
Abstract
Background
Radiofrequency ablation (RFA) is a potential application as a salvage tool after failure of surgery, chemotherapy, or radiotherapy of non-small cell lung cancer (NSCLC). Although several studies have evaluated the use of RFA in primary NSCLC, there is little literature on its potential application as a salvage tool.
Purpose
To evaluate CT-guided RFA employed as a salvage therapy for pulmonary recurrences of NSCLC after prior treatment with chemotherapy, radiation therapy, and/or surgery.
Material and Methods
A retrospective computer database search yielded 33 patients with biopsy proven primary NSCLC who underwent CT-guided RFA of 39 recurrent tumors following surgery, chemotherapy, and/or radiotherapy. Follow-up imaging was performed with CT and PET-CT. The endpoints of interest were progression-free survival (PFS) and time to local progression (TTLP). PFS and TTLP were compared by lesion size (<3 cm, ≥3 cm).
Results
The median PFS was 8 months. For patients with a tumor size <3 cm median PFS was 11 months, whereas the median PFS of patients with a tumor size ≥3 cm was 5 months. The difference did not reach statistical significance (P = 0.09). The median TTLP of all tumors was 14 months. TTLP of ablated tumors <3 cm in size was 24 months, compared to 8 months for ablated tumors ≥3 cm in size. The difference did not reach statistical significance (P = 0.07).
Conclusion
RFA of recurrent NSCLC may be a valuable salvage tool to achieve local tumor control, especially in tumors measuring <3 cm in size.
Keywords
Lung cancer is a significant global health issue, being the most common cause of cancer-related death worldwide (1). Surgical resection represents the treatment of choice and achieves the highest cure rate for localized non-small-cell lung cancer (NSCLC) (2). Nevertheless, the reported recurrence rates after surgical resection range from 16% to 75% (3–6). Chemotherapy and radiotherapy are common components of treatment for advanced disease (7). A recent phase II trial showed local control rates of 98% at 3 years (95% confidence interval [CI], 84.3–99.7%) with the use of stereotactic body radiation therapy (8). However, in recent meta-analysis corrected pooled estimates for 5-year overall survival was 20% for conventional radiation therapy (CRT) and 42% for stereotactic body radiation therapy (SBRT) (9).
Radiofrequency ablation (RFA) is another local therapy that can be used for stage I patients who are not surgical candidates or for those who refuse surgery. However, another potential application of RFA is as a salvage tool after failure of surgery, chemotherapy, or radiotherapy. Although several studies have evaluated the use of RFA in primary NSCLC (10–13), there is little literature on its potential application as a salvage tool (14). The aim of this study was to assess the significance of RFA as a salvage treatment of recurrent NSCLC on progression-free survival (PFS), time to local progression (TTLP), and overall survival (OS).
Material and Methods
Patient eligibility
This retrospective, HIPPA-compliant study was conducted after IRB waiver of authorization. A computer search of the general medical database of our institution was conducted of consecutive patients with histologically proven primary NSCLC who underwent computed tomography (CT)-guided thermal ablation between July 2005 and July 2008. Patients who had previously undergone other treatment modalities (chemotherapy, radiation therapy, and/or surgery) were included. Each patient was evaluated by a multidisciplinary team before ablation. Patients were excluded if it was unlikely to completely treat the lesion. Therefore, no “debulking” was intentionally performed. The longest diameter size was 7.5 cm. The distance from hilar structures was limited to >1 cm. All patients had only one lesion treated with RFA without further lungs lesions. One patient had extrathoracic lesions (bone metastases).
A total of 29/33 patients had pulmonary function tests (PFTs) available. Of these, four had normal PFTs prior to ablation, six had mild, seven moderate, and 12 severe dysfunction. The pulmonary dysfunction was of the obstructive type in 14 patients, restrictive in four and combined in seven patients. Mean (±SD) FEV1 predicted was 64 ± 26% (range, 16–124%); mean DLCO ± SD was 63 ± 20% (range, 35–106%).
Eleven of 33 patients had a normal ECG before the ablation, eight a borderline ECG, and 14 an abnormal ECG. The abnormal ECG generally included sinus arrhythmias, minor blocks, occasional premature ventricular complexes, or findings indicative of old myocardial infarction.
