
Abstract
Background
Renal involvement in patients with lymphoproliferative disease is an uncommon radiological finding.
Purpose
To determine its prevalence and radiological appearances in a patient population.
Material and Methods
All forms of lymphoproliferative disease (ICD: C81–C96) were considered. From January 2005 to January 2010, 668 consecutive patients with lymphoproliferative disease were identified with the help of the radiological database and patient records. Inclusion criteria were complete staging including appropriate CT scan and/or MRI. All stored images (initial staging and follow-up examinations) were reviewed.
Results
Review of all stored images revealed renal infiltration in patients with non-Hodgkin lymphoma (11 of 364 = 3.0%; median age = 65 years, m:f = 6:5) but also multiple myeloma (2 of 162 = 1.2%; median age = 72 years; m:f = 1:1) and leukemia (5 of 101 = 4.9%; median age = 12 years; m:f = 2:3). There were no cases of renal infiltration in 41 patients with Hodgkin's disease. In total there were six patients with solitary lesions, five patients with diffuse renal enlargement, four patients with perirenal lesions, and two patients with direct invasion of the kidney.
Conclusion
In leukemia the most common imaging pattern is diffuse enlargement. In the other subtypes of lymphoproliferative disease no specific correlation between typical CT patterns and subtype of lymphoproliferative disease can be found. The prevalence of renal involvement is in line with earlier studies. Contrary to earlier reports, multiple lesions were not found to be a common pattern.
In staging examinations of patients with lymphoproliferative disease, regardless of whether initial or follow-up, it is important to remember that the kidney might be involved. Extralymphatic organ involvement is considered Ann-Arbor stage 4. Therefore, renal involvement might have a significant impact on staging and therapy.
Although renal involvement is a common finding in autopsy of patients with advanced non-Hodgkin lymphoma (NHL) (1) and other lymphoproliferative diseases, it is much rarer found in radiological examinations. As the genitourinary system does not contain lymphoid tissue, the involvement is secondary in almost all cases (1–3).
Most publications regarding renal involvement in lymphoproliferative diseases are isolated case reports. There were only few studies concerning the prevalence and histology of renal infiltration in NHL (4–8). Renal involvement in Hodgkin's disease (4), multiple myeloma (9), and leukemia (10) is even rarer documented. There are excellent descriptions about radiological imaging patterns of renal involvement (3, 11). However, these picture reviews do not include self-acquired data about the prevalence of certain patterns in certain subtypes of disease.
The purpose of the present study was to estimate the prevalence of renal involvement in radiological examinations of patients with malignant lymphoproliferative diseases and to determine its radiological patterns in a consecutive patient group.
Material and Methods
This retrospective study was accepted by the institutional review board.
Between January 2005 and January 2010, 668 patients with lymphoproliferative disease (ICD: C81–C96) were treated at our institution. The population was divided into 364 patients (m:f = 203:161) with NHL including five patients with malignant immunoproliferative diseases (C88), 41 patients (m:f = 23:18) with Hodgkin's disease, 162 patients (m:f = 103:59) with multiple myeloma, and 101 patients (m:f = 56:45) with leukemia. Patients were identified by retrospective analysis of patient records. Only those patients who underwent complete initial staging work-up consisting of thorough clinical examination, complete hematological examination, renal functional evaluation, bone marrow examination, radiological imaging including appropriate CT scan, and/or MRI were included in the study. Most patients had additional staging examinations in the course of their disease. Respective CT and MRI scans were also reviewed to detect renal involvement in follow-up state.
The updated REAL/WHO classification (12) as well as the 10th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) was used in cellular stratification of the disease.
The stored images of 668 patients were reviewed by two radiologists (AGB, AS) to identify patients with renal involvement.
In 102 patients suspicious renal lesions were detected. In detail there were simple cysts (49 patients), complicated cysts (3 patients), atrophic kidneys and pathologies of the pelvicocaliceal system (18 patients), renal involvement in lymphoproliferative disease (17 patients), renal cell carcinoma (5 patients), metastatic involvement of prostate carcinoma (2 patients) and Ewing's sarcoma (1 patient), abscess (2 patients), hematoma (2 patients), and oncocytoma (1 patient). Lesions without histopathological confirmation that showed no response to therapy (2 patients) were excluded.
