
Abstract
Background
Renal artery aneurysms (RAA) are a relatively rare vascular entity. Treatment could be either surgical or via an endovascular route. The main aim of therapy is to prevent lethal rupture.
Purpose
To evaluate the angiographic and clinical results after endovascular treatment (EVT) of eight renal artery aneurysms.
Material and Methods
From January 2000 to June 2011, 18 patients presented with 18 renal artery aneurysms. One was classified as Rundback type I, 15 were type II, and two aneurysms were type III. Endovascular treatment was considered unsafe in 10 cases (all were Rundback type II), and were referred to surgery. The remaining eight aneurysms were treated endovascularly during altogether nine sessions. Among these, four patients were asymptomatic, three were hypertensive, and one presented with ipsilateral flank pains. Aneurysmal sac diameter varied between 12 and 50 mm. EVT included selective coil embolization in five cases, covered stents in two cases, and parent artery occlusion in one.
Results
Follow-up with CT angiography was obtained in all endovascularly treated aneurysms (range 6–54 months, mean 15 months). Complete durable occlusion was achieved in all aneurysms except one, which showed re-expansion after 20 months and was retreated with covered stent implantation. Clinically silent, branch occlusion occurred after four procedures with subsequent limited (less than 25%) ischemic parenchymal loss. All patients were discharged with preserved renal function. Clinical improvement was noted in all symptomatic patients.
Conclusion
Endovascular treatment of renal artery aneurysms is an adequate treatment and can be proposed, if feasible, as first step.
Renal artery aneurysms (RAA) are an uncommon vascular entity, with an incidence of 0.01–0.1% of all body aneurysms (1). The main aim of therapy is to prevent lethal rupture and to relieve symptoms related to the aneurysm (2). Recently, endovascular treatment (EVT) of RAA has emerged as an alternative to the traditional surgery; nonetheless, few small-sized series have been published (3–5). We herein present our experience of endovascular treatment of eight renal artery aneurysms.
Material and Methods
This study was reviewed and approved by our institutional review board as a retrospective study, which does not require informed consent from patients. Between January 2000 to June 2011, 18 patients presented at our institution with 18 renal artery aneurysms that were classified according to their location (Rundback Classification) (6). One was seen on the main renal artery trunk (Rundback type I), 15 were extrarenal at the proximal arterial bifurcations (Rundback type II), and two aneurysms were intrarenal at distal arterial branches (Rundback type III).
After initial diagnostic angiography, endovascular treatment was considered to be unsuitable for 10 cases with type II aneurysms (55.6% [10/18]) due to unfavorable geometry (relative wide necks or incorporation of a branch within the sac). They were therefore referred to surgery and excluded from the study. The remaining eight renal artery aneurysms (44.4% [8/18]) in eight patients were treated by endovascular techniques.
Demographic and clinical data
Among the eight patients treated via an endovascular route, there were five (62.5%) women and three (37.5%) men with a mean age of 58.4 years (range 30–72 years). In four patients, RAA were fortuitously discovered during CT imaging for other unrelated causes. Three patients presented with refractory hypertension, and one patient presented with flank pains at the ipsilateral side of his RAA.
Aneurysmal features
All aneurysms were unruptured at time of discovery, and were saccular in shape with non-calcified walls. One sac was type I, five were type II, and two were type III. The mean sac diameter was 19 mm (range 12–50 mm).
Endovascular treatment
All procedures were performed in one of two angiographic suites (Philips Allura, Best, The Netherlands or Multistar Top, Siemens, Erlangen, Germany). All procedures were performed with patients in a state of moderate sedation and through femoral artery access. After deployment of the first coil, or stent implantation, anticoagulation therapy was initiated, with a loading dose of 2000–3000 IU of systemic intravenous Heparin followed by continuous intravenous infusion of 20–40 IU/kg/h for 2 days. When stents were deployed, dual anti-platelet aggregation therapy (DL-Lysine Acetylsalicylic acid [100 mg/day] and Clopidogrel [75 mg/day]) was prescribed for one month post-treatment, followed by Aspirin (100 mg/day) for another 6 months.