Thermal ablation techniques
Written informed consent for lung tumor ablation was obtained from all patients before the procedure. Preprocedural studies included a coagulation profile and complete blood count. Antibiotic prophylaxis using intravenous cefazolin was provided to all patients. CT guidance (Light Speed 16 or ACT; GE Healthcare, Milwaukee, WI, USA) was used for device placement under general anesthesia in all patients. All ablations were performed by trained interventional radiologists with at least 5 years of experience with this technique. Ablation parameters, including type of applicator and number and length of treatments, were individually planned on the basis of tumor size, location, and shape and were chosen by the operator. The number of ablations was based on the operator's desire to overlap ablations to cover the entire lesion. Immediately after the procedure, patients had both postprocedure CT scans and a radiograph to assess the ablation area and for possible complications. Technical success was defined as finishing the ablation according to the protocol with coverage of the tumor. Thereafter, patients were observed in the post-anesthesia care unit.
Treatment evaluation
For this study, the serial reports and images of 153 CT and 78 fluorodeoxyglucose positron emission tomography (18F-FDG PET)–CT studies were reviewed to define TTLP and time to distant disease progression. All lesions were imaged with CT on the day of RFA. PET-CT imaging was performed in 24 of 39 lesions 0–3 months prior to RFA. To assess early response CT and PET-CT studies obtained within 6 months after ablation were compared to baseline CT which was the first CT study after ablation and to PET-CT studies which were obtained before ablation, respectively. The first CT study after ablation instead of the pretreatment CT was used as baseline CT study as ablation incites an inflammatory response in adjacent normal lung tissue that initially increases the apparent size of the tumor. Modified RECIST criteria (15) and EORTC Recommendations (16) were used to define complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) for CT and PET-CT, respectively.
Patients with lesions that were suspected of tumor persistence after RFA, or that showed poor response in CT, were evaluated with 18-F-FDG PET scans. CT follow-up was performed with multidetector CT (Light Speed 16 or VCT, GE Healthcare, Milwaukee, WI, USA). Unenhanced or contrast material enhanced CT images of the entire chest were acquired using following parameters: beam collimation, 20 mm or 40 mm, respectively; pitch, 1.375 or 0.984, respectively; effective slice thickness, 5 mm; reconstruction interval, 5 mm; tube voltage, 120 kV; tube current, automatic tube current modulation. For contrast-enhanced studies, patients received 100 mL of iohexol (Omnipaque 300; Amersham Health, Princeton, NJ, USA) at a flow rate of 2–3 mL/s. Image acquisition generally began 30 s after the start of contrast material injection. Whole-body PET-CT (Biograph, Siemens Medical Solutions, Erlangen, Germany; Discovery LS, ST, or STE, GE Healthcare, Milwaukee, WI, USA) was performed after acquiring a low dose CT from the skull base to the inguinal region for attenuation correction. PET-CT imaging was performed approximately 60 min after FDG injection. All patients were kept nil per os (NPO) at least 6 h prior to injection of FDG, but water was allowed. Plasma glucose was required to be <200 mg/dl prior to FDG injection in all patients.
Local tumor progression was defined as an interval increase in tumor size or interval onset of irregular nodular tumor shape in CT imaging and/or interval increase of 18F-FDG uptake of the ablated lesion in PET-CT imaging. Multiple measurements were performed for each lesion to rule out measurement variability. Progressive disease was defined as followed: local tumor progression, interval increase of size, and/or 18F-FDG uptake of lesions other then the ablated lesions within the lung or the pleura, new lesions within the lung or pleura with increasing 18F-FDG uptake or with increasing size in follow-up, interval increase of size and/or 18F-FDG uptake of hilar or mediastinal lymph nodes, and new onset of distant metastases.
