
Abstract
Background
Unexpected focal 18F-FDG breast uptakes are occasionally identified on PET/CT due to its increased use for cancer staging and follow-up. The need for their characterization has been suggested.
Purpose
To retrospectively evaluate the diagnostic value of ultrasonography (US) in distinguishing benign from malignant lesions for unexpected focal 18F-FDG uptakes in breast on PET/CT scans.
Material and Methods
Between April 2004 and January 2010, 27 focal 18F-FDG breast uptakes in 27 patients (age range 33–62 years; mean age 46 years) among 5214 patients who had undergone PET/CT scans were retrospectively analyzed. The American College of Radiology (ACR) Breast Imaging-Reporting and Data System (BI-RADS) final assessment categories of the US and the maximum standardized uptake values (SUVs) of the lesions were compared between the benign and malignant lesions.
Results
Of the 27 lesions, 15 (56%) lesions were malignant. The rate of malignancy, according to the final assessment category on the US, was 0% (0 of 6) for category 3, 60% for category 4 (9 of 15), and 100% (6 of 6) for category 5 (P = 0.001). The US evaluation revealed a sensitivity of 100% (15 of 15) and a specificity of 50% (6 of 12). The average maximum SUV of the malignant lesions was greater than that of the benign lesions (4.12 ± 1.94 vs. 1.94 ± 0.82; P = 0.001).
Conclusion
US evaluation of unexpected focal 18F-FDG uptakes on PET/CT scans can accurately distinguish benign lesions from malignant lesions.
As positron emission tomography with 18F-flourodeoxyglucose/computed tomography (18F-FDG-PET/CT) scan has gained increasing popularity for the evaluation of patients with malignant disease and for the screening of healthy subjects (1), unexpected focal 18F-FDG uptakes have also been increasingly identified using PET/CT scans. According to one previous study, the detection rate of unexpected additional primary malignancies using PET/CT scans was 1.2% (22 of 1912 patients) for new primary malignant sites in the lung (n = 7), thyroid (n = 6), colon (n = 4), and breast (n = 2) (2). There have been numerous reports in the literature regarding unexpected thyroid uptakes with malignancy rates ranging from 14–47% (3–8); however, there have been relatively few reports regarding breast 18F-FDG uptakes. One recent study reported that 0.4% (163) of 45,000 PET/CT scans exhibited unexpected focal 18F-FDG breast uptakes; of which 29% (7 of 24 confirmed cases) were found to be malignant (9). Although one earlier study suggested that unexpected 18F-FDG breast uptakes often indicated malignancy, with an 83% (5 of 6) malignancy rate (10), 18F-FDG uptakes have also been observed in various benign diseases, such as a fibrocystic change, fibroadenoma (11, 12), physiologic change, or lactation in the breast (13). The ability to further characterize these uptakes would be valuable for the field.
In one study, ultrasonography (US) was shown to have a high level of accuracy for the characterization of thyroid incidentalomas on 18F-FDG PET/CT scans (14). However, to the best of our knowledge, there have been no studies regarding the US evaluation of unexpected focal breast 18F-FDG uptakes.
Our institution has routinely performed breast US for the evaluation of unexpected focal 18F-FDG breast uptakes on PET/CT scans. The aim of this study was to retrospectively evaluate the diagnostic value of US in distinguishing benign masses from malignant unexpected focal 18F-FDG breast uptakes on PET/CT scans.
Material and Methods
Database search
The institutional review board of our institution approved the present study, and the requirement of informed consent was waived for this retrospective analysis. A retrospective search of the PET/CT scan database and the medical records of our institution identified 5214 consecutive patients who underwent a PET/CT scan between April 2004 and January 2010; of which 2% (106 of 5214) underwent breast US due to the presence of an unexpected focal 18F-FDG uptake in the breast. An unexpected focal 18F-FDG uptake in the breast was defined as a focally increased 18F-FDG accumulation in the breast of the woman without history of breast cancer, as measured by standardized uptake values (SUVs). Lesions with a mildly increased diffuse uptake and without SUV measurements (n = 9) were excluded from the present study. Of the 97 patients, 70 were excluded because they were found to have a known history of breast cancer. Finally, a total of 27 lesions in 27 patients (age range 33–62 years; mean age 46 years; 26 women and 1 man) were included in the present study (Table 1). A PET/CT scan was used to stage the known primary malignancies in 83% (23 of 27) of the participants and was used for cancer screenings in the healthy subjects in 15% (4 of 27) of the participants. The primary malignancies were lung cancer (n = 4), thyroid cancer (n = 4), lymphoma (n = 3), endometrial cancer (n = 2), colon cancer (n = 2), malignant meningioma (n = 2), vaginal cancer (n = 1), cervical cancer (n = 1), advanced gastric cancer (n = 1), eyelid cancer (n = 1), rectal cancer (n = 1), and gallbladder cancer (n = 1).