All available histological materials (sections stained by hematoxylin/eosin or by immunohistochemistry) were analyzed by two pathologists.
Contrast-enhanced CT (Somatom Sensation 64; Siemens, Erlangen, Germany) was performed in 13 patients. Sixty to 140 mL of an iodinated intravenous contrast medium were given at a rate of 1.5–3.5 mL/s in all cases. Typical imaging parameters were 120 kVp, 150–300 mAs, and 0.6- to 6-mm slice thickness with a pitch of 0.6–1.2.
In two patients MRI was additionally performed. In four patients only MRI was performed. The MRI studies were done using a 1.5T MRI scanner (Magnetom Vision Sonata Upgrade; Siemens, Erlangen, Germany). The protocol included a T2 turbo spin-echo sequence (repetition/echo time [TR/TE] 5000/130 ms, 4-mm slice thickness) and a T1 spin-echo sequence (TR/TE 500/14 ms, 4-mm slice thickness), prior to and after intravenous administration of contrast medium (gadopentate dimeglumine, Magnevist; Bayer Schering Pharma, Berlin, Germany; and gadodiamide, Omniscan; GE Healthcare, Oslo, Norway) at 0.1 mL/kg body weight.
In both CT and MR imaging no intravenous contrast medium was given in patients with renal failure (n = 5).
Collected data were evaluated by means of descriptive statistics (absolute and relative frequencies).
Results