Statistical analysis
The endpoints of interest were PFS, TTLP, and OS. OS was defined as the time from the date of first lesion ablation until death. Patients who were alive were censored on their date of last contact. PFS was defined as the time from the date of first lesion ablation until disease progression (local or distant) on imaging or death. Patients who were alive without evidence of progression were censored on the date of last imaging. Both OS and PFS were analyzed per patient. TTLP was analyzed per lesion and was defined as the time from the date of first ablation of each lesion until local tumor progression on imaging. Lesions that had not progressed on the date of last imaging follow-up were censored. OS, PFS, and TTLP were estimated by the Kaplan-Meier method. We examined whether lesion size (<3 cm, ≥ 3 cm) was significantly associated with OS, PFS, and TTLP. Comparisons in OS and PFS between groups were assessed by the log rank test. The effect of lesion size on TTLP was analyzed using Cox regression with a robust sandwich covariance matrix estimate to account for the intra-subject correlation of multiple lesions on the same patient. All statistical analyses were performed using SAS 9.2 (Cary, NC, USA).
Results
Patient and tumor characteristics
Thirty-three patients underwent RFA of 39 recurrent tumors in 35 sessions. Twenty-seven patients underwent RFA of one tumor in one session, four patients underwent RFA of two tumors within the same lobe in one session, and two patients underwent RFA of two tumors in different lobes in two sessions. Of the 39 ablated recurrent tumors, 29 were histologically proven. Histology of the recurrent tumors was not available in 10 cases, but all had biopsy-proven NSCLC leading to their initial therapy.
Twenty-three patients underwent initial surgery only, four patients underwent initial surgery and radiotherapy, one patient underwent initial surgery and chemotherapy, and 12 patients underwent initial surgery, radiotherapy, and chemotherapy. Five patients underwent initial radiotherapy only, and five patients underwent initial radiotherapy and chemotherapy.
Patients' and tumor characteristics are listed in Table 1. Fig. 1a summarizes the numbers of initial therapies applied to the patients.
Techniques and numbers of therapies applied to the 33 patients before (a) and after (b) thermal ablation of the tumors Patient and tumor characteristics *Of the 39 ablated tumors, 29 recurrent tumors were histologically proven (21 adenocarcinomas, six squamous cell carcinomas; in two recurrent tumors the NSCLC histology was not further specified by pathology). Histology of the recurrent tumors was not available in 10 cases, but all had biopsy-proven NSCLC leading to their initial therapy. These 10 lesions were assigned to a histological group based on histology of the previously diagnosed tumors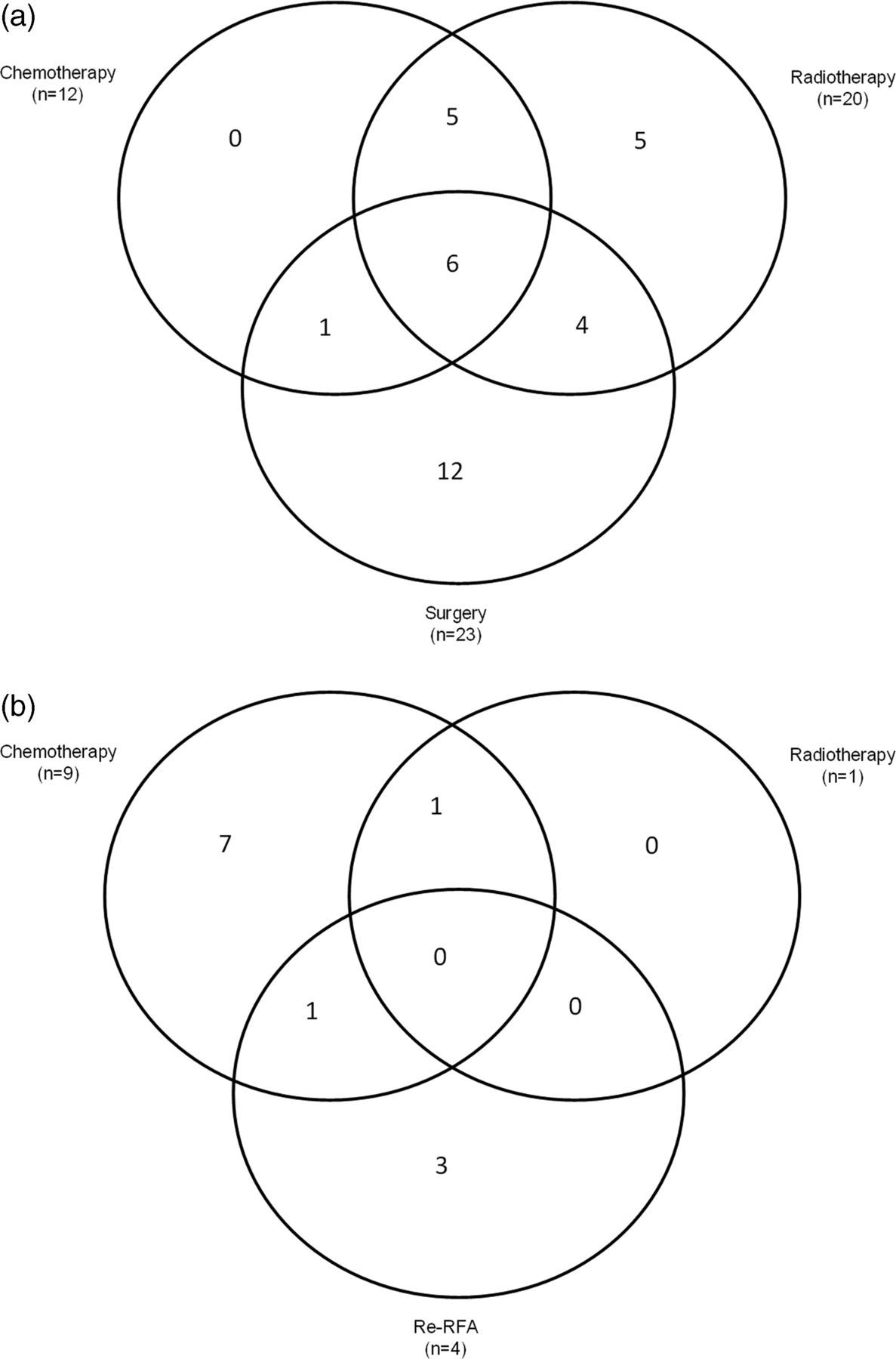
