
Abstract
Background
In the early phase of viral encephalitis, conventional MRI may appear normal. Diffusion-weighted imaging (DWI) is a sensitive tool for detecting early changes in cellular function in the central nervous system.
Purpose
To investigate the usefulness of DWI in the diagnosis of enterovirus 71 (EV71) encephalitis, and to determine whether DWI is superior to conventional MR sequences.
Material and Methods
MRI scans in 26 patients were retrospectively evaluated for distribution of lesions on T1-weighted images (T1WI), T2-weighted images (T2WI), fluid-attenuated inversion recovery (FLAIR), and DWI. Contrast-to-noise ratios (CNRs) were calculated for all regions on each sequence and differences in the four MRI sequences were assessed using CNRs. Apparent diffusion coefficient (ADC) values were measured for all regions to look for true restriction of diffusion.
Results
Fifteen out of 26 cases showed positive findings on MR imaging. The brain stem was involved in 11 patients, cortex and subcortical white matter in four patients. DWI was more sensitive in detecting the abnormalities (89.7%) compared to T2WI (48.7%), FLAIR (41.0%), and T1WI (35.9%), and the positive ratio of DWI was significantly higher compared to other sequences. Furthermore, no significant difference was found between T2WI and FLAIR (P = 0.649). The corresponding mean CNRs were 8.73 ± 2.57, 83.59 ± 29.28, 24.22 ± 6.22, and 132.27 ± 78.32 on T1WI, T2WI, FLAIR, and DWI, respectively. The absolute values of CNRs of lesions on DWI were significantly greater than those on other sequences.
Conclusion
DWI appears to be more sensitive in detecting EV71 encephalitis than conventional MRI sequences. This capability may improve the accuracy in diagnosing EV71 encephalitis, especially at the early stage.
Keywords
Hand, foot, and mouth disease (HFMD) is a common viral disease, caused by many kinds of viruses, including enterovirus 71 (EV71), coxsackievirus A (CAV), coxsackievirus B (CBV), and echovirus (Echo). EV71 and CAV16 are the most frequent etiologic agents causing outbreaks of HFMD. Although the majority of infections are mild and self-limited, with recovery taking only a short time, previous data have shown that EV71 infections can result not only in febrile disease and herpangina but also in serious complications, such as aseptic meningitis, encephalitis, myocarditis, acute flaccid paralysis(AFP), and even death (1–4).
EV71 encephalitis was first described in the United States in 1974 (5), and several outbreaks have subsequently been reported worldwide, especially in South Asia. A large outbreak of HFMD caused by EV71 and CAV16 occurred in Guangdong, China, in 2009 (6) and in 2010. Although there have been several outbreaks worldwide, there is little information in the literature regarding the MR imaging evaluation of EV71 encephalitis, and this literature primarily concerns the 1998 outbreak in Taiwan.
Shen et al. (7) reported that the majority of EV71 CNS lesions were located in the medulla oblongata, pons, midbrain, and the dentate nuclei of the cerebellum. In addition, in some cases, infection also involved the spinal cord as well as the thalamus and putamina. Chen et al. (8) noted that AFP associated with EV71 infection tends to specifically involve the anterior horn cells of the cord and the ventral roots.
DWI is widely used to evaluate various diseases involving the brain and spinal cord (9, 10), and its role in other conditions, including infection, has been increasingly explored (11). Conventional MR sequences used in routine practice to identify abnormal areas involved with viral encephalitis include T1WI, T2WI, contrast-enhanced T1WI, and FLAIR (12, 13). Recently, DWI has been reported to be more sensitive than T2WI and FLAIR images in the detection of intracranial inflammatory lesions (14–16).
While numerous reports concern the usefulness of DWI in viral encephalitides such as Nepal viral encephalitis and Japanese encephalitis, no study has been conducted to determine the usefulness of DWI for diagnosing EV71 encephalitis.
The purpose of this study was to evaluate the sensitivity of DWI in the diagnosis of EV71 encephalitis, and to determine whether DWI was superior to conventional MRI sequences in detecting CNS viral infection.
Material and Methods
The procedures followed were in accordance with the ethical standards of our committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 1983.
