
Abstract
Background
Cerebral microbleeds (CMBs) detected by gradient-echo MRI have been proven to be a potential risk factor for further bleeding, while the association between CMBs and the first onset of intracerebral hemorrhage has not been well investigated.
Purpose
To analyze the association between CMBs and the first onset of primary intracerebral hemorrhage (pICH).
Material and Methods
Two hundred and two consecutive inpatients with ICH and 234 consecutive outpatients without ICH as control group were enrolled in this study. MR imaging including T2*-GRE, T1W, T2W and fluid attenuated inversion recovery (FLAIR) sequences were performed to detect CMBs and other abnormalities. Prevalence, distribution, and grades of CMBs, as well as the location and size of the intracerebral hematoma were analyzed, respectively. Comparison was made between pICH and control group. Logistic analysis was performed to evaluate the association between CMBs and ICH. The correlation between hematoma size and CMBs grade/numbers was analyzed.
Results
CMBs were detected in 140 patients in pICH (69.3%) group and 62 patients in control group (26.5%). The incidence of CMBs in pICH group was significantly higher than that in control group (P < 0.0001). As the logistic regression analysis results, CMBs was the risk factor associated with ICH, with modulation OR value of 8.363 (95% CI 5.210–13.421). The volume of ICH with CMBs was 12.57 ± 17.23 mL, and the volume of ICH without CMBs was 17.77 ± 26.97 mL. Negative correlation was demonstrated between CMBs number and ICH volume (rs = −0.1769, P = 0.0118), as well as between CMBs grade and hematoma volume (rs = −0.1185, P = 0.1557).
Conclusion
CMBs may be an independent risk factor for the first onset of intracerebral hemorrhage.
Cerebral microbleeds (CMBs), also called hemorrhagic lacunes or petechial hemorrhage, demonstrate homogeneous round signal loss lesions with a diameter of up to 5 mm on T2*-weighted gradient echo (T2*-GRE) imaging (1). Previous studies have called attention to the frequent observation of small areas of signal loss in patients with primary intracerebral hemorrhage (pICH), which may represent residues of earlier clinically silent microbleeds (2, 3). A histopathologic study has proven that these signal loss lesions indicate previous blood extravasation (4, 5), of which perivascular hemosiderin deposition around angiopathic arterioles was confirmed as predominant cause (6, 7). Until recent years, CMBs had been usually ignored clinically, because of their asymptomatic nature. It has been found in several studies that CMBs are associated with bleeding occurring in patients with previous hemorrhagic or ischemic stroke, especially those who have accepted systemic anti-platelets therapy (8–10). This finding suggest that this pathological change may be an important risk factor for occurrence of intracerebral hemorrhage (ICH). However, the relationship between CMBs and the first onset of ICH has not been fully understood.
Gradient echo technique has been proven to have high sensitivity for detection and display of CMBs for magnetic susceptibility enhanced effects of hemosiderin (11). Until now, most studies on CMBs were performed using 1.5 T MR scanners. In recent years, 3.0 T MR units have been frequently applied in clinical practice. The high signal-to-noise ratio and spatial resolution is superior to obtain precise anatomical information and surrounding structures of lesions in the central nervous system (12). Compared with examinations on a lower magnetic field MR unit, T2*-GRE sequence on 3.0 T MR is more sensitive for detection of microbleed lesions.
In this study, we retrospectively analyzed prevalence and distribution patterns of CMBs in a large consecutive series of patients with the first onset of pICH using 3.0 T MR. We analyzed the association between CMBs and occurrence of pICH, as well as between numbers of CMBs and size of intracerebral hematoma. Comparison analysis was also performed between pICH group and non-pICH group.
Material and Methods
Subjects
The study population consisted of 202 consecutive pICH inpatients (127 men, 75 women, mean age 56.64 ± 13.44 years) with consistent clinical symptoms and confirmed by computed tomography (CT) or MRI, retrospectively collected from September 2007 to September 2010. A cohort of 234 consecutive non-pICH outpatients (146 men, 88 women, mean age 60.83 ± 10.55 years) with no ICH history during the same period were retrospectively collected as control group. Inclusion criteria for the control group included patients with suspected ischemic cerebrovascular disease, TIA symptoms, or hypertension. Patients with any history or recognized evidence of acute ischemic or hemorrhagic stroke were excluded from the control group. The exclusion criteria for both groups included traumatic cerebral hemorrhage, hemangioma, bleeding secondary to vascular malformation, hemorrhagic transformation of an ischemic stroke, intracranial neoplasia, moyamoya disease, subarachnoid hemorrhage, primary intraventricular hemorrhage, and any history of brain surgery. This study was approved by the ethics committee, and informed consent was obtained from all patients.