Thermal ablation characteristics
RFA was performed in 39 tumors. A total of eight cases were performed using a RITA Medical Systems device (Starburst-XL, AngioDynamics – RITA, Mountain View, CA, USA), 27 using a Valleylab device (Cool Tip, Valleylab – Covidien, Boulder, CO, USA), and four were performed using a Boston Scientific device (Le Veen, Boston Scientific, Natick, MA, USA). All RFA procedures were performed according to the manufacturer protocols for lung tumors. One ablation cycle was carried out in seven tumors, two ablations cycles in 20 tumors, and three ablation cycles in 12 tumors depending on the tumor size. Tip exposure or length, respectively, was 2 cm in one tumor, 3 cm in 34 tumors, and 4 cm in four tumors.
Follow-up imaging characteristics
Imaging characteristics
Technical success
The technical success rate was 97% (32 of 33 patients). In the patient in whom RFA was unsuccessful two ablation probes were placed into the medially located mass and a small pigtail catheter was then placed to inject air to pull the tumor away from the mediastinum. This failed to withdraw the lung away to a safe distance. The probes were then activated for approximately 2 min to treat adherent tumor cells. No imaging follow-up was available in this patient, because she died 38 days after ablation.
Complications
No intraprocedural deaths occurred. The overall 30-day mortality rate was 3% (1 of 33 patients). Respiratory distress occurred immediately after the procedure in this patient with a history of pneumonectomy, radiation, and underlying severe chronic obstructive pulmonary disease; this patient refused intubation and mechanical ventilation and was transferred to hospice against medical advice. He died of progressive respiratory distress 7 days after ablation. All other deaths were believed to be caused by a combination of systemic cancer progression and medical co-morbidities.
Postprocedural pneumothorax required chest tube placement in 29% (10 of 35 ablation sessions). Median duration for the 10 chest tubes was 1.5 days (range, 1–3 days). There was no case of prolonged air leak (chest tube duration >5 days).
Mild brachial plexopathy which improved after therapy occurred in one case.
The median hospital stay for the 35 ablation sessions was 1 day (range, 1–5 days).
Overall survival, progression-free survival, and time to local progression
There were 33 patients at risk and 21 (64%) of these patients died. The median OS was 21 months (95% CI: 15, 27). The median follow-up for survivors was 24 months. OS did not differ significantly by lesion size (P = 0.38). Table 3 shows the median OS and the 1-year OS for patients with tumors <3 cm and for those with tumors ≥ 3 cm. Fig. 2 shows the Kaplan-Meier curve of OS.