Patient age, mammographic findings, and sonographic findings of the focal FDG-uptake breast lesions
*Two lesions of asymmetric parenchyma were not included in the analyses
†The lesion size was determined as maximal diameter on US
The data are numbers of lesions; the numbers in parentheses are percentages
PET/CT scans and interpretation
Prior to the intravenous administration of the 18F-FDG (5.2 MBq/kg of bodyweight), the patients were instructed to fast for at least 4 h to ensure a serum glucose level of below 7.8 mmol/L. At 1 h after the intravenous administration of the 18F-FDG, images from the base of the skull to the proximal thigh were acquired using a PET/CT scanner (Biograph, Siemens Medical Solutions, Hoffmann Estates, IL, USA; or Allegro, Philips Medical Systems, Cleveland, OH, USA) in 3D mode. The acquired images were then reconstructed using an iterative reconstruction algorithm. Specifically, the ordered-subset expectation maximization (OSEM) algorithm for the Siemens PET/CT scanner or the low-action maximal likelihood algorithm (RAMLA) for the Philips PET/CT scanner was used. Two experienced nuclear medicine physicians visually evaluated all of the acquired 18F-FDG-PET/CT scan images on a high-resolution monitor. For the quantitative analysis of 18F-FDG uptake, a region of interest (ROI) was placed over the most intense area of 18F-FDG accumulation for each patient, and the standardized uptake value (SUV) was calculated as follows: SUV = region's radioactivity concentration (Bq/ml)/injected dose (Bq)/patient's weight (g). The maximum standardized uptake value (SUV), which was defined as the peak SUV on the pixel with the highest count within a ROI, was measured and recorded for the focal areas of uptake in the scan.
Imaging evaluation
The mammograms, US, and their radiologic reports of the patients were retrieved from the picture archiving and communication system (PACS). All of the focal 18F-FDG uptakes in the breast were evaluated by one of seven radiologists, all of whom had between 3 and 15 years of experience in breast imaging. All images were subsequently reviewed by consensus. Mammography was performed using the Senographe 2000D (GE Healthcare, Milwaukee, WI, USA) or the LORAD Selenia digital mammography machine (Hologic, Inc., Bedford, MA, USA) for 25 of the 27 patients. Two patients who were under 30 years old did not undergo mammography because they refused the exam of their own will. US was performed using a 6- to 14-MHz linear array transducer (EUB-8500 scanner, Hitachi Medical, Tokyo, Japan), a 5- to 12-MHz linear array transducer (iU 22, Philips Medical System, Bothell, WA, USA) in all 27 patients. The mammographic findings were negative in 10 of the cases, masses were found in 14 cases, and a mass with microcalcifications was identified in one case. During US evaluations, the mammographic findings were correlated and focal uptakes on 18F-FDG-PET/CT scans were searched based on the information of the lesion size, depth, and location. All 27 focal FDG uptakes on PET/CT scans were identified as focal lesions on US. American College of Radiology (ACR) Breast Imaging-Reporting and Data System (BI-RADS) final assessment category was prospectively determined based on the most suspicious findings, either mammography or US, and it was recorded on PACS (15). The lesion size was determined as the maximal diameter on US. The imaging features of the lesions were recorded, including the shape, orientation, margin, boundary, echo pattern, posterior acoustic features, surrounding tissue, and calcifications (Table 1). An assignment of category 3 indicated that the finding was probably benign, with a probability of malignancy of less than 2%; category 4 indicated a suspicion of malignancy, with a probability of malignancy of 3–94%; and category 5 indicated that the finding was highly suggestive of malignancy, with a probability of malignancy of greater than 95%. The subcategories of category 4 were defined according to their probability of malignancy; 3–10% for 4a (a low level of suspicion), 11–50% for 4b (an intermediate level of suspicion) and 51–94% for 4c (a moderate level of suspicion).