MR imaging
For pICH and control subjects, the same MRI protocol including T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), fluid attenuated inversion recovery (FLAIR), and T2*-GRE sequence was performed using a 3.0 T MR unit (Siemens Magnetom Trio-Tim, Erlangen, Germany). The parameters of T2*-GRE sequence were: TR/TE = 215/10 ms, flip angle = 20o, FOV = 220 mm × 220 mm, matrix size = 256 × 256. For each sequence slice thickness was 5 mm, gap width was 1.5 mm.
Image assessment
All images were reviewed by two experienced neuroradiologists who were blinded to the patients' clinical information. The prevalence and distribution of CMBs, the size and location of intracerebral hematoma were analyzed respectively. A consensus was obtained when the results from two neuroradiologists were different.
CMBs were defined as a homogeneous, round signal loss lesion with a diameter of up to 5 mm on T2*-GRE sequence (Fig. 1a–e). The numbers of CMBs were recorded according to their different locations, including cortical–subcortical regions, basal ganglia, thalami, brainstem, and cerebellum. CMBs were graded from I to III according to the total number of CMBs: Grade I, mild (total number of CMBs, 1–5); Grade II, moderate (6–15); Grade III, severe (>15).
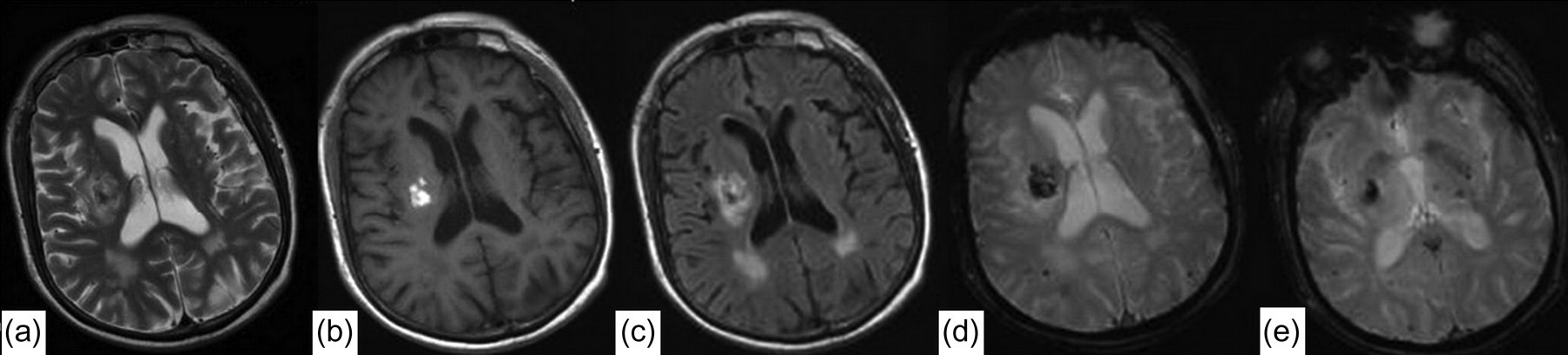
Axial MR images of a 70-year-old male patient with pICH. The hemorrhage lesion displayed patchy abnormal signal located in right basal ganglia (a, b, c). T2*WI GRE sequence demonstrated low signal intensity. Multiple dotty low signal intensity lesions were found in subcortical area, thalami, and basal ganglia (d and e)
For the pICH group, intracerebral hematomas were grouped by its location: (a) lobar, involving the cortex and/or subcortical regions; (b) basal ganglia/thalamic; and (c) infratentorial, involving the brain stem and/or the cerebellum. The size, signal, and other abnormal changes around hematoma of each ICH lesion were evaluated.
