
Abstract
Background
In the primary infection of pulmonary histoplasmosis, pulmonary lesions are commonly solitary and associated with hilar and/or mediastinal nodal diseases, which spontaneously resolve, resulting in calcifications in individuals with normal cellular immunity.
Purpose
To assess the lymphatic drainage to the mediastinum from each pulmonary segment and lobe using computed tomographic (CT) observations of a calcified primary complex pulmonary histoplasmosis and predict which patients with N2 disease that would benefit from surgery.
Material and Methods
We collected 585 CT studies of patients with primary complex histoplasmosis consisting of solitary calcified pulmonary lesions and calcified hilar and/or mediastinal nodal disease. Using the N stage criteria of non-small cell lung cancer, we assessed the distribution of the involved hilar and mediastinal nodes depending on the pulmonary segment of the lesion, with a focus on skip involvement. We also assessed the correlation between the incidence of N1and skip N2 involvement and the mean number of involved mediastinal nodal stations in the non-skip N2 and skip N2 groups.
Results
Skip involvement was common in the apical segment (9/45, 20.0%), posterior segment (7/31, 22.6%), and mediolbasal segment (13/20, 65.0%) in the right lung, and in the apicoposterior segment (7/55, 12.7%), lateral basal segment (6/26, 23.1%), and posterobasal segment (16/47, 34.0%) in the left lung. The incidence of skip involvement in each segment showed a significant inverse correlation with that of N1 involvement (r = –0.51, P <0.05) in both lungs. The mean number of involved mediastinal nodal stations in the non-skip N2 and skip N2 groups in all segments of both lungs were 1.4 (434/301) and 1.2 (93/77), and the former was significantly greater than the latter (P <0.01).
Conclusion
Our data showed a predictable pattern of segmental and lobar lymphatic drainage to the mediastinum and suggested that skip involvement could represent the initial mediastinal node involvement via direct lymphatic drainage.
Keywords
The most important prognostic factor in operable non-small cell lung cancer (NSCLC) is lymph node metastasis, and the involvement of mediastinal lymph nodes is considered to be an adverse prognostic factor (1). However, the prognosis of N2 disease is heterogeneous, and several factors, including unsuspected pathologically detected metastasis, skip metastasis, regional metastasis, and one-station mediastinal lymph node metastases suggest favorable survival rates (2–9). To appropriately select the patients with N2 disease who would benefit from thoracotomy and to determine the extent of adenectomy that should be performed during thoracotomy, many authors have analyzed prognostic factors in resected N2 disease with a particular focus on the distribution of mediastinal node metastases (2–17). However, the pulmonary lymphatic drainage patterns are extensive and variable, and those in each lobe still remain to be clarified.
Histoplasmosis is an endemic fungal disease caused by Histoplasma capsulatum, and its infection is particularly prevalent in the central and eastern United States. The infection primarily occurs in the lung resulting from inhalation of airborne spores. In primary infection, pulmonary lesions are commonly solitary and associated with hilar and/or mediastinal nodal disease. In individuals with normal cellular immunity, pulmonary histoplasmosis spontaneously resolves and results in a calcified primary complex consisting of a calcified pulmonary nodule and calcified hilar and/or mediastinal nodes, similar to the Ranke complex of primary tuberculosis (18). Therefore, a calcified primary complex is a common finding on chest CT studies in patients from an endemic area (Fig. 1).