Histologic evaluation
Surgical excision and core biopsy specimens were evaluated by one pathologist with 25 years of experience in breast pathology. Characterization of all of the lesions that were observed using US was confirmed using an US-guided, automated gun biopsy using a 14-gauge needle (Acecut, TSK Laboratory, Japan or Pro-Mag2.2, Manan Medical Products, Wheeling, IL, USA) (n = 23) or a subsequent surgical excision (n = 10), which was performed for all of the lesions with an invasive ductal carcinoma or ductal carcinoma in situ. In one patient with an atypical papilloma that was diagnosed using an automated gun biopsy, a surgical excision was performed, and the lesion was confirmed as a ductal carcinoma in situ. Two patients with secondary breast lymphomas underwent chemotherapy without surgery. Three patients with infiltrating ductal carcinomas did not undergo surgical excision; two of these patients refused surgery due to stage IV primary malignancy, and one of these patients was referred to another hospital due to the patient's preference. The mean interval between the 18F-FDG PET/CT scan and the core biopsy was 15.5 days (range 1–145 days). Of the six patients with category 3 lesions, two patients underwent an automated gun biopsy because the patients wanted histologic confirmation of the lesions. The remaining four patients with category 3 lesions underwent follow-up visits for at least 12 months and then the stability of the lesion confirmed. Ten patients with surgically confirmed malignant lesions underwent follow-up visits for 35.2 ± 17.2 months, and there were no patients with metastasis or recurrence.
Statistical analysis
To evaluate the performance of the US in distinguishing the benign from the malignant FDG uptakes, the rates of malignancy, according to the final assessment category and the mean of maximum SUV, were compared between the two groups using a Fisher's exact test and an independent samples t-test, respectively. The sensitivity and specificity of the final assessment category on the US and the sensitivity and specificity of the maximum SUV were calculated. The area under the curve (Az) of a receiver-operating characteristic (ROC) curve of the maximum SUV was also calculated. The statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS version 17.0 for Windows, Chicago, IL, USA). P values of less than 0.05 were considered to indicate significant differences between groups.
Results
Of the 27 lesions of the focal FDG uptakes, 12 (44%) lesions were benign, and 15 (56%) lesions were malignant. The benign lesions that were confirmed using a needle biopsy were of the following types: fibrocystic change (n = 4), fibroadenoma (n = 2), papilloma (n = 1), and gynecomastia (n = 1) (Fig. 1). The benign lesions that were confirmed by a follow-up of at least 12 months were the following: an asymmetric parenchyma (n = 2), a cyst (n = 1), and a foreign body granuloma (n = 1). The malignant lesions included an infiltrating ductal carcinoma (n = 10), a ductal carcinoma in situ (n = 3), and a lymphoma (n = 2) (Fig. 2). The mean lesion size that was measured using US was 14 mm (range 3–26 mm).