Between July 2010 and February 2011, 26 patients (16 boys and 10 girls, age range 4–60 months) suffering from EV71 infection were enrolled in this retrospective study. All children were admitted into the pediatric intensive care unit (PICU) because of serious CNS symptoms that included herpangina, fever, headache, vomiting, drowsiness, cranial nerve palsies (nerves VI, VII, IX, X, XI), hyperspasmia, tachycardia, shock, dyspnea, and so on. MRI examination was performed during the acute phase of the disease in each patient (2–6 days after onset of symptoms, average time of onset 3.6 days). EV71 was confirmed by the Center for Disease Control and Prevention of Guangdong Province using sequence analysis performed on stool, rectal swab, throat swab, and cerebrospinal fluid specimens.
MR examinations were performed using a 1.5-T MRI (Signa Excite HD, GE Healthcare, Milwaukee, WI, USA) equipped with an 8-channel head coil. The standard MR examinations included T1WI (TR/TE 400/11 ms), T2WI (TR/TE 4300/100 ms), and FLAIR images (TR/TE 8400/120 ms, range of inversion times 2100 ms). All images for all sequences were 5 mm thick with an interslice gap of 1.0 mm. The matrix size was 256 × 256, and the field of view (FOV) was 18 cm.
DWI sequences were acquired using diffusion gradients with a b value of 1000 s/mm2 consecutively applied in x, y, and z directions. We used a single-shot echo-planar DWI sequence with a TR of 6000 ms, a TE of 81 ms, one excitation, and a matrix size of 128 × 128. Contrast-enhanced studies were obtained using intravenous gadopentetate dimeglumine (Gd-DTPA, Magnevist; Bayer Schering Pharma, Berlin, Germany) using 0.1 mmol/kg body weight. SE T1W images were acquired in transverse, coronal, and sagittal planes.
Image sets were transferred to the postprocessing unit. Images of each patient were loaded into a digital picture archiving and communication (PACS) workstation (Centricity; GE Healthcare, Milwaukee, WI, USA). All MRI examinations were reviewed by two radiologists, in consensus, with full knowledge of the patient's clinical findings and history. The locations of the signal abnormalities were identified and signal intensity changes on T1WI, T2WI, FLAIR, and DWI were noted. MR images were retrospectively reviewed, and contrast-to-noise ratios (CNRs) of lesions were measured by subtracting the signal intensities of lesions from those of adjacent or contralateral normal brain parenchyma and dividing by the standard deviation of signal intensities of background noise on T1WI, T2WI, FLAIR, and DWI sequences.
Region-of-interest (ROI) analysis was performed by using manual oval ROI measurements (15 ∼ 20 mm2) in the areas of abnormality. Throughout the study, ROIs were placed by the same author. Apparent diffusion coefficient (ADC) values were computed for all regions on each DWI scan to evaluate for true restriction of diffusion and its quantification. ADC values of the involved and adjacent or contralateral normal brain tissues were compared for each lesion. ADC values were calculated from the ROI by dividing the signal intensity by 1000 to give values in terms of ADC × 10−3 mm2/s.
All analyses were performed using SPSS (Version 13.0, SPSS Institute, Inc. Chicago, IL, USA). To compare the detection rate of various MRI sequences in the diagnosis of EV71 encephalitis, the chi-square test was applied for the numeration data. To assess differences in the four MRI sequences according to the CNRs, the Welch correction test was performed, and to compare two groups, the Dunnett T3 method was used. A P value less than 0.05 was considered significant.
Results
After appropriate clinical management, all 26 patients recovered well within approximately 1 to 2 months, except for one patient who had severe neurologic sequelae, and one patient who died of cardiopulmonary collapse. Overall, 15 out of 26 patients showed positive findings on MRI. The total number of lesions equaled 39. A single lesion was found in two cases and multiple lesions were noted in 13 cases, while most lesions (12 cases) appeared symmetrical.
Of these 15 patients with positive findings on MRI, 11 out of 15 patients presented with abnormal signal intensities in brain stem (Fig. 1), and the remaining four cases involved cortex and subcortical white matter (Fig. 2). In addition, these four cases also presented with diffuse meningeal enhancement, and increased signal intensity was also seen on FLAIR image in the sulci (Fig. 2). Of these 11 patients with the abnormal areas of the brain stem, four cases involved the posterior portions of the medulla oblongata, two cases involved the posterior portions of the midbrain, and five cases involved the posterior portions of the pons (Fig. 1). In these 11 patients, some additional lesions were found in the splenium of the corpus callosum (Fig. 3), dentate nuclei of the cerebellum, the head of caudate nucleus, and the thalamus.