Renal involvement was found in 17 patients (Table 1): eight women and nine men, with an age range from 1–81 years (median age 63 years). In all of them involvement was already present at the initial staging examination. The diagnosis was confirmed histopathologically in 11 cases (by renal biopsy in 5, and after nephrectomy in 6 cases). In the other six patients, widely disseminated disease was confirmed by typical radiological imaging findings and further by biopsy of lymph nodes or bone marrow. Additionally, the response of the renal lesions to chemotherapy was considered confirmatory.
Characteristics of patients with renal involvement in malignant lymphoproliferative disease
*One patient showed renal invasion of both NHL and leukemia
†Tumor other than lymphoma in patients with microscopical infiltration with lymphoma
‡At time of first imaging
RB = renal biopsy, NC = nephrectomy
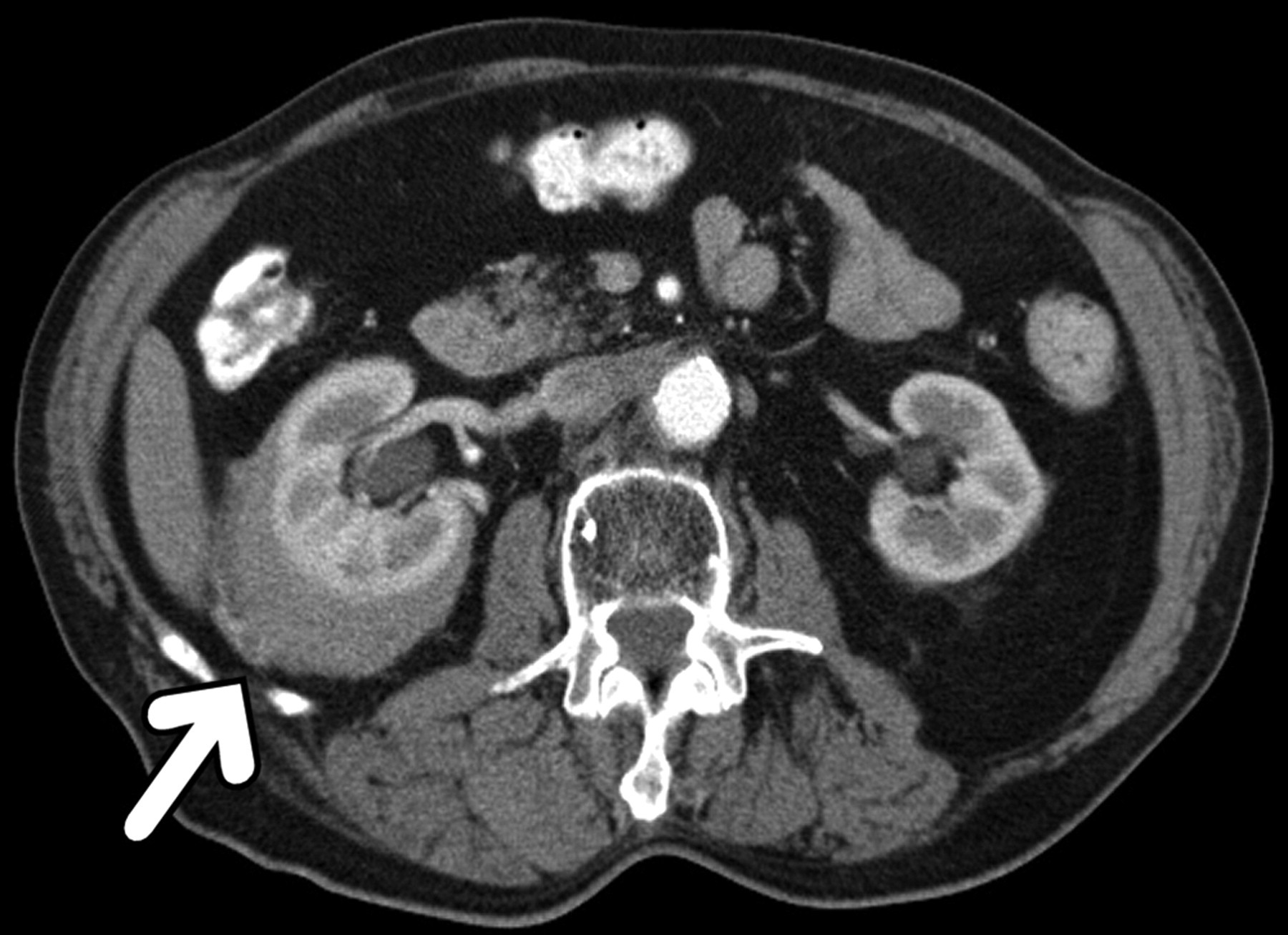
Identified radiological imaging patterns include solitary lesions (Fig. 1), perirenal lesions with signs of capsular infiltration (Fig. 2), direct invasion of the kidney via retroperitoneal lymph nodes (Fig. 3), and diffuse enlargement of renal parenchyma (Fig. 4). In total there were six patients with solitary lesions, five patients with diffuse renal enlargement, four patients with perirenal lesions, and two patients with direct invasion of the kidney. Multiple lesions as a radiological pattern of renal involvement were not found. A detailed overview of the distribution of radiological patterns among subgroups of lymphoproliferative disease is given in Table 1.