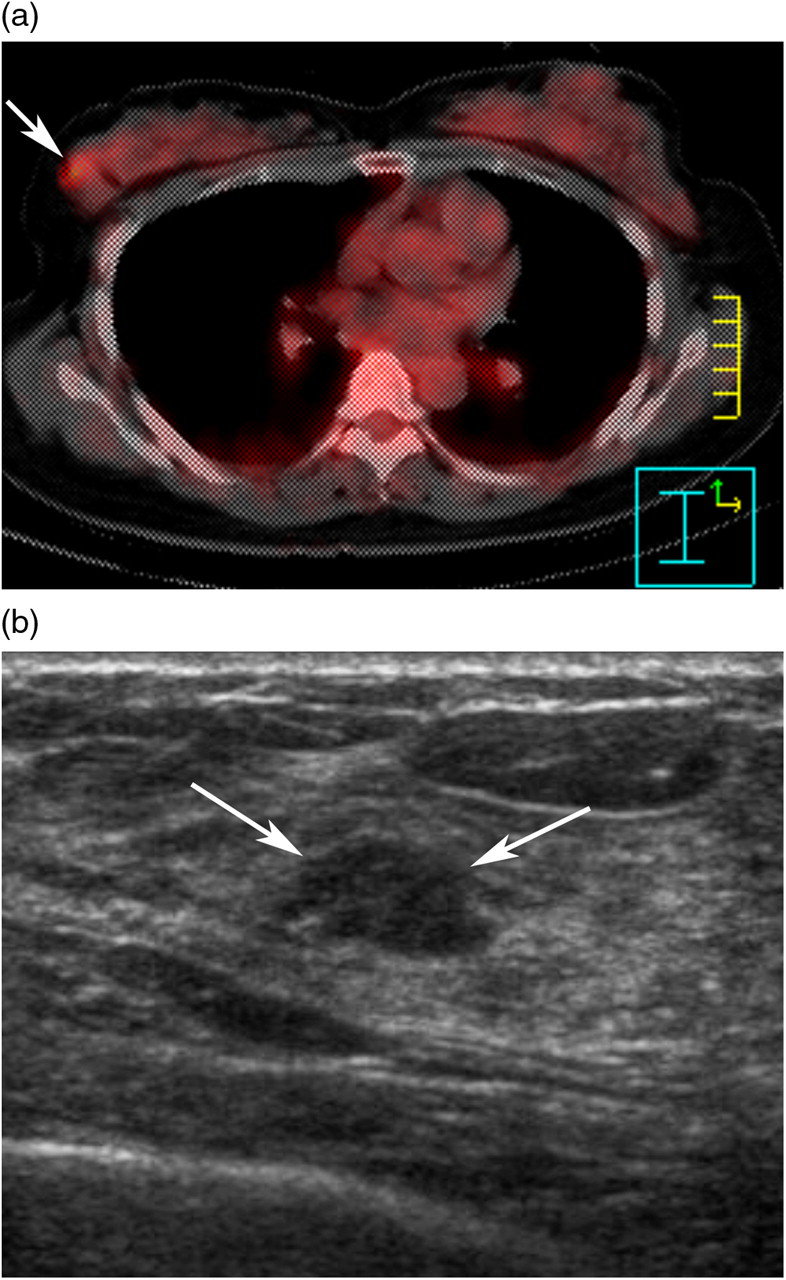
Fibroadenoma in a 51-year-old woman. (a) An axial 18F-FDG PET/CT scan shows a focal radiotracer uptake (arrow) in the right breast, and its SUVmax was calculated as 3.3; (b) A transverse ultrasonography image shows an oval hypoechoic mass with a circumscribed margin in the corresponding area (arrows), which was classified as BI-RADS category 4a. The mass was determined to be a fibroadenoma using an US-guided core needle biopsy
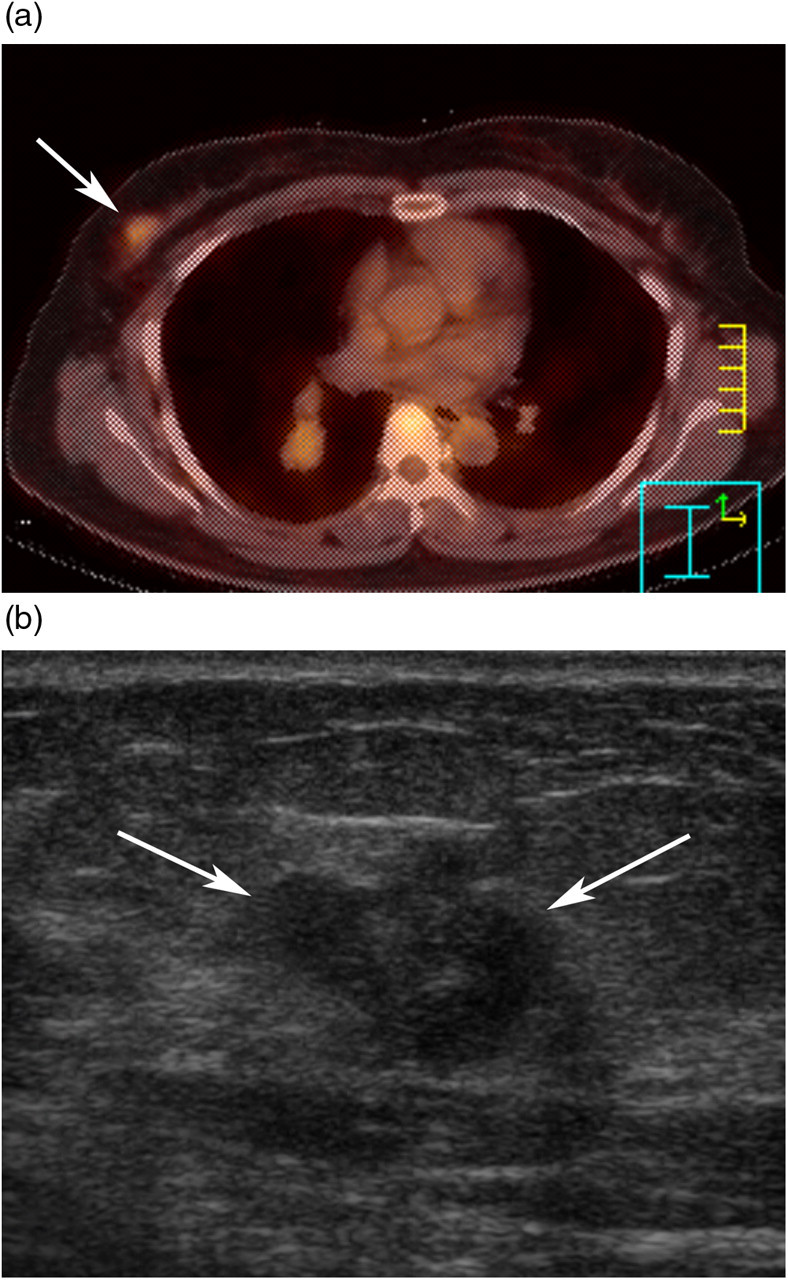
Infiltrating ductal carcinoma in a 50-year-old woman. (a) An axial 18F-FDG PET/CT scan shows a focal radiotracer uptake (arrow) in the right breast, and its SUVmax was calculated as 2.3. (b) A transverse ultrasonography image shows an irregular hypoechoic mass with an angular margin in the corresponding area (arrows), which was classified as BI-RADS category 5. This mass was determined to be an infiltrating ductal carcinoma using an US-guided core needle biopsy
The rate of malignancy, according to the lesions' final assessment categories, was 0% (0 of 6) for category 3, 60.0% (9 of 15) for category 4 and 100% (6 of 6) for category 5 lesions (P = 0.001, Fischer's exact test) (Table 2). As for the subcategories of category 4, the rate of malignancy was 29% (2 of 7) for category 4a, 50% (1 of 2) for category 4b and 100% (6 of 6) for category 4c lesions. When the category 4 and 5 lesions were defined as positive, the US category exhibited 100% (15 of 15) sensitivity and 50% (6 of 12) specificity.
Histopathologic diagnosis according to the final assessment category on sonography for 27 focal 18F-FDG uptake breast lesions
*The final diagnosis was based on a follow-up period of more than 1 year
The average maximum SUV of the malignant lesions was greater than that of the benign lesions (4.12 ± 1.94 vs. 1.94 ± 0.82; P = 0.001, independent samples t-test) (Fig. 3). When the optimal cut-off value for the maximum SUV of 2.2 was used, which was defined as the maximal sum of the sensitivity and specificity, the maximum SUV exhibited 93.3% (14 of 15) sensitivity and 75.0% (9 of 12) specificity. The one false-negative case was an infiltrating ductal carcinoma, with a maximum SUV of 1.9. The final assessment category for the case was 4c. The area under the ROC curve (Az) of the maximum SUV was 0.914 (95% confidence interval, 0.742–0.987) (Fig. 4).
