
Abstract
Background
Potential drawbacks of percutaneous radiofrequency ablation (RFA) for renal cell carcinoma (RCC) include local recurrence after RFA due to a limited ablation area, massive hemorrhage induced by kidney puncture, and difficulty in visualizing the tumor at CT-guided puncture.
Purpose
To evaluate retrospectively the technical success, effectiveness, and complications elicited in patients with unresectable RCC following single-session sequential combination treatment consisting of renal arterial embolization followed by RFA.
Material and Methods
Ten patients (12 RCCs) who were not candidates for surgery were included in this pilot study. All tumors ranged from 18–66 mm in size (mean 31 ± 3.9 mm), and were percutaneously ablated several hours after embolization of the tumor vessels with iodized oil and gelatin sponges. We evaluated the technical success, effectiveness, effect on renal function, and complications of this treatment. Effectiveness was judged on CT and/or MR images obtained every three months after RFA. The effect on renal function was assessed based on the creatinine level and glomerular filtration rate (GFR) before, one week, and three months after the procedure.
Results
Renal arterial embolization followed by percutaneous RFA was technically successful in all patients. On contrast CT and/or MR images obtained one week and three months after RFA we observed necrosis in the embolized segment of all RCCs. There were no major complications during and after the procedure. All patients reported tolerable pain and a burning sensation during RFA. After the procedure, five patients (50%) experienced back pain, one each manifested fluid collection, subcapsular hematomas, hematuria, or nausea. There were no instances of recurrence during a mean follow-up period of 47 ± 3.8 months. We noted no significant difference in serum creatinine and GFR before and after treatment.
Conclusion
Our pilot study suggests that sequential combination treatment by renal arterial embolization followed by percutaneous RFA is feasible in patients with inoperable RCC. The treatment complications were acceptable and excellent effects were obtained.
Laparoscopic partial nephrectomy and laparoscopic cryotherapy are used to treat renal cell carcinoma (RCC) although less invasive treatments are needed in high-risk patients (1–4). Gervais et al. (5) who addressed 42 tumors with 140 ablations in the course of 54 patient visits reported that the treatment of all 29 exophytic tumors proved successful (mean follow-up 13.2 months). On the other hand, Michaels et al. (6) who performed a pathological study of tissues resected after RFA found that especially in patients with central or mixed tumors, RFA did not produce satisfactory results.
A drawback of RFA, with a considerable negative impact on its effectiveness, is its potential cooling effect on the blood flow (7, 8). Reducing or eliminating the blood flow during the RFA procedure increases the volume of ablation (7, 9). Because RCCs are supplied almost entirely by the renal arteries, it seems reasonable to perform RFA after blocking the renal arterial blood flow (10). Another limitation of RFA, the massive renal hemorrhage induced by kidney puncture, may be obviated by arterial embolization before puncture. The administration of a radiopaque agent before RFA may provide a marker for needle puncture under CT guidance.
Under local anesthesia, Arima et al. (11) performed CT-guided percutaneous RFA after arterial embolization in patients with unresectable RCCs smaller than 4 cm. Their technique required two interventional sessions and they used a permanent embolic material to obtain prolonged arterial occlusion. The session interval was six days and they encountered post-embolization complications such as pain and fever and prolonged hospitalization.
In our pilot study we performed selective arterial embolization with a temporary embolic material, gelatin sponge particles, before RFA under real-time CT fluoroscopic guidance to treat unresectable RCCs. Iodized oil was the marker for CT-guided puncture. We assessed the feasibility of this treatment by evaluating its safety and therapeutic effects.
Material and Methods
Patients
Our institutional review board approved this retrospective study and informed consent was obtained prior to intervention. An overview of the patient population and the tumors are shown in Table 1. Between September 2005 and January 2009, 10 patients (seven men and three women with age range 38–93 years, mean 68 years, 12 RCCs) who were not candidates for surgery (poor renal function [n = 2], heart failure [n = 2], a single kidney [n = 2], bilateral tumors [n = 2], severe liver cirrhosis [n = 1], and refusal of surgical treatment [n = 1] underwent treatment comprising arterial embolization followed by RFA. The diagnosis of RCC was based on the results of needle biopsy. The size of the tumors ranged from 18 to 66 mm (average 31 mm). At two to seven days before the procedures we acquired dynamic contrast-enhanced CT scans for the depiction of the RCCs (Fig. 1). The tumor location was classified according to the definition of Gervais et al. (5). Of the 12 tumors, six were exophytic, two were central, and four were mixed. Two patients had von Hippel-Lindau disease, one patient harbored bilateral tumors, and another had only one kidney due to prior nephrectomy for RCC.