Statistical analysis
Categorical variables were presented as percentage and continuous variables were expressed as mean ± SD or median (Q1–Q3). Chi-square test and Fisher exact test, as appropriate, were used for comparison of normally and non-normally categorical variables, respectively. Student's t test was used for comparison of normally distributed variables, while Wilcoxon rank sum score was used for non-normally distributed variables. Correlation of ICH and CMBs was analyzed using logistic regression model, Spearman correlation coefficient was used to evaluate the association of size of hematoma and CMBs grade/numbers. All analysis were performed with SAS software version 9.1 (SAS Institute Inc, Cary, NC, USA). P < 0.05 was considered statistically significant.
Results
Patients' characteristics
The clinical data of the two groups are summarized in Table 1. The age of the pICH group was lower than that of the control group (P = 0.0004); also the patients with CMBs in the pICH group were younger than patients with CMBs in the control group (P = 0.02). For the pICH group, the age of patients with CMBs was higher than that of patients without CMBs (P = 0.01), while for the control group, no significant difference was found between the age of patients with and without CMBs. There were more male patients than female patients within both groups, while no significant difference of gender distribution was found between two groups.
Age and gender distribution of patients of pICH group and control group
*t value
†χ2 value
Prevalence, grade, and distributional characteristics of CMBs
CMBs were detected in 69.3% (140/202) of the patients in the pICH group, and 26.5% (62/234) patients in the control group, respectively. The incidence of CMBs in the pICH group was much higher than that of control group (χ2 = 79.9100, P < 0.0001), with OR values of 6.2643 (95% CI: 4.1293–9.5032). The cases with different CMBs grade in both groups are summarized in Table 2. For both groups, case number decreased in higher CMBs grade level. However, the percentage of CMBs grade II and grade III cases in the pICH group was larger than that of the control group.
Number of cases of different grade for pICH and control groups
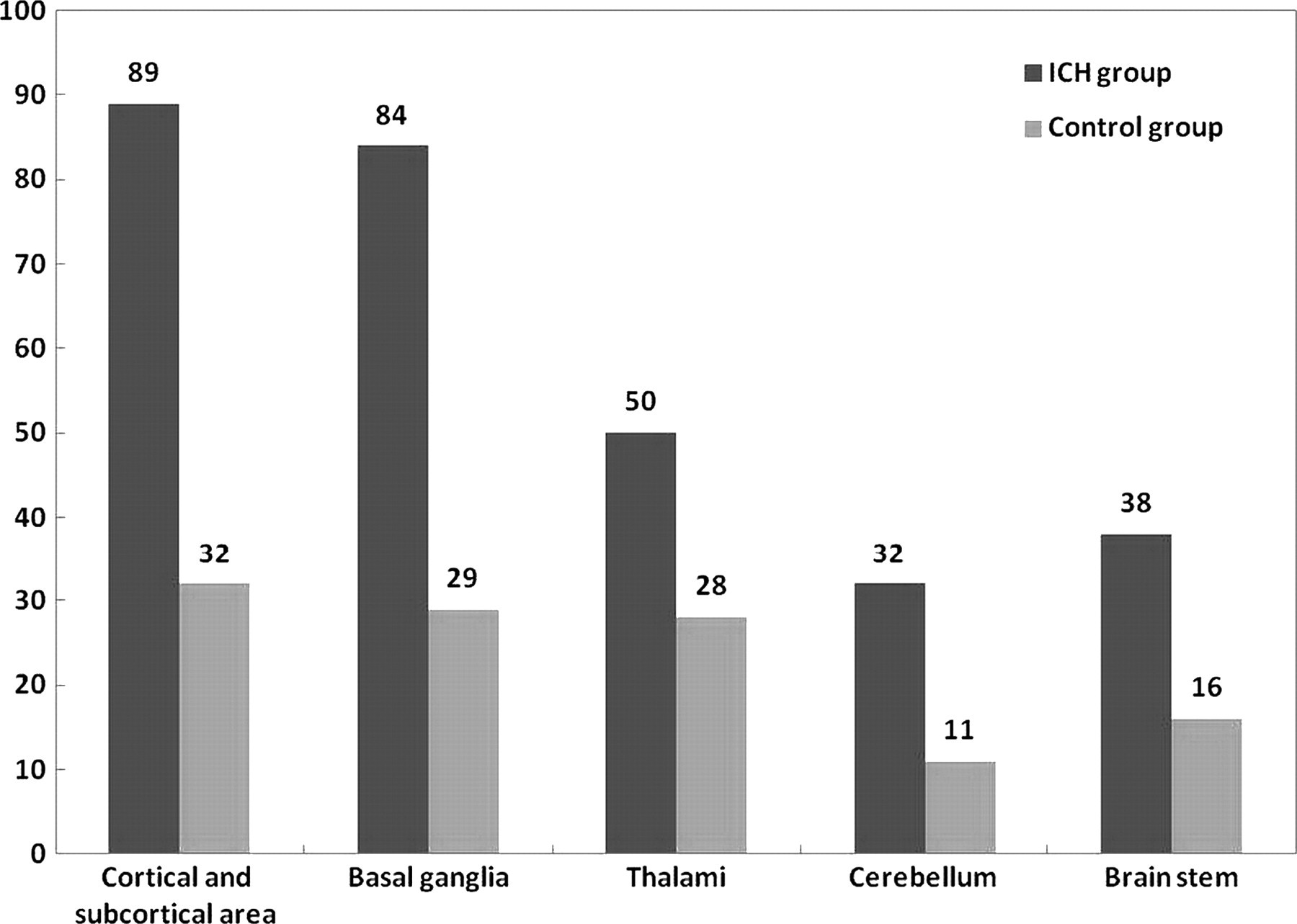
