheter tip was placed in the replaced RHA (4 patients) or the PHA (4 patients), all patients responded to TASIT (Table 3). Additional accumulation of cases may be required for an objective assessment. Second, cases of hepatic failure are sometimes self-limiting, and several cases of complete remission treated only by a conservative therapy have been reported (36). We cannot deny the possibility that such a self-limiting case might have been included in the effective group in this study. Re-evaluation using a randomized control trial is required to settle this issue. A third limitation is the medical safety and ethical problems in undergoing angiography and intra-arterial catheter placement for patients with a bleeding tendency. In general, a low value of prothrombin time or a low platelet count is believed to be a contraindication of angiography. Written informed consent was obtained from the patients, and TASIT was performed under the approval of our hospital's ethics committee.
In the present study, all patients with non-fulminant SAHF responded to TASIT, and successfully avoided progression of SAHF to the fulminant form or referral to liver transplantation. The success rate of TASIT was lower in patients with fulminant form SAHF, and its fatality rate was too high. Still, the catheter placement procedure was relatively simple and easy, and there were no serious complications related to the procedures. Therefore, it is suggested that hepatic artery catheter placement and TASIT can be positively applied to SAHF patients. This study suggests that TASIT following hepatic artery catheter placement is a feasible and efficient treatment option for SAHF regardless of the anatomic variation of the hepatic artery.
In conclusion, indwelling catheter placement in the hepatic artery and intra-arterial steroid infusion therapy can be safely performed for SAHF using intervention techniques. Careful manipulation during the procedure to prevent hepatic artery injury may be the most essential not only for successful TASIT, but also for liver transplantation, which may follow failed TASIT treatment. TASIT is a novel and relatively safe therapeutic choice in the management of patients with SAHF.