Large exophytic-central renal cell carcinoma in a 93-year-old man. An axial arterial-phase dynamic enhanced CT image shows RCCs measuring 6.5 cm and 5.5 cm in the right kidney (lower part of the pole)
Patient profiles
RFA = radiofrequency ablation
Treatment
In all patients we used a temporary embolic material, gelatin sponge particles, for selective arterial embolization. This procedure was followed by percutaneous RFA under CT fluoroscopic guidance. All interventional procedures were performed in an interventional radiology (IVR)-CT unit (AXIOM Artis dTA/VB30E; Siemens, Erlangen, Germany) comprising an angiographic suite and a CT.
Selective arterial embolization
Before RFA the tumor vessels were embolized with iodized oil and gelatin sponge particles. First, under local anesthesia, aortograms were obtained using a 4-Fr pigtail catheter (Medikit, Tokyo, Japan) to evaluate the orifice of the renal arteries. In eight patients whose serum creatinine was less than 2 µg/mL the catheter tip was placed in the abdominal aorta at the level of the renal arteries and an aortogram were obtained using 30 mL of iomeprol (Iopamiron 300; Bayer, Osaka, Japan; 300 mg I/mL) with a flow rate of 10 mL/s.
In the other two patients serum creatinine exceeded 2 µg/mL and in order to preserve the renal function, we did not acquire aortograms. Subsequently, the catheter was replaced with a 4-Fr catheter (RC2; Medikit, Tokyo, Japan) and a renal artery angiogram was obtained after manually injecting 10 mL of iomeprol. Finally, a 2.5-Fr microcatheter (Renegade -18, Boston Scientific, Watertown, MA, USA) was inserted into the tumor vessels (Fig. 2). Iodized oil (Lipiodol Ultrafluid, Laboratorie Guerbet, Aulnay-Sons-Bois, France), which served as a reference for needle puncture of the tumor under CT fluoroscopic guidance, was initially injected. Thereafter, embolization was performed by using gelatin sponge particles (Gelfoam; Upjohn, Kalamazoo, MI, USA) (Fig. 3). The endpoint of embolization was the retention of contrast medium in the feeding vessels. Embolization of the whole tumor was confirmed by CT performed in the IVR-CT unit (10, 11).

Large exophytic-central renal cell carcinoma in a 93-year-old man. Selective renal arteriograph obtained before transarterial embolization shows a hypervascular tumor in the right kidney (lower part of the pole)

Large exophytic-central renal cell carcinoma in a 93-year-old man. The needle electrode was placed under CT-fluoroscopic guidance. The CT image shows the LeVeen needle electrode in the lipiodol-filled nodule after transarterial embolization during the first percutaneous radiofrequency ablation
Percutaneous RFA
All RFA procedures were performed several hours after arterial embolization using a monopolar RF generator (RF3000; Boston Scientific, San Jose, CA, USA) at 460 kHz and a maximum power output of 100 W with the patients under local anesthesia and conscious sedation with 0.1 mg of i.v. phentanyl citrate (Phentanest, Sankyo, Tokyo, Japan). In all cases a coaxial 14-gauge LeVeen needle electrode (Boston Scientific) was used, with a 2, 3, and 3.5 cm array depending on the tumor size.
The needle electrode was placed under CT-fluoroscopic guidance (Fig. 4). After satisfactory deployment, the 2, 3, or 3.5 cm needle was connected to the RF generator and ablation was started at 20, 30, or 40 W. The energy was increased by 5, 7, or 10 W, respectively, every 60 s. Tissue impedance was continuously monitored and ablation was stopped when there was a sharp rise (roll-off). After 1-min cool-down, the tumor was ablated in a second session (11). In cases where we used an electrode with an array diameter or a non-insulated tip length equal to or smaller than the tumor diameter, we created multiple overlapping ablation zones to obtain the ablative margin.