Different endovascular techniques were applied including:
Implantation of covered stent grafts in three cases (one sac type I and two sacs type II), using Jostent Peripheral Stent Graft (JOMED, Helsingborg, Sweden) in two cases, and Advanta V12 (Atrium Europe B.V., SL Mijdrecht, The Netherlands ) in one case (Fig. 1); Coil embolization of the aneurysmal sac using interlocking detachable coils (IDCs; Boston Scientific, Watertown, MA, USA) in five cases (62.5%) (four type II sacs and one type III sac) (Fig. 2); Parent artery occlusion using Amplatzer vascular plug (AVP; AGA Medical, Golden Valley, MN, USA) in one type III intrarenal aneurysm (Fig. 3).

(a) Selective renal angiogram shows type 1 RAA. (b) Control angiogram following covered stent graft placement demonstrates complete aneurysmal exclusion
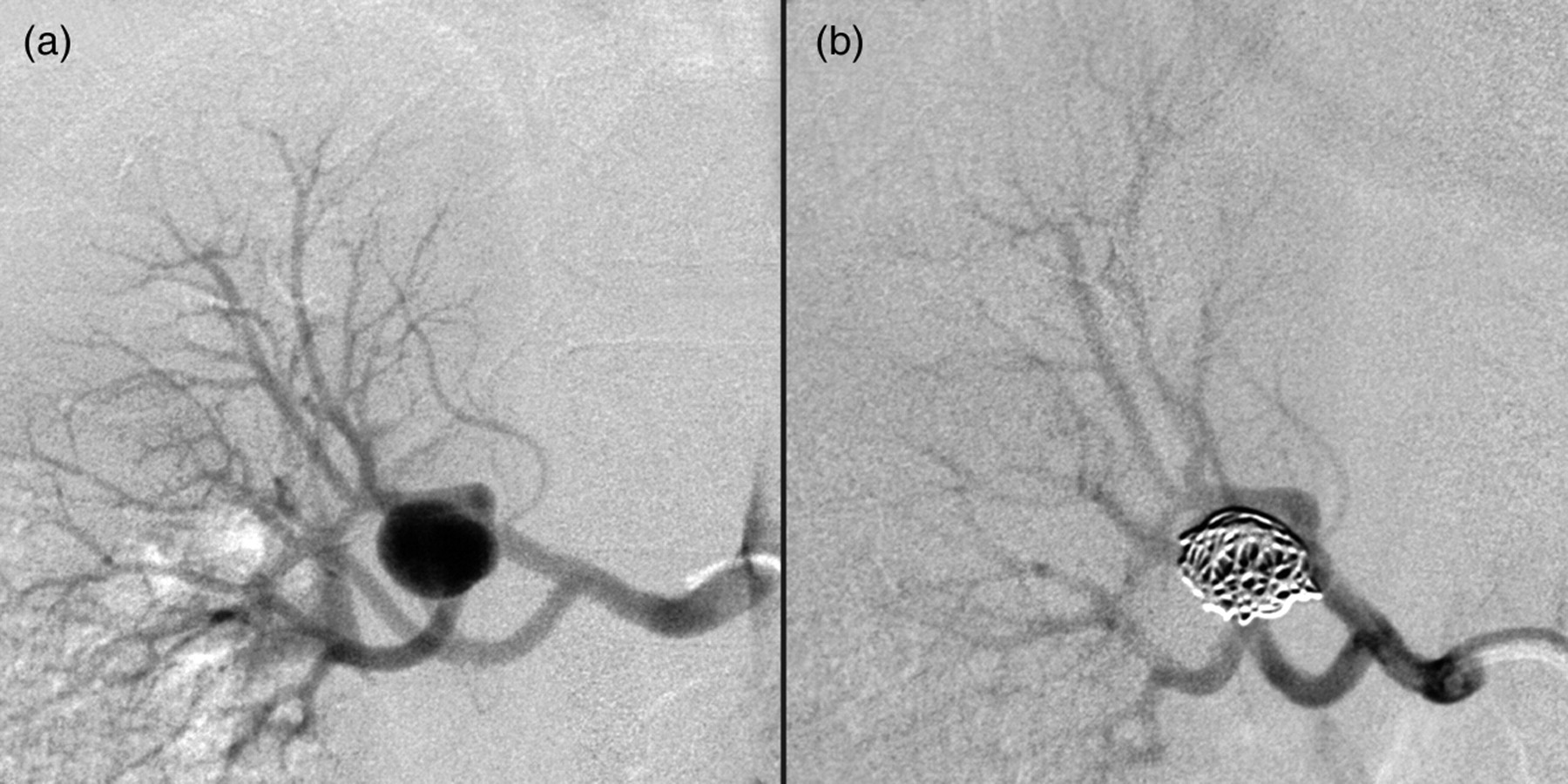
(a) Selective renal artery angiogram shows type 2 RAA. (b) Control angiogram post coil packing shows adequate embolization of aneurysm with preservation of distal branch vessels
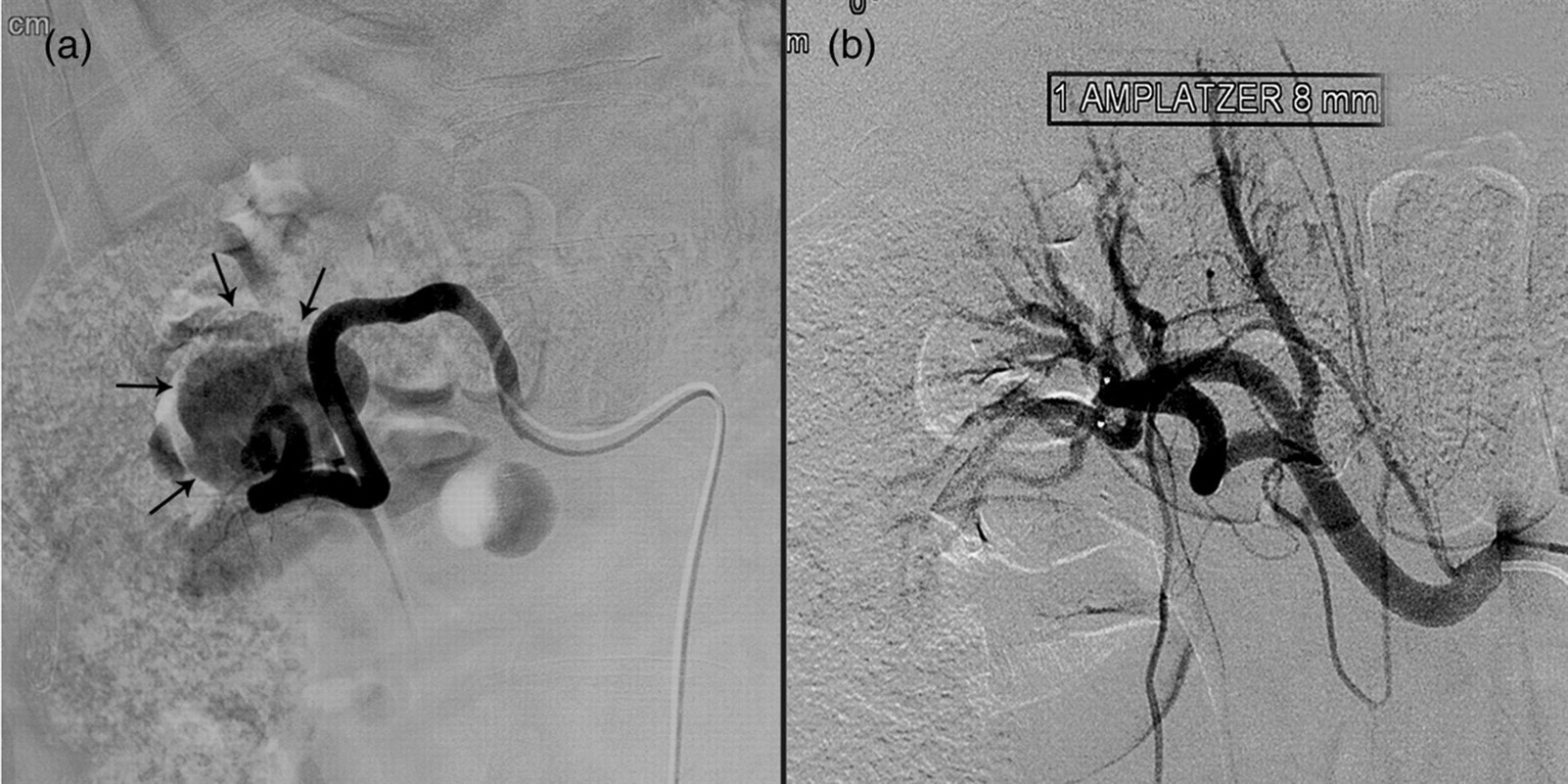
(a) Super selective renal artery angiogram shows a large type 3 RAA (arrows). (b) Control angiogram post parent artery occlusion with Amplatzer vascular plug shows complete aneurysmal exclusion
Follow-up CT angiography was usually performed at one and 6 months, and yearly CT examinations only for cases with initial incomplete sac occlusion, till 3 years post coiling.