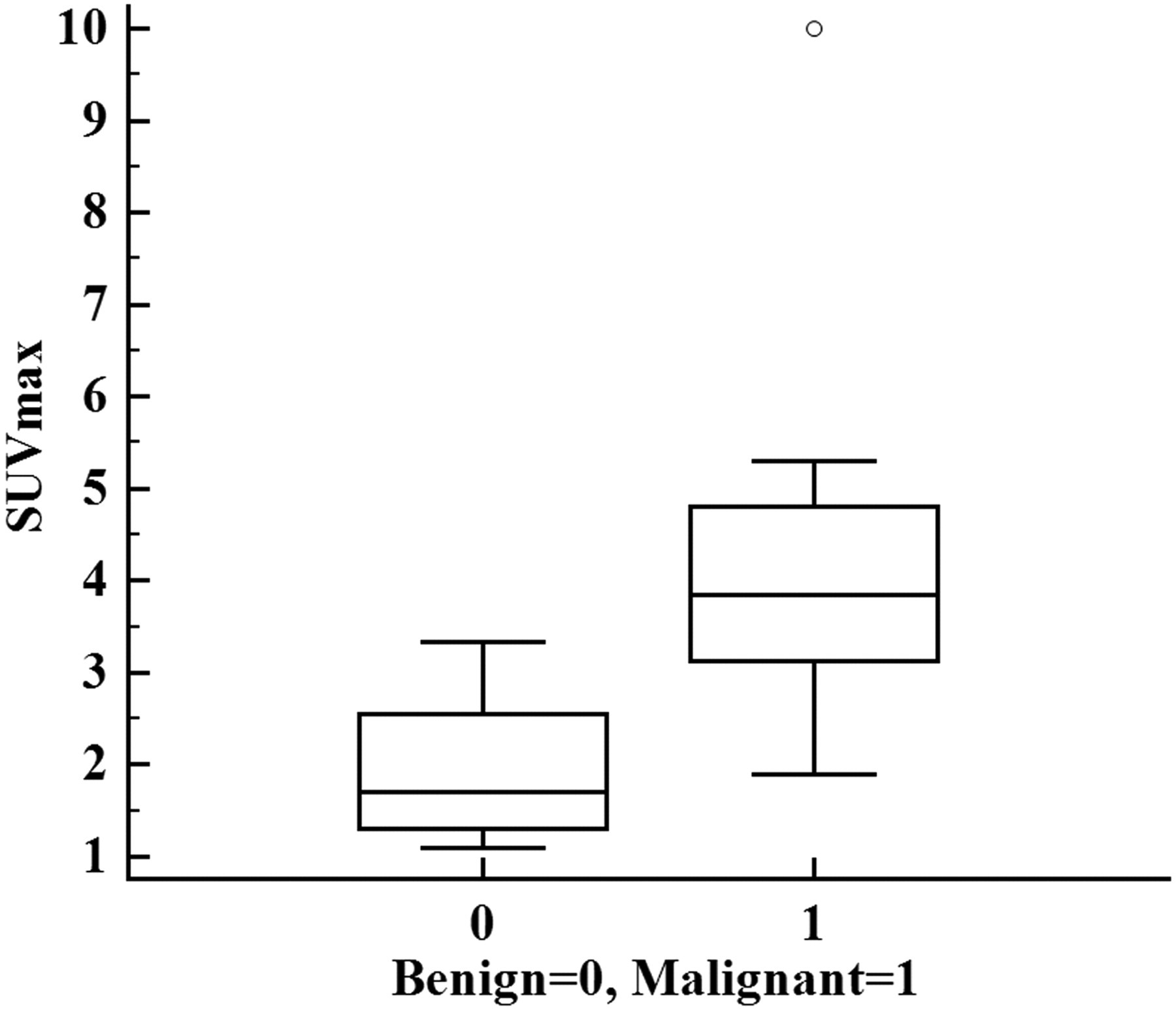
Box plot of maximum standardized uptake value (SUVmax) for benign and malignant focal 18F-FDG uptakes on PET/CT. The top and bottom of each box represent the 25th and 7th percentiles of maximum SUV, respectively. The horizontal line inside of each box represents the median value. The median value of the malignant lesions (3.84) is higher than that of the benign lesions (1.7). The outlier (º) was a case of invasive ductal carcinoma with a SUVmax of 10
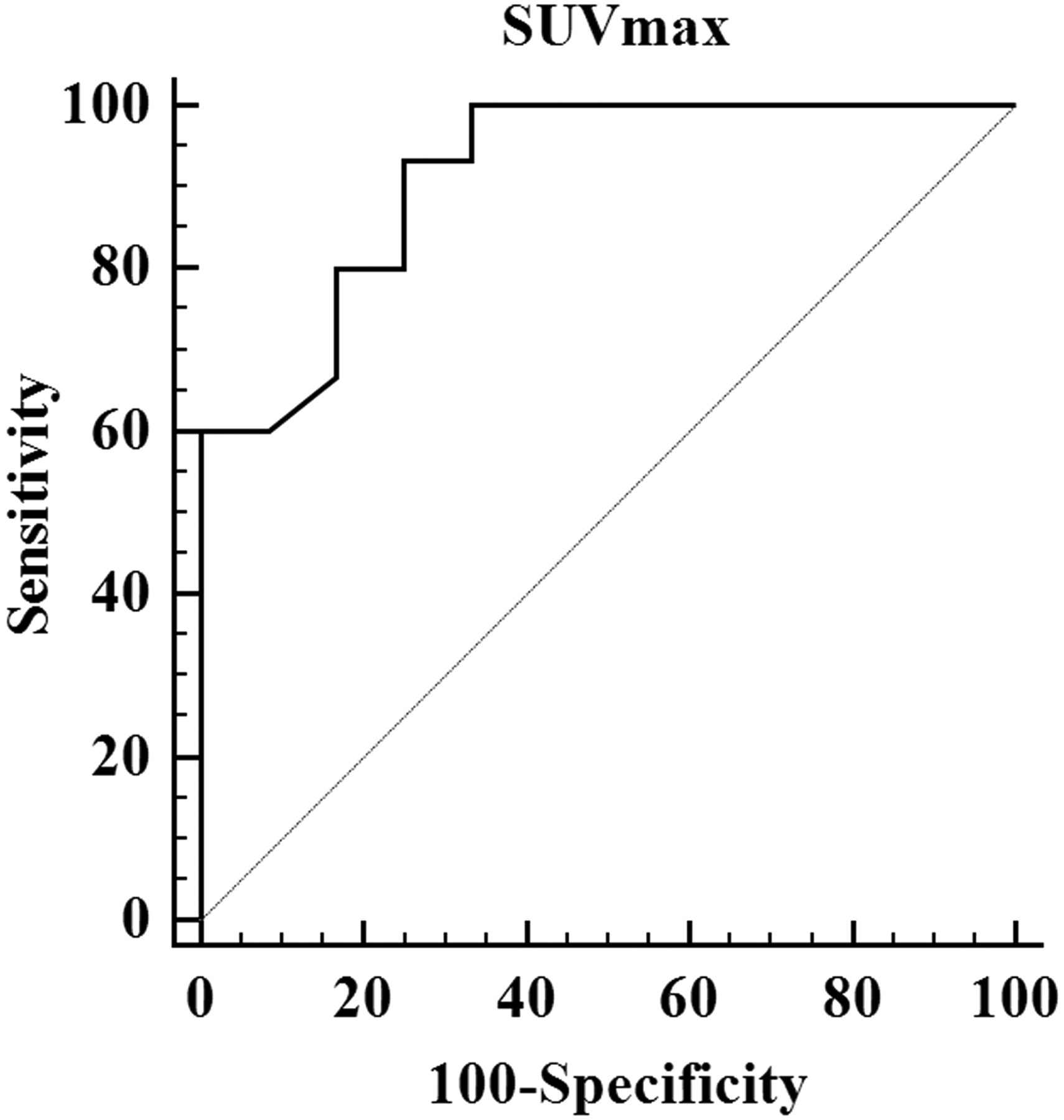
Receiver-operating characteristic curve of maximum standardized uptake value (SUVmax) to distinguish benign from malignant focal 18F- FDG uptakes in the breast on PET/CT. The area under the curve was 0.914
Discussion
In the present study, the malignancy rate of the unexpected focal 18F-FDG breast uptakes was 56%, and the US evaluation was accurate in distinguishing benign from malignant unexpected breast uptakes that were detected using PET/CT scans. When the lesion showed higher final assessment category, the probability of malignancy was much higher. Notably, we achieved 100% (15 of 15) sensitivity and 50% (6 of 12) specificity, which is consistent with the results of a previous study that reported greater percentages of (98.4%, 123 of 125) sensitivity and moderate (67.8%, 424 of 625) specificity of the breast US for distinguishing benign from malignant disease (16). Our results suggest that US evaluation can be useful in distinguishing benign from malignant focal FDG uptakes using PET/CT scan. In addition, a focal breast lesion showing low SUV may be biopsied if the lesion appears suspicious on US. Indeed, one false-negative case based on SUV of 1.9 on PET/CT scans was classified as category 4c on US. In other cases of cyst or foreign body granuloma, although a benign lesion such as a cyst showed increased FDG uptake with SUV of 1.6, they appeared with benign features on US and were confirmed as benign. This result is consistent with benign non-physiologic lesions including a cyst with increased FDG uptake in a previous report (17).