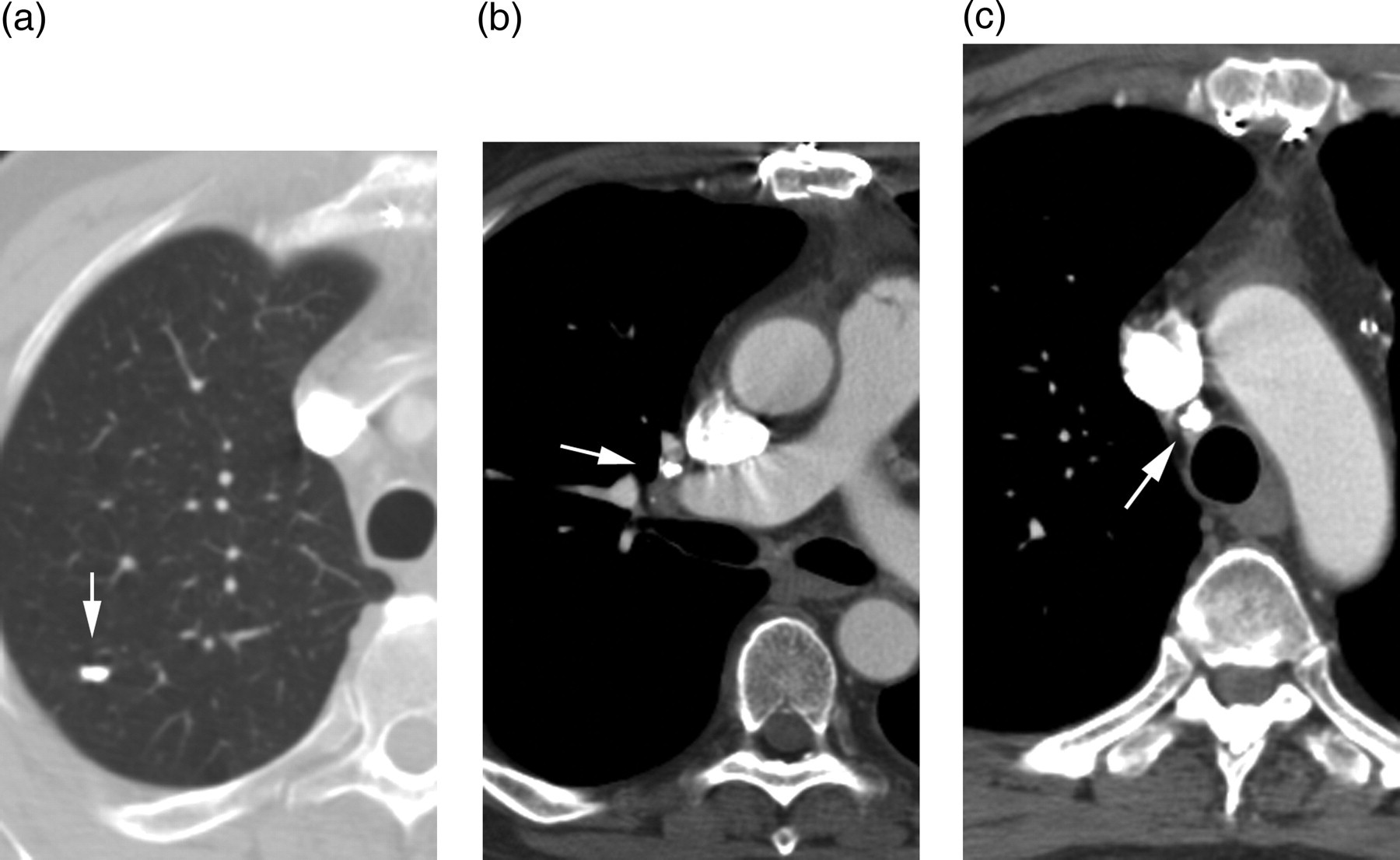
A 50-year-old woman with primary complex histoplasmosis in the right upper lobe. (a) CT with the lung window settings showed a calcified nodule at the apical segment of the right upper lobe (arrow); CT with the mediastinum window settings at the level of the hilum (b) and mid-trachea (c) showed a right hilar (arrow in (b)) and right lower paratracheal (arrow in (c)) calcified node, respectively. The high attenuation in the superior vena cava represents the injected contrast material
In this study, we retrospectively assessed the CT images of the primary complex of pulmonary histoplasmosis for the distribution of involved hilar and/or mediastinal lymph node stations depending on each segment of the lung in order to clarify the pulmonary lymphatic drainage to the mediastinum.
Material and Methods
Study subjects
We examined all subjects in whom a clinical diagnosis of primary complex of pulmonary histoplasmosis was made from January 2004 to January 2005 using CT findings, which included the association of single or multiple well-defined calcified lung nodules and hilar and/or mediastinal calcified lymph nodes. These findings were generally considered to be diagnostic of primary complex of pulmonary histoplasmosis in an area endemic for histoplasmosis. Patients with a clinical history of tuberculosis, sarcoidosis, or pneumoconiosis were excluded so as to avoid intrathoracic calcifications of other etiologies. The pulmonary lesion was solitary in 585 patients and multiple in 256 patients (total 841 patients). Only patients with solitary pulmonary lesions were enrolled in this study to assess the lymphatic flow from a specific pulmonary segment to the hilum and mediastinum. In 585 patients with primary complex pulmonary histoplasmosis with solitary pulmonary lesions, 191 showed only hilar node calcifications, 320 showed both hilar and mediastinal node calcifications, and 74 showed only mediastinal node calcifications. The institutional review board approved this retrospective study without requirement of informed consent.