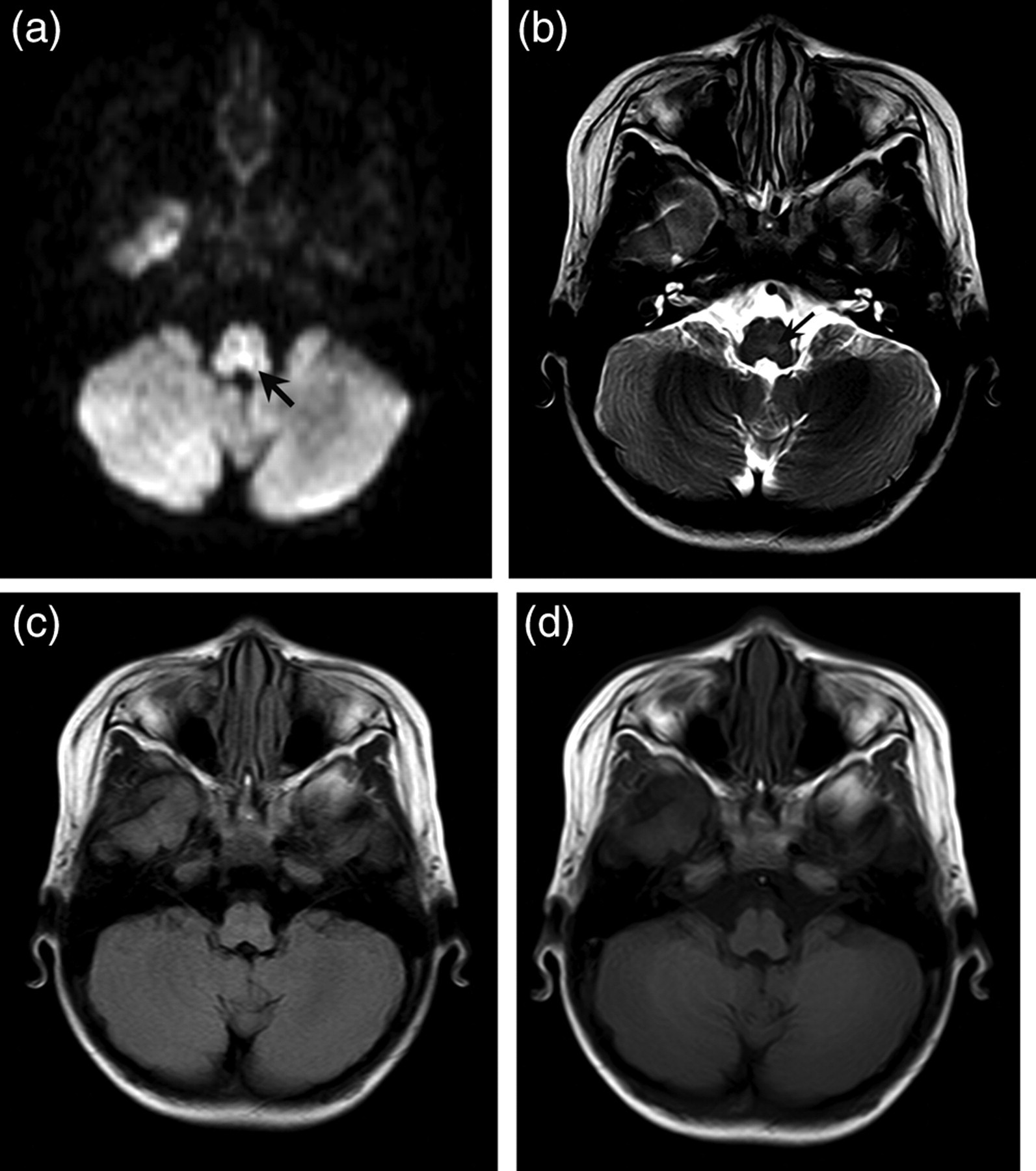
A 1-year-old boy suffering from EV71. (a) DWI shows remarkable hyperintense focal lesion on the posterior portion of left pons; (b) T2WI demonstrates lightly high signal intensity (arrowhead). The lesion is hard to be recognized on FLAIR (c) and T1WI (d)

A 3-year-old boy suffering from EV71 There are extensive lesions in the parieto-occipital cortex and the subcortical white matter on T2WI (a), which are hypointensity on T1WI (b) and hyperintense on FLAIR (c), and increased signal intensity in the sulci on FLAIR images compatible with meningoencephalitis; (d) DWI readily demonstrates high signal intensity; (e) Contrast-enhanced transverse T1WI shows diffuse meningeal enhancement

A 4-month-old infant suffering from EV71. (a) FLAIR reveals no significant abnormality at the splenium of corpus callosum; (b) T2WI demonstrates slightly high signal intensity (arrowhead), but the lesion border is unclear; (c) Low signal intensity on T1WI are unremarkable; (d) DWI in the axial plane shows obviously hyperintense focal lesion (arrowhead) at the splenium of corpus callosum; (e) ADC map shows hypointensity in the lesion due to the restriction
The frequency of lesions detected and signal changes observed using various MRI sequences in all 15 patients are shown in Table 1. Fourteen lesions showed hypointense signal on T1WI, 19 lesions showed hyperintense signal on T2WI, 16 lesions were hyperintense on FLAIR, and 35 lesions were hyperintense on DWI. Only one lesion, which was located in the posterior portion of the medulla oblongata, showed slight enhancement. MRI abnormalities were more common on DWI (89.7%) compared to T2WI (48.7%), FLAIR (41.0%), and T1WI (35.9%), and the sensitivity of DWI was significantly higher compared to the other sequences, while T1WI was the least sensitive compared to the other three sequences (P = 0.000). Furthermore, no significant difference was found between T2WI and FLAIR (P = 0.649).