Solitary lesion: contrast-enhanced CT scan of the kidneys in a patient with large cell (diffuse) B-NHL shows a well-defined mass (arrow) in the left kidney
Perirenal lesion: contrast-enhanced CT scan of the kidneys in a patient with diffuse B-NHL shows a perirenal mass (arrow) with soft-tissue attenuation around the right kidney

Direct renal invasion: contrast-enhanced CT scan in a patient with large cell (diffuse) B-NHL demonstrates a large soft-tissue mass with indistinct margins (arrow) located in the left retroperitoneum extending into the left perinephric space. Additionally, the left kidney is hypoperfused in comparison to the right kidney
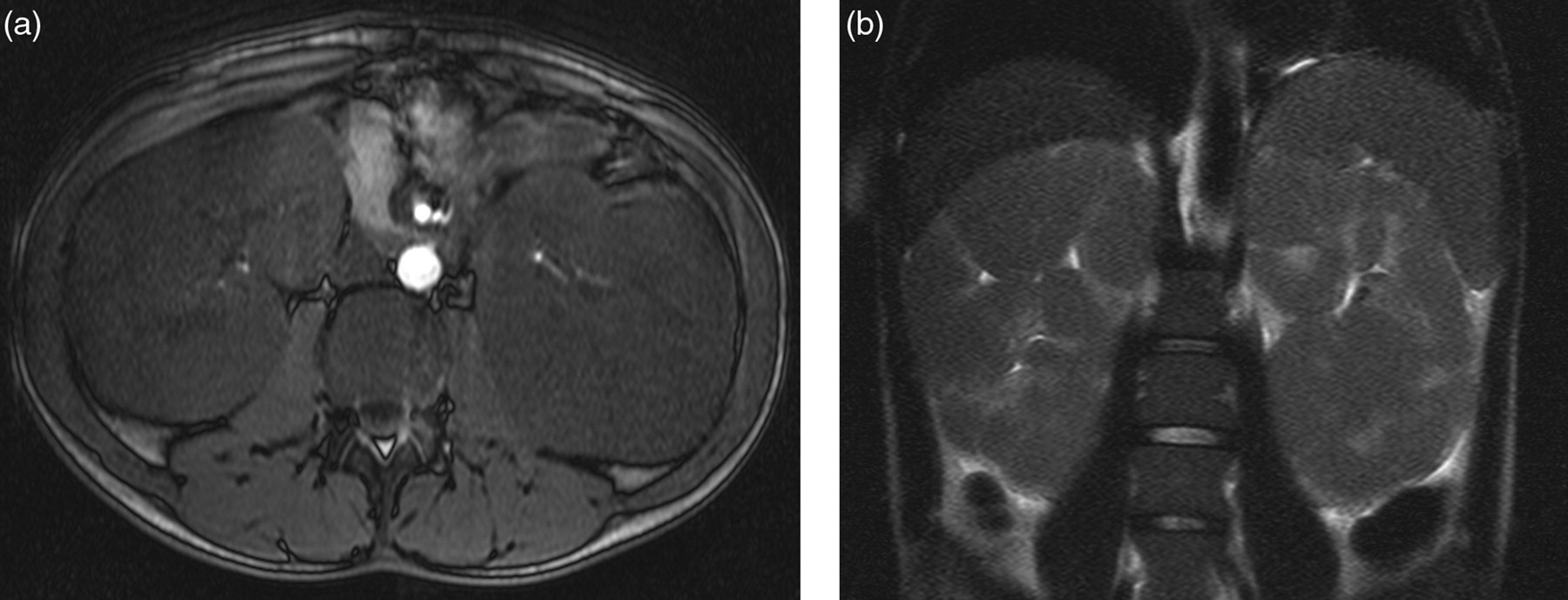
Diffuse enlargement of renal parenchyma: axial T1w (a) and coronar T2-HASTEw (b) MR images in a patient with acute lymphoblastic leukemia and renal failure
In patients with NHL 11 of 364 presented renal infiltration (3%). In most cases there was a solitary or perirenal lesion and the most common subtype was large cell (diffuse) B-NHL (Fig. 3). In three patients creatinine concentration was higher than 100 µmol/L, indicating renal failure. In one patient infiltrates of follicular B-NHL were found together with cells typical for chronic lymphoid leukemia. Therefore, both diseases were diagnosed (Table 1).
Renal involvement was not identified in any of the 41 patients with Hodgkin's disease. However, two of 162 patients with multiple myeloma were proven to have renal involvement (1.2%).
In one case with a solitary lesion, oncocytoma was identified on histopathological examination. However, there was an infiltrate with myeloma cells in the surrounding renal tissue. The same patient presented with renal failure (Table 1).
In 101 patients with leukemia, renal involvement was identified in 5 (5%). The most common radiological pattern was bilateral enlargement of the kidney (3 of 5 cases). One patient suffered from renal failure. Another patient presented with a solitary lesion that was identified as renal cell carcinoma on histopathological examination, together with infiltrates of myelo-monocytic leukemia (Table 1).