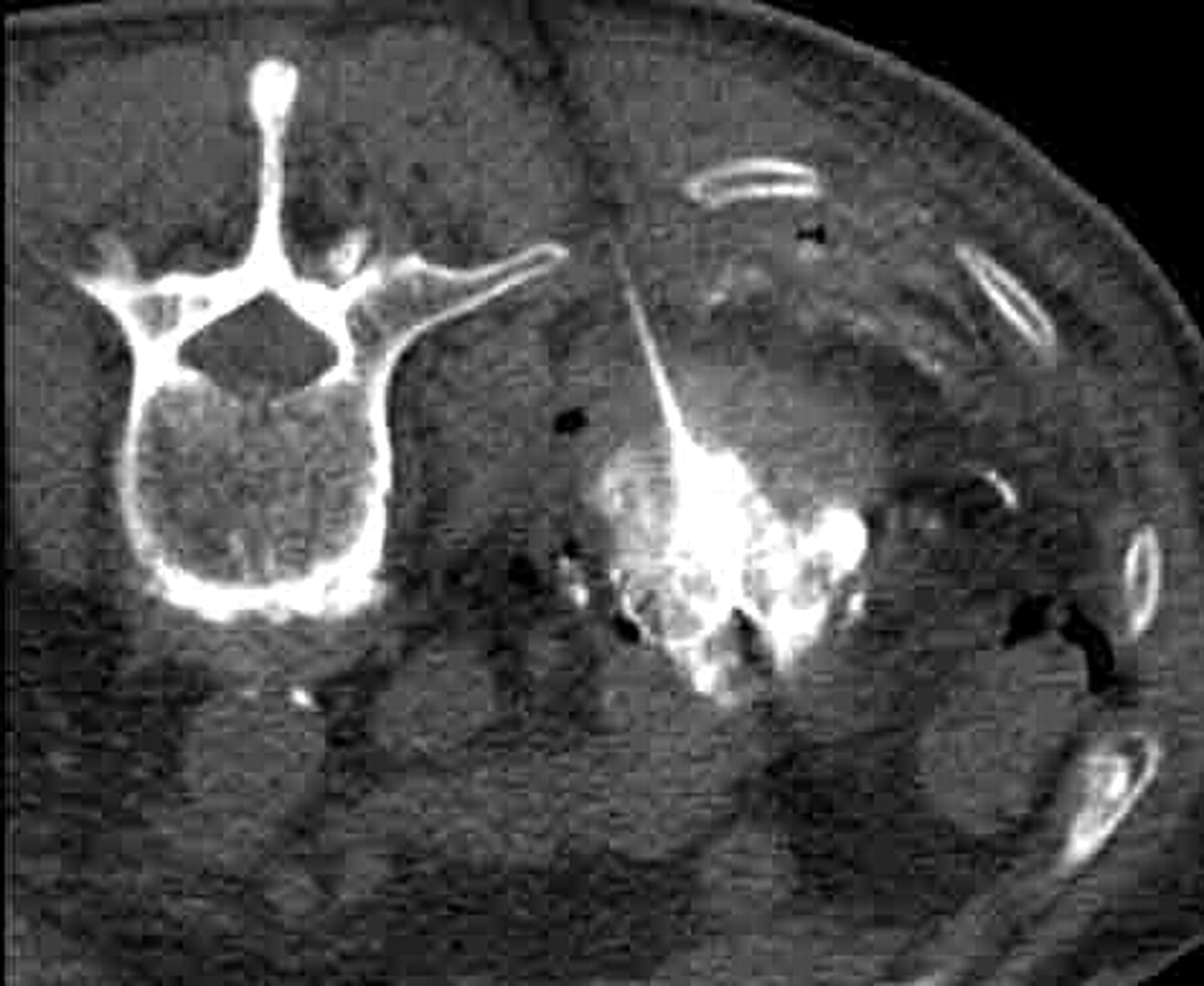
Large exophytic-central renal cell carcinoma in a 93-year-old man. CT image showing the LeVeen needle electrode introduced by the other route during the second percutaneous radiofrequency ablation procedure
Treatment evaluation
Technical success, technique effectiveness, the effect on renal function, and procedural complications were assessed. Therapeutic complications such as abscess formation and hemorrhage were evaluated by contrast-enhanced dynamic CT or MR images obtained within one week after treatment. The imaging studies were repeated every three months after RFA to evaluate the efficacy of treatment.
In cases where dense Lipiodol deposits were observed in the tumor, MR studies were performed to visualize residual enhancement within the mass. CT images were acquired on a 16- or 64-row multidetector CT (MDCT) scanner (Brilliance-16 or 64, Philips Medical Systems, Best, The Netherlands), MR images on a 3T superconductive MR unit (Achieva 3T; Philips Medical Systems). Any lesion enhanced by more than 10 Hounsfield units on CT images was considered viable. Partial enhancement within the tumor on MRI scans was also considered to indicate viability. The effectiveness of RFA was judged on enhanced CT or MR images by the presence of an area harboring non-enhanced tissue that contained the entire treated tumor. Follow-up evaluation was based on contrast-enhanced CT or MR studies performed every three months after RFA.
The effect of treatment on renal function was analyzed by comparing the serum creatinine level (µg/mL) and the glomerular filtration rate (GFR) (mL/min) and recorded before, one week, and 3 months after the procedure. Statistical analysis was with the t-test; statistical significance was defined as P < 0.05.
Complications related to the interventional radiology techniques were classified as major and minor according to the reporting standards of the Society of Interventional Radiology.
Results
Technical success and therapeutic effects
Selective arterial embolization was technically successful in all patients and the angiograms confirmed the retention of contrast medium in vessels feeding the tumor. RFA was technically successful in all patients (Fig. 4). In five tumors that were larger than 35 mm we used a different route to perform a second puncture to obtain coverage of the entire tumor and a sufficient margin (Fig. 5). On contrast-enhanced dynamic CT or MR images obtained within three months after RFA, enhancement disappeared after two RF roll-offs in all tumors (Fig. 6). As contrast-enhanced CT and/or MR images acquired three months after RFA revealed necrosis in the embolized segments of all RCCs, none of the 12 tumors required further treatments.