Kaplan-Meier curve of OS. The median OS was 21 months (95% CI: 15, 27). The median follow-up of survivors was 24 months Overall survival (OS), progression free survival (PFS), and the time to local progression (TTLP) compared by lesion size
There were 33 patients at risk and 26 (79%) of these patients progressed or died. Of 20 patients who progressed, 11 patients had local progression only, five patients had progressive disease with local tumor progression and additional lung tumors and/or pathologic hilar lymph nodes and/or pleural carcinomatosis and/or distant metastases; and four patients had progressive disease without local tumor progression. Three patients underwent repeated RFA of the lesion; one patient underwent repeated RFA combined with chemotherapy. One patient underwent radiotherapy of the lesions ablated before combined with chemotherapy, and seven patients underwent chemotherapy after RFA only. Fig. 1b summarizes the further therapies applied after thermal ablation.
The median PFS was 8 months (95% CI: 5, 14). PFS did not significantly differ by lesion size (P = 0.09). Table 3 shows the median PFS and the 1-year PFS for patients with tumors <3 cm and for those with tumors ≥3 cm. Fig. 3 shows the Kaplan-Meier curve of PFS.
Kaplan-Meier curve of PFS. The median PFS was 8 months (95% CI: 5, 14)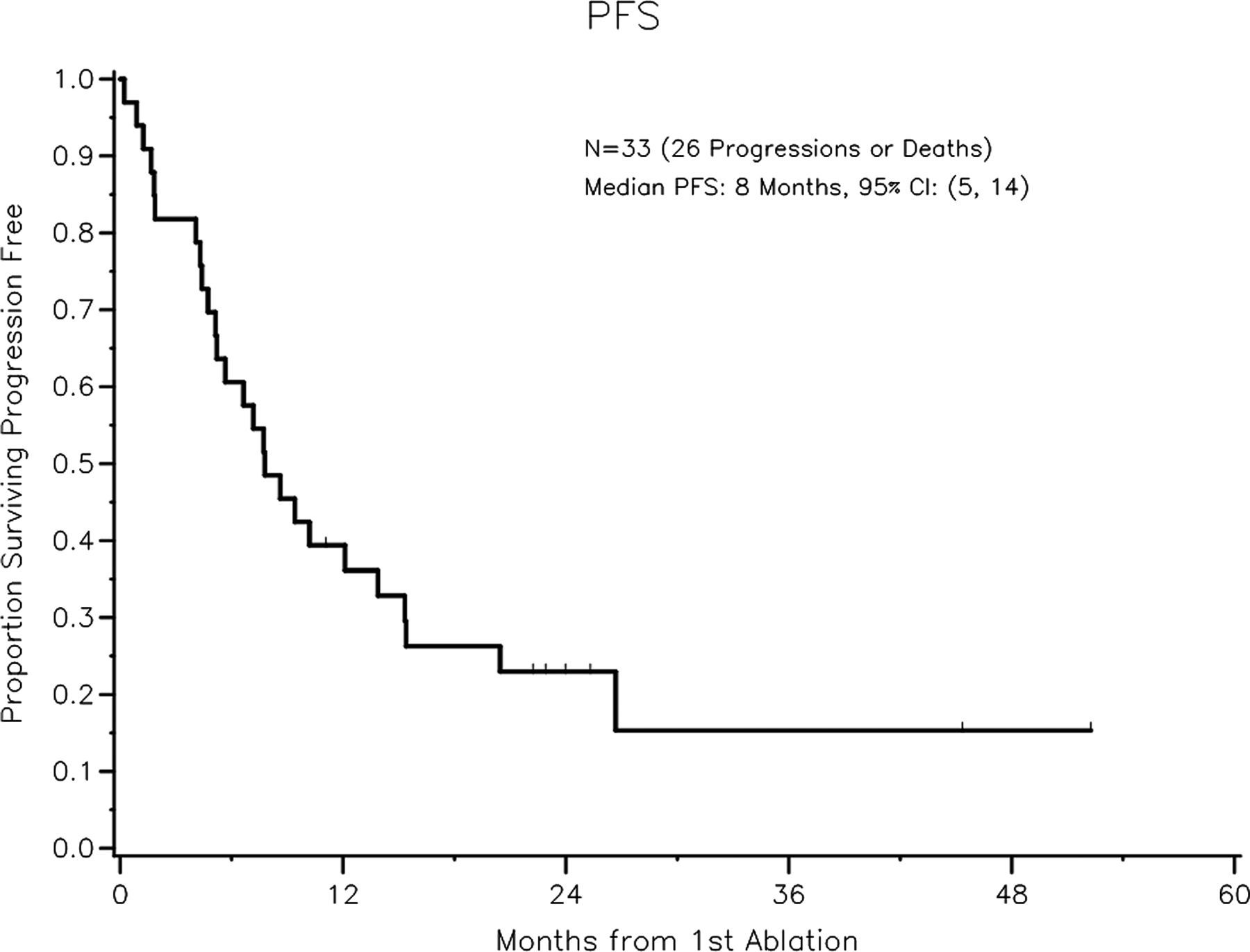
Of 39 tumors at risk, 18 (46%) tumors progressed. The median TTLP was 14 months (95% CI: 9 – not achieved). Table 3 shows the median TTLP and the 1-year LP free rate for patients with tumors <3 cm and for those with tumors >3 cm. The 1-year LP free rate decreased from 65% to 17% when tumors were >3 