Discussion
Renal involvement in malignant lymphoproliferative diseases was first described by Sutton and Turner in 1878 (13). Tumor infiltration of the kidney as part of systemic malignant lymphoproliferative disease was reported with a prevalence of up to 30% in autopsy studies (13, 14). However, in radiological and clinical studies, renal involvement has been found less frequently (Table 2). This discrepancy between the radiological and autopsy/histopathological results may be related to the fact that renal involvement by lymphoma or other malignant lymphoproliferative diseases is clinically silent and often only detectable in histopathological examinations (3, 15). Furthermore, not every patient with leukemia or plasmacytoma undergoes radiological investigation of the kidneys.
Overview of studies on renal involvement in malignant lymphoproliferative disease
n/a = not available, NHL = non-Hodgkin lymphoma, HD = Hodgkin's disease, MM = multiple myeloma
Positron emission tomography (PET) and PET-CT might increase detection rate in the staging of lymphoproliferative disease, because PET detects increased metabolic activity within lymphomatous deposits (3, 16, 17).
In the present study group, in two patients renal lymphoproliferative infiltration was incidentally detected histopathologically (Table 1). As renal infiltration rarely has special therapeutic consequences, routine renal biopsy in patients with lymphoma is not performed.
The median age in patients with renal infiltration is in line with the typical age of manifestation of the different forms of malignant lymphoproliferative diseases.
In children the prevalence or renal involvement in NHL was found to be 8–13% (4, 18). This prevalence is higher than that found in this study in adults. In the present study, there were only 11 children with NHL. None of them presented renal involvement. The exclusive use of intravenous urogram or ultrasound in a number of patients (18) may have led to false-positive results in these reports.
Interestingly, a predominance of boys and men has been reported repeatedly in renal involvement of lymphoproliferative diseases (Table 2). The present data do not support this finding. However, comparison of this aspect with earlier studies is limited. Data about gender distribution in the patient population are missing in almost all earlier reports. Therefore the male dominance might be due to bias in the examined patient population.
Clinically, renal failure in patients with malignant lymphoproliferative disease is a common finding, especially in multiple myeloma (19). However, renal failure is usually not related to the extent of the renal tumor infiltration. Tumor masses may invade or compress the kidney without significantly affecting renal function (3). In most cases renal failure occurs due to tumor-lysis-syndrome (18, 20), infection, nephrotoxic drugs, paraneoplastic syndromes, or obstruction of the urinary system (5, 21).
Therefore, renal lymphoproliferative infiltration is rarely diagnosed by clinical findings. It is most commonly diagnosed on initial radiological examination for staging (18).
In the present study, five of 17 patients with renal lymphoma showed increased serum creatinine at the time of imaging (Table 1). Renal function should be monitored closely because there is a strong correlation between the degree of renal insufficiency and survival (18, 22).
According to the literature (1, 5, 23, 24), there is no difference in radiological appearances of primary or secondary forms of renal lymphoproliferative infiltration. Primary renal infiltration is very rare (23). This is related to the fact, that the kidney contains no lymphatic tissue (5, 24). In the present study with 668 patients included none fulfilled the criteria (5, 25) for primary extranodal renal infiltration.
CT is the imaging modality of choice in most patients with suspected renal masses (3). Previously reported CT patterns in renal involvement of malignant lymphoproliferative disease include solitary lesions, perirenal lesions, direct invasion from contiguous retroperitoneal disease, and diffuse enlargement of renal parenchyma. In the present study, all types were seen.
Multiple lesions have been reported to have a typical pattern as well. The lesions usually range in size from 1–3 cm as areas of decreased enhancement. Similar to single lesions they show a minimal homogenous attenuation. Rarely central necrosis, calcification, or bleeding is seen (11).
However, this pattern was not found in our study group. In patients with diffuse renal enlargement, it is sometimes not possible to distinguish tumor masses, so this pattern may be underlying in some patients with diffuse enlargement of renal parenchyma.