CT examination and interpretation
All CT studies were performed with 4- or 6-detector row CT scanners (Aquillion, Toshiba Medical Systems, Tokyo, Japan, or Emotion 6, Siemens Medical Solutions, Erlangen, Germany) with the following scan parameters: 135kV, 130mAs, gantry rotation time of 0.5 s, 3-mm collimation, and a pitch of 1. All CT images were reconstructed with contiguous 3-mm thick slices and displayed on a workstation monitor (AR28, System 5 workstation, Kodak, Tokyo, Japan). The images were assessed with both lung (window level of –500 HU and window width of 2000 HU) and soft tissue (window level of 40 HU and window width of 400 HU) window settings, which were voluntarily adjusted, if necessary. The patients received 80–150 mL of non-ionic IV contrast material (Omnipaque [240 mg I/mL], Amersham Health, Princeton, NJ, USA) at an injection rate of 2 mL/s, depending on the clinical indications of the CT studies.
A single experienced pulmonary radiologist subsequently assessed all CT data. In patients with a calcified primary complex of histoplasmosis, we determined the segment of the pulmonary lesion within a lobe and the extent of nodal disease using the N staging of NSCLCs: hilar (N1), ipsilateral mediastinal (N2), and contralateral mediastinal (N3). Skip involvement was defined as mediastinal node involvement without intrapulmonary or hilar node involvement (Fig. 2) (19, 20). In patients with mediastinal nodal disease, the site of nodal involvement was determined according to the classification advocated by the American Thoracic Society, American Joint Committee on Cancer and the Union Internationale Contre le Cancer (AJCC-UICC), which was designed primarily for the staging of bronchogenic carcinoma (19): #1 highest mediastinal, #2 upper paratracheal, #3 prevascular and retrotracheal, #4 lower paratracheal, #5 subaortic, #6 para-aortic, #7 subcarinal, #8 paraesophageal, and #9 pulmonary ligament node. We assessed the incidence of N1, N2 (non-skip N2 and skip N2) and N3 disease in each segment, the correlation coefficient between the incidence of N1 and that of skip N2, and the mean number of involved mediastinal node stations in non-skip N2 and skip N2 patients in all segments. We further assessed the distribution of the involvement of each mediastinal nodal station according to the involved pulmonary segments. Calcifications within the lesion were initially evaluated by qualitative assessment, and the region of interest measurement was used in equivocal cases. An attenuation value greater than +200 HU was considered to reflect calcifications. For nodal disease, we considered both partial and total calcifications to be significant.