cm. Fig. 4 shows the Kaplan-Meier curve of TTLP. CR within 6 months was observed in eight (26%) tumors, PR in eight (26%) tumors, SD in eight (26%) tumors, and PD was observed in seven (23%) tumors. In the remaining eight tumors neither baseline CT and second CT nor PET-CT were obtained within 6 months after ablation. Of the seven progressive tumors three tumors were <3 cm and four tumors were >3 cm in size.
Kaplan-Meier curve of TTLP. The median TTLP was 14 months (95% CI: 9, not reached)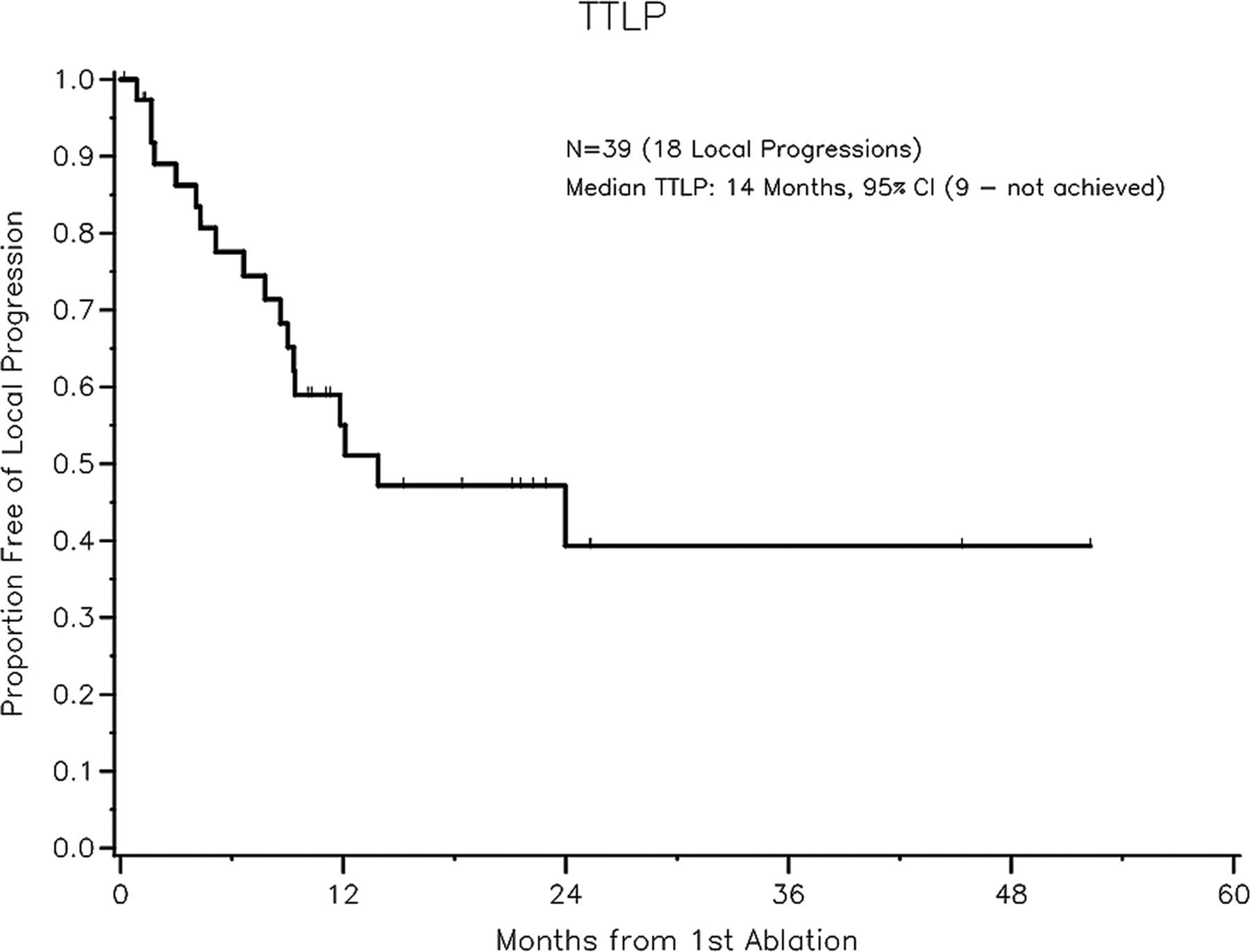
Discussion
Reports of the outcome in patients with primary NSCLC treated with radiofrequency ablation
Performance of salvage ablation of recurrent NSCLC may be more difficult compared to ablation of primary NSCLC due to pre-existing postsurgical or postradiation scarring, which can result in ambiguous tumor boundaries. Also, more aggressive tumor biology may adversely influence outcomes in this subset of patients considering that they have failed their first line of therapy. This may result in different outcomes when compared to patients treated primarily. Pennathur et al. (14) performed RFA of primary NSCLC in 46 patients and recurrent NSCLC in 25 patients and reported a median OS of 27 months for patients with primary NSCLC and an OS of 33 months for patients with recurrent NSCLC. In our study, the median OS of patients with recurrent NSCLC was 21 months and within the range of the reported median OS rates after ablation of primary NSCLC (19 and 29 months) (14, 19, 21, 22). Median PFS was 7 months for primary and recurrent NSCLC as well in the study by Pennathur et al. (14) compared to 8 months in our study. Pennathur