Furthermore, almost all genuine data about the prevalence of radiological patterns date back 20 years and more (26, 27). Since then, these reports have been repeatedly cited (3, 11). Advances in imaging technology as well as in treatment of lymphoproliferative diseases and earlier detection might have changed the distribution of radiological patterns in the last 20 years.
In most cases hematogenous involvement results in bilateral distribution of multiple lesions (28). In the present study six of 17 patients presented bilateral renal lesions. In five of these six patients the pattern was diffuse enlargement of renal parenchyma. This finding is in line with the idea of lymphoproliferative proliferation within the interstitium of the kidney (11).
Most of renal lymphoma in NHL patients are from the B-cell line (1, 4–7, 18, 29). According to the literature, renal lymphoma can manifest with all of the above-mentioned radiological patterns (30). There are no specific correlations between the radiological appearances and cellular subtypes of NHL (1, 4–6, 18, 29, 30). There is one exception to this rule with Burkitt's lymphoma, in which only single and multiple lesions are reported (31). In the present study we did not encounter renal manifestation of Burkitt's lymphoma.
Hodgkin's disease is usually almost entirely confined to the lymph nodes. Extranodal involvement is much less common in Hodgkin's disease than in NHL (32). Renal manifestation in Hodgkin's disease has been reported in less than 1% of patients (4, 14, 32). Its radiological appearance often consists of invasion of the perirenal space (32). In the present study, there was no case with renal infiltration.
Kidney involvement has been described as a common finding in autopsy series of multiple myeloma (33, 34). The most frequently observed pathological feature is myeloma diffuse cell infiltration. In the present study, this infiltration was incidentally detected in one case during the histopathological examination (Table 1). Radiological reports demonstrate kidney involvement as a rare occurrence (35, 36) in about 0.5% of patients (9). The discrepancy between the radiological and autopsy/histopathological results is discussed above. In the other case the pattern was perirenal (Table 1). The lesion presented as a circumscribed hypervascular nodule. An earlier report described perirenal nodular involvement as the most frequently involved extraosseous site (35). In the same report it is speculated that the mechanism of lesion enhancement is likely due to hypervascularity of the plasmacytoma lesions (35).
At autopsy up to 90% of patients with leukemia show renal involvement (13, 14, 37). However, in the majority of cases this infiltration is not related to any macroscopic or imaging abnormalities. Additionally, patients with leukemia do not routinely undergo abdominal CT imaging. As reported previously, the predominant pattern is diffuse enlargement of renal parenchyma, however, any other pattern may be found as well (10, 38). Similar findings are shown in our study. However, in two patients with leukemia, the kidneys showed no radiological abnormalities on CT or MRI and leukemic infiltrates were detected incidentally on histopathological examination.
As described, renal involvement in malignant lymphoproliferative diseases can manifest with several patterns. They should be differentiated from other malignant or benign renal diseases. A solitary, non-cystic, low-attenuation renal mass after contrast enhancement can be seen with renal cell carcinoma, transitional cell carcinoma, metastatic neoplasm, and renal infection. The hypervascular enhancement pattern is more common in renal cell carcinomas than in renal lymphoma (3). In addition, multiple, small bilateral lesions can be detected in patients with multiple angiomyolipomas, fungal infection, and metastatic disease. The finding of a surrounding retroperitoneal mass can be confused with that of a neuroblastoma.
Enlargement of renal parenchyma due to diffuse infiltration is difficult to distinguish from other causes of renal enlargement, such as diffuse renal injury or infection (10).
Therefore, when renal manifestation of lymphoproliferative disease is suspected, histopathology has to be taken into consideration.
In conclusion, in this study renal infiltration in malignant lymphoproliferative disease was detectable via CT and/or MRI in 3% in NHL, 5% in leukemia, and about 1% in multiple myeloma. Four radiological patterns can be identified. In almost all subtypes of NHL and multiple myeloma no specific correlation between typical CT patterns and subtype of lymphoproliferative disease can be found.