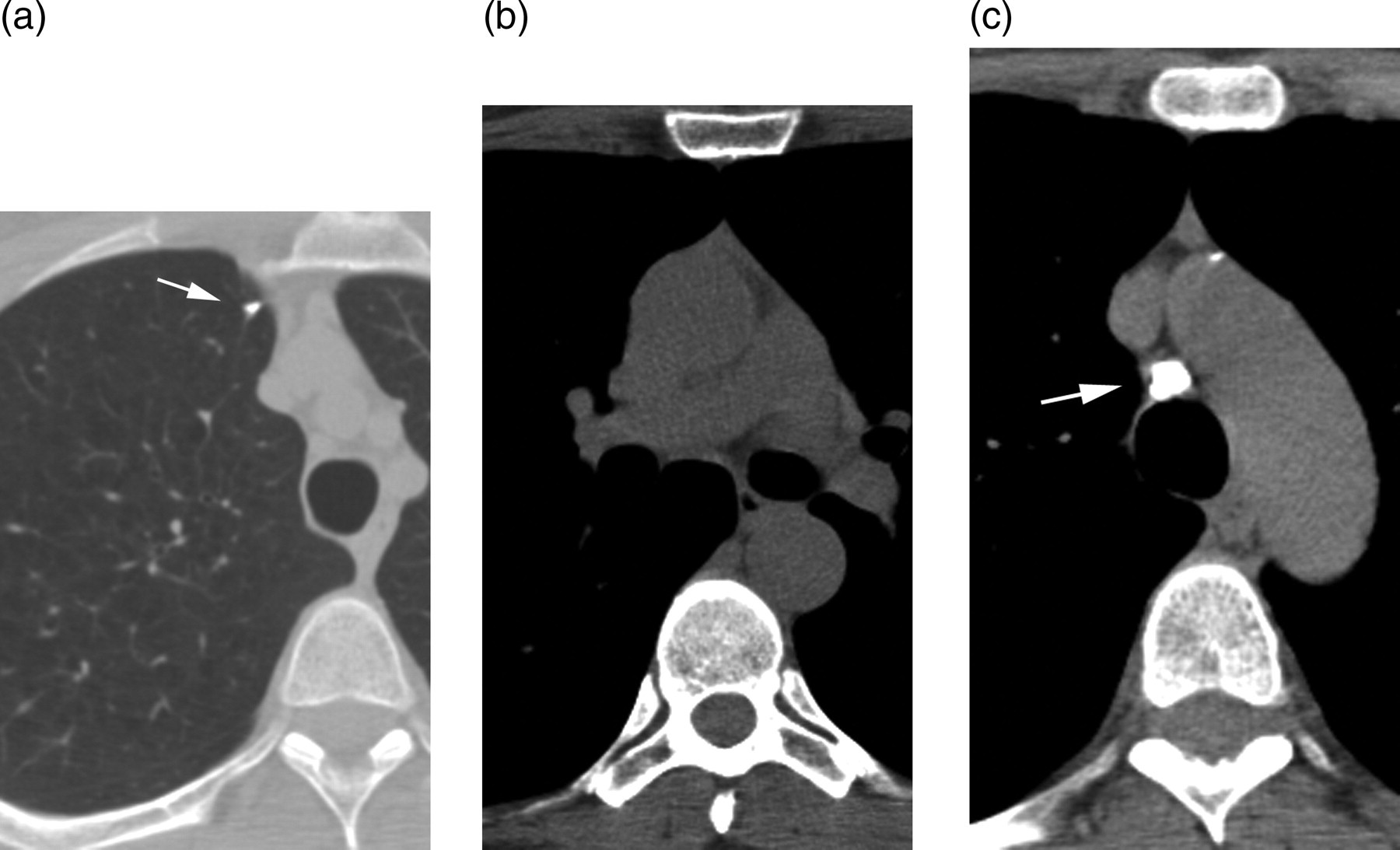
A 56-year-old woman with skip involvement from a right upper lobe histoplasmosis. (a) CT with the lung window settings showed a calcified nodule at the anterior segment of the right upper lobe (arrow in (a)); CT with the mediastinum window settings at the level of the hilum (b) and mid-trachea (c) showed a calcified right lower paratracheal node (arrow in (c)) but no calcified node in the hilum
Statistical analysis
For the statistical comparative analysis of the mean values and assessment of the relationship of the proportions between two groups, we used the two sample t-test and a correlation coefficient, respectively. Parameters with a P value < 0.05 were considered to be statistically significant, and all tests were two tailed.
Results
The incidence of nodal involvement patterns
Table 1 shows the incidence of N1, non-skip N2, skip N2, and N3 pattern involvement in each segment of both lungs. The incidence of skip N2 involvement varied depending on the segments in both lungs. In the right lung, skip involvement was relatively common in the apical segment (9/45, 20.0%), posterior segment (7/31, 22.6%), and anterior basal segment (13/20, 65.0%). In the left lung, skip involvement was common in the apico-posterior segment (7/55, 12.7%), lateral basal segment (6/26, 23.1%), and posterior basal segment (16/47, 34.0%). In each segment of both lungs, the incidence of skip involvement showed a significant inverse correlation with that of N1 involvement (r = –0.51, P < 0.05).
Distribution of patients in relation to the N staging and pulmonary segments
The mean number of involved mediastinal nodal stations in the non-skip N2 and skip N2 patients in all segments of both lungs were 1.4 (434/307) and 1.2 (93/77). The mean number of involved mediastinal nodes in the non-skip group was significantly greater than that in the skip group (P <0.01).
Mediastinal node involvement in relation to the pulmonary segment
Table 2 shows the distribution in the involved mediastinal nodal stations, including that of skip involvement, depending on the pulmonary segment in patients with N2 pattern disease.