et al. (14) reported an initial CR for primary and recurrent tumors in 21%, PR in 41%, SD in 20% and PD in 18%. In our study on recurrent tumors CR, PR, and SD were achieved in 26% each, and PD was observed in 23%. Different numbers of imaging follow up with PET-CT and different definitions of baseline CT (pretreatment CT in the study by Pennathur et al. (14) vs. first post-treatment CT in our study) have additionally to be taken in consideration.
PFS and TTLP were by trend associated with tumor size. The inclusion of large tumors with up to 7.5 cm may have contributed to the decrease of TTLP in tumors >3 cm. The trend association of tumor size with PFS and TTLP obtained in our study for recurrent NSCLC is concordant with studies of primary NSCLC. Simon et al. (19) reported a median TTLP for tumors ≤3 cm of 45 months while median TTLP for tumors >3 cm was 12 months. Ambrogi et al. (17) reported that for tumors < 3 cm, median survival reached 31 months, compared with 15 months for lesions ≥3 cm. Lanuti et al. (13) reported a recurrence rate of 50% for lesions >3 cm, compared to 44% for lesions 2–3 cm in size. Incomplete ablation is most likely the reason for the higher progression rates in larger lesions. In a study by Choe et al. (22) the complete ablation rate was significantly higher in smaller-sized tumors than those in tumors >3 cm. The rate of complete ablation by RFA was 76% for tumors <3 cm and only 28% for tumors >3 cm. In a study by Akeboshi et al. (17), complete tumor necrosis (resolution of FDG-uptake on PET image or contrast enhancement on CT image) was achieved in 69% of lesions ≤3 cm, compared to 39% of lesions measuring >3 cm.