The regional distribution of CMBs for both groups are demonstrated in Fig. 2. For the pICH group, CMBs were most frequently found in the cortical–subcortical regions in 89 (63.57%) of the cases with mean number 2.89, followed by basal ganglia in 84 (60%) of the cases with mean number 1.74, thalami in 50 (35.71%) cases with mean number 1.07, brain stem in 38 (27.14%) cases with mean number 0.64, and cerebellum in 32 (22.86%) cases with mean number 0.66. The same tendency of CMBs distribution was identified in the control group. CMBs in cortical–subcortical regions were detected in 32 (51.61%) cases, followed by basal ganglia in 29 (46.77%) cases, thalami in 28 (45.16%) cases, brain stem in 16 (25.81%) cases, and cerebellum in 11 (17.14%) cases.
Analysis of the location and frequency of CMBs according to anatomic division in patients of pICH group and control group
MR features of intracerebral hematoma
For the pICH group, the clinically symptomatic hematoma was lobar in 60 (29.70%) cases, 56 (27.7%) cases were located in the basal ganglia, 69 (34.16%) cases in thalami, 12 (5.94%) in brain stem, and 7 (3.4%) in cerebellum, respectively. The mean volume of ICH was 14.61 mL, with the median of 6.19 mL and quartile volume of 1.2–20.13 mL. The signal intensity of a hematoma was homogenous (9.9%) or heterogenous (90.1%). The perifocal edema was displayed in 90% of lesions with different degree.
Correlation analysis between pICH and CMBs
Logistic regression analysis was performed to analyze the correlation between pICH and CMBs. Variables including CMBs, sex, age, white matter changes, and lacunar infarction were put into the risk factor regression equation. The results showed that CMBs and age were risk factors for pICH. After adjusting risk factors of age, sex, demyelinating change, and lacunar infarction, CMBs were identified as the independent risk factor associated with pICH, with the modulation OR value of 8.363 (95% CI: 5.210–13.421). The incidence of pICH in patients with CMBs is much higher than that of patients without CMBs as reviewed in Table 3.
Multiple logistic regression analysis of risk factors about ICH
Correlation between volume of pICH and CMBs grade
The mean volume of pICH in patients with CMBs was 12.57 ± 17.23 mL, with median (Q1–Q3) 4.67 mL (0.68, 18.82). The mean volume of pICH without CMBs was 17.77 ± 26.97 mL, with median (Q1–Q3) 8.52 mL (3.06, 23.60). The volume of pICH with CMBs was smaller than that without CMBs with a statistically significant difference of P = 0.0418. Spearman correlation analysis revealed a negative correlation between CMBs number and hematoma volume (rs = −0.1769, P = 0.0118), as well as between CMBs grade and hematoma volume (rs = −0.1185, P = 0.1557).