Frequency of lesions detected and signal changes observed using various MRI sequences in 15 patients with enterovirus 71 encephalitis
The corresponding mean CNRs were 8.73 ± 2.57, 83.59 ± 29.28, 24.22 ± 6.22, and 132.27 ± 78.32 on T1WI, T2WI, FLAIR, and DWI, respectively. The absolute value of lesion CNRs on DWI were significantly greater compared to those on T2WI, FLAIR, and T1WI, while the CNRs of lesions on T1WI were lowest (P = 0.014). Comparing CNRs between T2WI and FLAIR, no significant difference was noted (P = 0.312).
The ADC value in each lesion was lower than the corresponding normal brain tissue, which confirmed true restriction of diffusion. The mean ADC value in the 35 lesions on DWI was lower (0.803 ± 0.110 × 10−3 mm2/s) than that of corresponding normal brain tissues (0.996 ± 0.486 × 10−3 mm2/s).
Discussion
During the endemic spread of HFMD caused by EV71, CNS infections are frequently diagnosed and may lead to severe neural injury or even death. Therefore, accurate diagnosis at an early stage is crucial. We found that DWI was more sensitive in detecting abnormalities in EV71 encephalitis (P = 0.000), and we demonstrated that absolute values of CNRs on DWI were significantly higher compared to those on T1WI, T2WI, T2-FLAIR (P = 0.014). Although T2WI had higher positive ratios and greater CNRs compared to FLAIR, there was no significant difference between the two sequences in the diagnosis of EV71 encephalitis.
Although EV71 encephalitis is a type of viral encephalitis, its characteristic imaging features are different from the other common viral infections. Knowledge of the typical MR imaging findings of EV71 encephalitis is crucial for guiding diagnosis. The locations in our cases primarily involved the posterior aspects of the medulla oblongata, midbrain, and pons, but EV71 may also rarely involve the dentate nuclei of the cerebellum and the head of caudate nucleus. The lesions usually showed hypointensity on T1WI and hyperintensity on T2WI or FLAIR, DWI also revealed hyperintensity during the acute stage. The lesions showed almost no enhancement, and the patients were sometimes complicated by aseptic meningitis.
Reports concerning MR findings in EV71 encephalitis are limited, and our findings correlate with the previous reports (7, 8). According to the literature, typical locations primarily involved with infection include the posterior portion of the brain stem and spinal cord, while the bilateral dentate nuclei of the cerebellum, bilateral putamina and thalami are rarely involved. When the disease involves the posterior portion of the medulla oblongata, the dorsal nuclei of the vagus nerve, the medial longitudinal fasciculus, the reticular formation, and the nuclei of the solitary tract may be affected. If the portion of the pons and midbrain were involved, the nuclei of cranial nerves III and IV, VI, VII and IX may be affected. The accompanying radiculomyelitis of EV71 encephalitis is uncommon and tends to involve unilateral the anterior horn cells of the cord and the ventral roots (8). Like other common viral encephalitis, cortex and subcortical white matter was involved in only a few of our patients, although there is no report of cortex and subcortical white matter involvement with EV71 in the published literature (7, 8). The meningeal involvement in four of our patients was nonspecific and cannot be seen on DWI.