Large exophytic-central renal cell carcinoma in a 93-year-old man. Axial arterial-phase CT image obtained one week after treatment shows no tumor enhancement and clear non-enhancing tissue around the tumor (tumor-free margin)

Large exophytic-central renal cell carcinoma in a 93-year-old man. Axial arterial-phase CT image obtained 3 months after treatment shows a decrease in the tumor size and no tumor enhancement. Note the clear non-enhancing tissue around the tumor (tumor-free margin)
Complications
There were no major complications during the procedures. All patients reported tolerable pain and burning sensation during RFA. Postoperatively, five patients (50%) reported back pain that required three days administration of analgesics. One of the 12 tumors (8.3%) showed fluid collection in the anterior pararenal space, which was treated with antibiotics for one week. Subcapsular hematoma, hematuria, and nausea occurred in one patient each, but did not require treatment.
There was no significant difference in the mean serum creatinine level and GFR before (1.12 ± 0.18 mg/dL, range 0.66–2.18 mg/dL and 57.59 ± 15.57 mL/min, range 33.1–85.7 mL/min, respectively), one week (1.39 ± 0.29 mg/dL, range 0.64–3.39 mg/dL and 61.02 ± 24.95 mL/min/, range 24.3–93.2 mL/min, respectively), and three months (1.34 ± 0.31 mg/dL, range 0.71–3.52 mg/dL and GFR, respectively) after the procedure.
Follow-up findings
Although no patient experienced local recurrence during a mean follow-up of 47 ± 3.8 months (Fig. 1), one patient with von Hippel-Lindau disease suffered ectopic recurrence. One patient with lung metastases underwent systemic chemotherapy. Another patient with severe liver cirrhosis died of hepatic failure 20 months after RFA treatment, but the death was considered to be unrelated to the RCC.
Discussion
The management options for RCC continue to evolve and recent developments are in the area of nephron-sparing surgery and laparoscopic procedures (2, 12–14). On the basis of their mean growth rate of 3–4 mm per year, it was recommended that small incidentally-discovered RCCs be followed by imaging studies, especially in older patients to avoid nephrectomy or surgery (15, 16). RFA of malignant tumors has been a viable option in patients with primary and metastatic liver lesions, who are not candidates for surgery (7, 8, 17, 18). RFA may also be appropriate to manage some renal lesions (5, 6, 11, 12).
A characteristic of RFA is its cooling effect on the blood flow, which has a considerable effect on the outcome of RFA treatment (7, 8). The reduced efficacy of RFA with respect to large tumors reflects in vivo biophysiological limitations imposed by perfusion-mediated vascular cooling, and this limits heat-induced coagulation necrosis. In animal models it has been possible to increase RF-induced coagulation necrosis by occluding the blood flow to the liver during ablation procedures (7, 9, 19, 20).
Transcatheter arterial embolization (TAE) has been performed to treat hypervascular RCCs (21–23). It can block the renal arterial blood flow and attenuate the cooling effect of the tumoral arterial blood flow. Clinically, RFA combined with transarterial embolization was effective in large tumors other than RCCs (18, 24). Arima et al. (11) used this method to treat stage one RCCs in patients with an increased surgical risk, and performed arterial embolization six days before RFA. To obtain prolonged arterial occlusion they introduced a permanent embolic material, however, they found that materials such as ethanol inflict severe tissue damage and that its manipulation was difficult. Their patients suffered treatment-related complications such as pain or fever. The other permanent embolic material, polyvinyl alcohol foam, is not available in Japan.
As the interval between arterial embolization and RFA in our study was several hours rather than days, the burden placed on our patients was decreased, as were treatment costs. In addition, the length of hospitalization was shorter than after application of the two-session intervention method. We were able to use a temporary embolic material, gelatin sponge particles, for selective arterial embolization. Iodized oil served as a marker for CT-guided kidney puncture and our follow-up imaging studies confirmed that treatment even of large tumors was successful.
Our study has several limitations. First, because it was retrospective, the need for strict inclusion criteria limited the number of patients that we were able to enroll and precluded a meaningful statistical analysis of RFA with renal artery embolization. Second, longer follow-up in more patients is needed to assess the validity of sequential combination treatment for the management of RCC. Lastly, we did not compare the therapeutic effects, complications, and cost-effectiveness of our technique with the two-session method reported by Arima et al. (11).
In conclusion, our study that included a mean follow-up of 47 months suggests that the treatment of RCC by renal arterial embolization with a temporary embolic material followed by percutaneous RFA is safe and effective in patients with inoperable RCC.