Median PFS of patients who underwent salvage ablation of recurrent NSCLC was shorter in our study compared to published median PFS rates of patients who underwent ablation of primary NSCLC. The median PFS of patients who underwent ablation of primary NSCLC was 15–31 months (13, 15, 17, 18), whereas in our study of salvage ablations of recurrent NSCLC median PFS was 8 months. In a study including patients who underwent ablation of primary NSCLC and recurrent NSCLC as well median PFS was 18 months (15). For patients with primary tumors <3 cm in size, reported median PFS after ablation of primary NSCLC was 31 months (17), whereas in our study of salvage ablation of recurrent NSCLC median PFS was 11 months. For patients with tumors ≥3 cm in size PFS was 15 months (17), respectively, compared to 5 months in our study.
The median TTLP in our study was similar to the TTLP reported for primary NSCLC, although there are limited data available in the literature (10, 12). The median TTLP in our study was 14 months; the tumors had a mean size of 2.8 cm. Reported median TTLP for primary stage I NSCLC varied between 9 months (10) and 27 months (12) for tumors with a similar mean size (2.4 cm (10) and 2.6 cm (12), respectively). The median TTLP was by trend associated with tumor size. The inclusion of large tumors (up to 7.5 cm) may have led to a TTLP of 8 months and a 1-year LP free rate of only 17% in tumors ≥3 cm in size. Of seven tumors that progressed within 6 months, four had a size > 3 cm.
RFA is in challenge with other local salvage therapies such as radiation therapy. In a study by Kelsey et al. (24), median survival after radiation therapy, with or without chemotherapy, was 17 months in patients with local/regional recurrence of NSCLC after surgery; 2-year survival was 38%. Cai et al. (25) reported that patients with postresection recurrent NSCLC achieved survival comparable to that of newly diagnosed NSCLC patients when they were both treated with radiotherapy or chemoradiotherapy. The median survival time was 19.8 months vs. 12.2 months for recurrent vs. newly diagnosed patients; the difference in survival time did not reach significance. Chemotherapy was a significant prognostic factor for progression-free survival (25). Sugimura et al. (26) reported a median postrecurrence survival of 8.1 months in patients who experienced recurrent cancer after complete surgical resection. Surgical treatment for recurrences limited to the lung was performed in a selected group of patients, and median survival was 32.8 months.
The complication rate in our study was within what has been previously reported (15, 19, 20, 27). Pneumothorax requiring chest tube occurred in 29% and has been reported in 10–39% (15, 19, 20, 27, 28). The rate may be high, because patients were under general anesthesia and after the procedure probes were removed while the patients were still being ventilated. This increased pressure may have led to an increased pneumothorax and need for a chest tube. However, the median duration for the chest tubes was on and a half day and there was no case of prolonged air leak.
The overall 30-day mortality rate was 3% (one patient). This death was believed to be procedure-related. Reports showed that 30-day mortality related to the procedure was 0.4–2.6% (28). It has been suggested that exclusion criteria of RFA should include central lesions that are immediately adjacent to major pulmonary vessels or the pulmonary hilum.
Our study is limited by selection bias which is common to retrospective studies, as well as by the low number of patients and by the heterogeneity of the group. Because this was a retrospective study, inclusion and exclusion of patients were rather based on an evaluation by a multidisciplinary team than on strict inclusion and exclusion criteria. Patients had varying numbers of tumors treated with different modalities or combinations. A multivariable analysis could not be performed to look at the differences by treatment modality due to restricted statistical power. Heterogeneity also encompasses re-treatment of recurrent tumors or metastatic tumors. This may have positively influenced OS rates in patients with progressive disease. In addition, longer follow-up may increase the number of survival endpoints. In our study, we did not account for deaths without progression as a competing risk. This may result in a slight over-estimation of the true proportion that is alive and progression-free. Current methods that take into account death as a competing risk in the presence of multiple observations per patient are not available.
In conclusion, our study suggests that thermal ablation of recurrent NSCLC may be a valuable tool to achieve local tumor control, especially in patients with tumors <3 cm in size. Comparing our data to published data of thermal ablation of primary NSCLC suggests that PFS may be shorter for the salvage ablation of recurrent NSCLC than ablation of primary NSCLC.