Distribution of mediastinal lymph node involvement in relation to the pulmonary segment in patients with N2 pattern disease
*Upper paratracheal
†Prevascular and retrotracheal
‡Lower paratracheal
§Subaortic
**Para-aortic
††Subcarinal
‡‡Paraesophageal
§§Pulmonary ligament
n = number of N2 patients; ns = number of skip N2 patients, number in table = number of involved lymph node stations, number in parenthesis in table: number of lymph node stations with skip involvement
In the right upper lobe, the most commonly involved station was the lower paratracheal node in all three segments. In the right middle lobe, the subcarinal node was the most common, and the lower paratracheal node was the next most commonly involved station in both the lateral and medial segments. In the right lower lobe, the most commonly involved station was the subcarinal node in the superior, anterior basal, lateral basal, and posterior basal segments, and was the pulmonary ligament node in the medial basal segment.
In the left upper lobe, the subaortic node was the most commonly involved in all four segments, and the subcarinal node was also equally involved in the inferior lingular segment. In the left lower lobe, the most commonly involved station was the subcarinal node in the superior segment, the pulmonary ligament node in the anterior basal, lateral basal, and posterior basal segments was commonly affected.
In the segments in which skip involvement was common, the most commonly involved mediastinal station was the right lower paratracheal node in the right apical and posterior segments, the right pulmonary ligament node in the right medial basal segment, the subaortic node in the left apical posterior segment, and the left pulmonary ligament node in the left lateral basal and posterior basal segments (Fig. 3).

Specific patterns of skip involvement from pulmonary segments. In the segments in which skip involvement was common, the most commonly involved mediastinal station was the right lower paratracheal node in the right apical and posterior segments, the right pulmonary ligament node in the right medial basal segment, the subaortic node in the left apical posterior segment, and the left pulmonary ligament node in the left lateral basal and posterior basal segments
Discussion
Many authors have analyzed the prognostic factors in resected N2 NSCLCs with a particular focus on the distribution of mediastinal node metastases to disclose the specific drainage patterns from each pulmonary lobe to target mediastinal nodes, but the patterns still remain to be clarified (2–17). In contrast, our current results disclosed the lymphatic drainage pattern of each pulmonary segment and lobe to the mediastinum based on the infectious process, which may facilitate the understanding of nodal metastatic patterns in NSCLCs.
Our observations on CT images of pulmonary histoplasmosis have several unique advantages in the assessment of pulmonary lymphatic drainage to the mediasinum. First, in histoplasmosis with mediastinal nodal disease, the number of involved nodal stations was limited: single in 70% of cases, and 1.4 stations on average. This generally self-limited infectious disease is considered to be suitable for the assessment of the initially involved mediastinal node from each pulmonary segment or lobe. Second, due to the small size of calcified pulmonary lesions in histoplasmosis (within a few mm in diameter), we can precisely determine the involved pulmonary segment on CT images, whereas this is occasionally difficult in NSCLCs due to their large size and extensive invasion. Third, in NSCLCs, the assessment of the distribution of mediastinal node metastases may be limited, depending on the extent of preoperative sampling or dissection in thoracotomy of mediastinal nodes. In contrast, in our studies with histoplasmosis, we could entirely evaluate the distribution of involved mediastinal nodes using thin slice CT images of the whole thorax.
In our previous study on 400 patients with pulmonary histoplasmosis consisting of mediastinal node involvement and pulmonary lesions within a single lobe, including multisegmental lesions (18), we assessed the lymphatic drainage pattern to the mediastinum from each lobe but could not disclose segment specific lymphatic drainage pattern. To assess the lymphatic drainage pattern to the mediastinum depending on each pulmonary segment, we collected the CT studies of patients with primary complex of histoplasmosis with solitary pulmonary lesion and hilar and/or mediastinal node involvement in the current study.
In our observations, the lymphatic drainage of an each pulmonary lobe can be summarized as follows: the right upper lobe mainly drains into the right lower paratracheal node, and skip involvement of this station is common, especially from the apical and posterior segments. The middle lobe drains bidirectionally into the subcarinal and right lower paratracheal nodes, mainly via the hilar node. The lower lobe has a more complex pattern, involving the subcarinal node, the pulmonary ligament node, the paraesophageal node, and less commonly, the right lower paratracheal node. Drainage into the pulmonary ligament and paraesophageal node is especially common from the medial basal segment, with frequent skip involvement. The left upper lobe tends to drain into the subaortic node and less frequently to the subcarinal node. Skip involvement is common to the subaortic node, mainly from the apical posterior segment. The left lower lobe commonly drains into the pulmonary ligament, subcarinal, and paraesophageal nodes. Skip involvement is common in the pulmonary ligament node, especially from the posterior basal segment. Our data are similar to the previously reported lobe-specific preferentially involved mediastinal nodes observed during the assessment of resected N2 NSCLCs (2–4, 13–17).