Discussion
CMBs have attracted more and more attention in clinical and research fields. The existence of CMBs in different population has been reported in the literature. CMBs are detected not only in patients with ICH but also in patients with ischemic stroke and even in a small proportion of asymptomatic elder individuals (13–15). The prevalence of CMBs varied in previous studies. A wide range of 18–65% in patients with ischemic stroke has been reported. In this study, we found evidence of old CMBs in 69.31% of patients with pICH. The incidence was higher than the results of 54% in a previous study by Roob et al. (7). Greenberg et al. (4) reported a high incidence of CMBs (80%) in patients with ICH, however, this result was limited by small sample size and enrollment of only lobar ICH patients. In our control group, the prevalence of CMBs was 26.50%, which was similar to previous studies with a prevalence range from 21.30–29.10% (16–19). The discrepancy of CMBs prevalence can be explained by different study population and protocol used in each research.
Several studies reported that CMBs were detected in ICH patients, suggesting that the distribution of old CMBs may be related to the occurrence of pICH (4, 20, 21). However, no comparison between CMBs and first onset of pICH has been reported. Our results demonstrate that the probability of pICH occurrence in patients with CMBs is much higher (more than eight times) than that in patients without CMBs, indicating that CMBs is an important risk factor for the first onset of pICH.
Previous studies have suggested that CMBs are closely related to increasing age and hypertension (19, 22). Our results show that in the pICH group, the mean age of patients with CMBs was higher than those without CMBs, while no significant difference was found in the control group. The result indicates that CMBs may be closely associated with relatively aged pICH patients. Histopathology has demonstrated that CMBs are focal accumulations of hemosiderin-containing macrophages adjacent to small vessels (6). For aged patients, gradually developed degeneration of the elastic fiber and smooth muscle of the vessel wall would result in increased fragility of small arteries, where the micro-vascular aneurysms may form, and finally lead to CMBs or ICH.
The distributions of CMBs were also analyzed in this study. For both the pICH and control groups, the common locations of CMBs were cortical–subcortical areas, basal ganglia, and thalami, followed by brain stem and cerebellum, which was consistent with previous literature (15). The distribution of symptomatic hematomas was correspondingly often located in the lobar, basal ganglia, and thalami areas. The resemblance of locations of CMBs and ICH may also suggest that there is a possible association between CMBs existence and the onset of ICH.
CMBs were classified into three grades in this study. The percent of grade II and grade III cases in the pICH group were larger than that in the control group. This suggests that a large number of CMBs may be associated with pICH. Cerebral amyloid angiopathy (CAA) is a disease characterize by multiple CMBs in the brain, which has a great tendency of hemorrhagic stroke attacks. Histopathologic findings suggested a combination of CAA with hypertensive microangiopathy as a cause of more widespread distribution of CMBs in some patients (6, 23–25). It is supposed that some cases in this study were possibly CAAs, especially grade III cases. It is unable to confirm whether there is a specific distribution pattern of CMBs in CAA. The features of CMBs in CAA may be identified in further study by further investigations.
Our results showed that hematoma volumes decreased with increasing CMBs numbers/grade in contrast to the previous study by Lee et al. (10), finding that the volume of cerebral hemorrhage in patients with CMBs was two to three times larger than that without CMBs. The difference may be explained by different study populations from different ethics and regions. Also, the size of the hematoma varied in different stages, which may be influenced by the time at examination. Since there are only a few studies focusing on this aspect, there may be other unknown reasons to be explored in further studies.
Our study is limited by its retrospective nature. Although the results showed association between CMBs and pICH, a large-scale prospective case-control study with long-term follow-up in patients with/without CMBs would be more convincing. The clinical information of the subjects in this study was relatively insufficient. A couple of risk factors including hypertension may be helpful to explain some results of this study. Susceptibility weighted imaging (SWI) sequence which is more sensitive to hemosiderin can be used to detect CMBs as a better alternative in the further study.
In conclusion, CMBs have been proven to be an independent risk factor of pICH, and is closely associated with the first onset of hemorrhagic stroke. It is suggested that more attention should be paid to patients with CMBs detected by MR examination in clinical practice.
Footnotes
ACKNOWLEDGEMENTS
This work was supported by the National Key Project of Scientific and Technical Supporting Programs funded by the Ministry of Science & Technology of China during the 11th five-year plan (No. 2007BAI05B07).