FLAIR has been reported to be more sensitive than T2WI in detecting encephalitic lesions (12, 17), nevertheless, we found that the sensitivity of FLAIR was not superior to T2WI in detecting EV71 lesions. This result is similar to most earlier reports, possibly due to the fact that the EV71 encephalitis frequently involves the brain stem, whereas other viral encephalitides usually involve the cortical and subcortical white matter. In present study, we found FLAIR was superior to T2WI for the evaluation of cerebral lesions, but T2WI was superior to FLAIR for detection of brain stem lesions. These findings are in agreement with a report concerning Japanese encephalitis (18).
During the acute stage of EV71 encephalitis, T2WI revealed hyperintense areas that were not seen on T1WI, reflecting acute inflammation of brain tissue, and these findings are in agreement with one report (7).
More recent reports in the literature indicate that DWI can be useful in the early diagnosis of the neurological complications associated with CNS infections (19, 20). We evaluated the ability of DWI to visualize encephalitic lesions in EV71 compared to conventional MRI.
DWI provides a novel way to characterize tissues based on its sensitivity to the molecular motion of water. The characteristic histologic changes associated with EV71 encephalitis in the acute stage are associated with inflammatory cell infiltration of the brain parenchyma or meninges, cytotoxic edema, necrosis, and perivascular cuffing. It is possible that these changes are responsible for the cytotoxic edema that leads to restricted diffusion and low ADC. The involved areas on DWI are seen as hyperintense lesions. While in the subacute stage, the components of vasculitis and perivascular cuffing diminish, and the proportion of diffusion restriction decreases as ADC starts to increase. Thus, DWI may be less sensitive if the MRI study is delayed. In newborns and infants, DWI proved successful in demonstrating the acute infectious process even before detection by conventional MRI sequences. To a large extent this relates to the water content of the immature brain and the problem achieving conspicuity as conventional MRI cannot differentiate between the normal watery brain and infectious lesions (21).
All of our patients were infants, and MRI was carried out within 7 days after onset of symptoms which may be responsible for the high sensitivity of DWI found in our study, as DWI not only detects early encephalitic lesions more effectively, but also depicts the border of infected areas more precisely. DWI is widely used in various infections and is felt to be the most sensitive test for the early clinical diagnosis of Creutzfeldt-Jakob disease (CJD) (22). DWI may also help in the staging of the disease (23). It also can differentiate necrotizing herpes simplex encephalitis (HSE) from non-necrotizing JE by correlating ADC values. In HSE lesions, there is restricted diffusion with low average ADC values observed in the acute stage, in contrast to JE lesions, which do not show either restricted diffusion or low ADC values during the acute stage (18).
The intrinsic T2 signal characteristics of the affected tissue termed the ‘shine-through effect’ must be considered in the evaluation of the hyperintensity seen on DWI (24). One method by which the T2 ‘shine-through effect’ can be eradicated is to generate an ADC map that reflects only the diffusion properties of water and not the characteristics of the T2 signal. ADC values are the quantitative expression of abnormal water diffusion in the brain parenchyma. ADC mapping is crucial for interpreting diffusion images, and the ADC map adds further sensitivity and specificity compared with DWI alone. In our study, the ADC values of each lesion were lower than that of corresponding normal brain tissue.
Brain stem encephalitis could be caused by a variety of viruses, mainly including poliovirus, Japanese encephalitis virus, and so on (25, 26). Poliomyelitis is tend to involve symmetrical anterior horn of the spinal cord (25), however, unilateral anterior horn and contrast-enhanced the ventral roots are usually seen in accompanying poliomyelitis of EV 71 encephalitis (8). In Japanese encephalitis, the lesions are characteristically seen in thalamus, basal ganglia, and brain stem, and less commonly in cortex and subcortical area (17, 26), maybe the clinical symptom of herpangina in EV 71 infection is potentially distinguishable.
Our study had several limitations. We evaluated a relatively limited number of patients, and the histopathological correlation was not available in all cases. Furthermore, follow-up MR imaging was not carried out, so we could not evaluate the role of DWI in the subacute or chronic stage of EV71.
In conclusion, DWI has a short acquisition time which is suitable for pediatric cerebral MRI examinations. Our study suggests that the DWI sequence is more sensitive compared to routine MRI sequences in patients with EV71 encephalitis, especially in the early stage. In addition, measurement of ADC can supply additional quantitative parameters, which may prove helpful in monitoring the progression of the disease.
Footnotes
ACKNOWLEDGEMENTS
This work was partially supported by Science and Technology Planning Project of Guangdong Province, China (2009B080701053).