The incidence of skip N2 metastases in previously reported studies was 5–10% in all NSCLC patients, and 20–40% of pN2 patients (5–10). Several studies have suggested a more favorable prognosis for skip N2 metastases than non-skip N2 metastases (5-10). Skip metastases in lung cancers have been suspected to occur owing to overlooked small metastatic foci in the hilar and/or intrapulmonary nodes, a direct lymphatic pathway to the mediastinum, or some biological factors involving the tumor cells, such as their proliferative potential (20, 21).
Using immunohistochemical staining for cytokeratin, a previous study assessed the micrometastases in the N1 lymph node of skip N2 disease, and indicated that the microscopic spread of cancer cells could be detected in only 17.6% of patients with skip N2 disease (20). Another study assessed micrometastases in lymph node samples obtained from 181 NSCLCs patients diagnosed with N0 disease by conventional histopathological examination. They stated that nodal micrometastases were found in a single level mediastinal node station in 26 patients consisting of 19 with the skip pattern and seven with a non-skip pattern (22). These results suggest that skip metastasis was also found in micrometastatic disease, and that overlooked micrometastases in the N1 node is not the main mechanism of skip N2 disease.
Our data showed that skip involvement also occurs in pulmonary infections in the lobe-specific preferential stations of the mediastinal node, and these patterns and incidences are similar to those observed in lung cancer cases. These results suggest that the biological behavior of tumor cells cannot thoroughly account for skip metastasis in NSCLCs.
In our study, the incidence of skip involvement differed depending on the segment affected within a lobe, and showed an inverse correlation with that of N1 involvement in the same segments, suggesting that anatomical direct lymphatic drainage to the mediastinum contributes to skip metastases from the lung. In an autopsy study of 260 patients, a 20–40% incidence of segmental lymph channels draining directly into mediastinal lymph nodes was reported (23). This incidence is similar to that of skip metastases reported in the literature (5–10). Sasaki et al. suggested that septal structures between the pulmonary veins and mediastinum, which are occasionally seen on high-resolution CT images of normal subjects and those of pneumothorax patients, might be a direct communication between the upper lobe and the mediastinum, and may provide a pathway for skip involvement (24).
In our study, the patients with skip involvement had a smaller number of involved mediastinal lymph node stations than did the non-skip patients (1.2 vs. 1.4, P < 0.01). This finding was concordant with the studies in NSCLC cases. Skip-positive patients had a smaller number of tumor-infiltrated mediastinal lymph nodes per patient than did skip-negative patients, and this finding could offer a possible explanation for the more favorable prognosis of patients with NSCLC who have skip metastases (5, 7, 8, 20). Therefore, skip metastases could represent early stage mediastinal node involvement via direct lymphatic drainage. We think that patients with NSCLC who have skip N2 disease, the right paratracheal node metastasis from the right upper lobe lesion; subaortic node metastasis from the left upper lobe; and pulmonary ligament node metastasis from lower lobe, should be considered as minimal N2 disease and would benefit from surgery.
There are some limitations to our study. First, the diagnosis of histoplasmosis was made clinically, and lacked a definitive diagnosis based on culture or histological studies. Although its lymphatic drainage pattern is nearly the same with histoplasmosis, there could be some cases with primary complex of tuberculosis in our study. Second, although the involved lymph nodes usually reveal calcification in patients with resolved pulmonary histoplasmosis, and we assessed the presence of calcifications on thin slice 3-mm CT images, we cannot conclusively state that only those lymph nodes that are calcified are those that drained the specific region of the lung.
In conclusion, observation of CT images of primary complex pulmonary histoplasmosis consisting of segmental lesions within the lung and associated nodal disease disclosed the lobe-specific preferentially involved lymph node station(s) in the mediastinum. These findings are similar to those in previously reported studies on nodal metastases in NSCLCs, and suggest skip metastases would represent early stage mediastinal node involvement via direct lymphatic drainage.