Another important point of our study was the establishment of US as a biopsy guidance modality for lesions that are depicted using PET/CT scans. Although the feasibility of positron emission mammography-guided biopsy has been recently reported, this method is not yet routinely available in clinical practice (18). However, because of the high level of correlation of the anatomic location and shape of the lesions between high-resolution US and PET/CT scans, an accurate localization of focal FDG uptakes in the breast can be obtained, allowing tissue confirmation. Therefore, for the evaluation of incidental 18F-FDG uptakes in the breast, US can be performed with confidence.
In one previous report, the use of PET/CT scans at follow-up was suggested when the focal 18F-FDG breast uptakes were not identified using mammography. The authors reported that 40% (16 of 40) of the lesions that exhibited 18F-FDG uptake disappeared on the follow-up PET/CT scan due to the variable nature of the 18F-FDG uptake in the breast depending on age, breast density, and menstrual cycle (9). However, with such management, curable malignancy may be delayed with adverse consequences. So, we recommend immediate US evaluation of unexpected focal FDG uptakes for early diagnosis of cancer. In our study, of the 15 patients with malignancy, 10 patients were found to have curable breast cancer, including three lesions of DCIS.
With regard to the maximum SUV, which quantifies the 18F-FDG uptakes, lesions with higher maximum SUVs also tended to have higher malignancy risks. The area under the ROC curve of the maximum SUV was 0.914, the sensitivity was 93.3% (14 of 15), and the specificity was 75% (9 of 12) when the maximum SUV of 2.2 was used as a cut-off value. These results are consistent with other studies that showed that a SUV of 2.0–2.5 was the accepted cut-off value for distinguishing benign from malignant lesions (19, 20). Other studies have also reported a sensitivity of the 18F- FDG PET/CT scans that ranged from 80% to 96% and a specificity that ranged from 83% to 100% for detecting primary breast cancer and staging (16, 21).
Our study has several limitations. First, we only included focal 18F- FDG uptakes that had been evaluated by US. The relatively greater malignancy rate of 56% in our study than the rates in a previous study may be related to the inclusion criteria (9). Although patients with a focal 18F- FDG breast uptake that is identified using PET/CT scans are routinely examined using breast US in our institution, lesions with a lower likelihood of malignancy would not have undergone US and thus, were not included in the present study. Second, although the lesions that were identified using US and using PET/CT scans were determined to be correlated in terms of their size, morphology, location, and temporal stability during the follow-up, the possibility for discrepancies still remains. Third, although mammography was negative in 40% of the patients, the role of mammography evaluation for unexpected focal 18F-FDG uptake was not separately evaluated, as the final assessment category was determined based on the combined mammography and US findings.
In conclusion, the maximum SUV is useful in distinguishing benign from malignant unexpected focal 18F-FDG uptake lesion. In addition, US is also helpful in distinguishing benign from malignant unexpected focal 18F-FDG uptake lesion So, an US-guided core biopsy may be used for the histologic confirmation of focal 18F-FDG uptakes in the breast on PET/CT scans.