Coexisting fibromuscular dysplasia, was simultaneously treated in one case with a type I aneurysm in the same session (Fig. 4).

(a) Selective renal artery angiogram shows type 2 RAA with coexisting fibromuscular dysplasia. (b) Six-month follow-up angiogram, shows complete sealing of the aneurysm, restoration of normal caliber of renal artery with a covered stent and non-significant in stent intimal hyperplasia
Results
Technical results
All aneurysms were completely excluded from circulation and kept stable occlusion during mean follow-up period of 15 months (range 6–54 months) except one, with initial partial occlusion which showed significant re-expansion at a follow-up CT conducted after 20 months and was successfully retreated with complementary coiling and covered stent implantation.
Clinically silent, segmental branch occlusion occurred in four procedures, with subsequent limited parenchymal loss. This occurred due to deliberate branch sacrifice in two cases; using covered stent (in a type II sac) and Amplatzer vascular plug (in a type III sac). In another two cases this event occurred unintentionally due to coil loop herniation in one case and late embolic complications in one.
Clinical results
Postprocedural course was uneventful in all cases with unchanged renal functions at discharge and at subsequent follow-up visits. Clinical improvement was noted in all symptomatic patients with controlled blood pressure in all three hypertensive (passing from three antihypertensive drugs to only one within a one-month period) and relief of flank pain in the fourth patient at the same day of the procedure.
Discussion
Endovascular therapy of RAA offers usually rapid and safe cure while avoiding all the risks of open surgery (7). Different classifications for RAA are available (8, 9). We use a classification proposed by Rundback et al. (6) because of its therapeutic implementation dividing RAA into: type I, saccular sacs arising from the main renal artery trunk; type II, fusiform or saccular, arising at a proximal bifurcation; and type III, intralobar aneurysms, arising from small segmental or accessory arteries.
The definite indication of treatment of RAA constituted a dilemma, regarding the threshold of repair. Treatment is highly recommended for aneurysms measuring 2 cm or more in women of childbearing age and may be indicated in menopausal women and men of all ages (10). The lower morbid-mortality rate of EVT has encouraged some authors to treat aneurysms less than 2 cm in size when the sac is at least twice as large as the parent artery diameter (11, 12), especially when the patient is young or a women of childbearing age, or when the aneurysm is symptomatic, dissecting or shows progressive increase in size (6, 13, 14). When conservative treatment is proposed, annual imaging follow-up is advised.
Many authors have reported their successful experience in EVT of RAA either with selective coiling (simple or balloon-assisted) (3, 5, 15), covered stent deployment (16–22), or with liquid embolic agents (5, 23). The optimum therapeutic choice depends mainly upon the aneurysmal architecture, location, as well as the experience of the interventional radiologist.
Type I aneurysms represent the ideal setting for stenting when the aneurysm is located on a straight renal artery, with its neck away from the renal ostium or the main bifurcation by not less than 15 mm (16–22). Otherwise selective coiling could be proposed (5, 24).
Type II aneurysms are the most challenging due to usual complex surrounding branching pattern and relative wide neck. Coil mesh herniation presents a potential risk, and covered stent implantation necessitates branch sacrifice. EVT is still doable and has been reported using Trispan or balloon-assisted coil embolization (5, 25). The new multilayer uncovered stent system has been tried successfully without branch sacrifice and would therefore increase the feasibility of EVT of type II aneurysms (26). In our series, type II aneurysms constituted 83.3% of all RAA presenting during the study period (15/18 aneurysms). Our feasibility rate of EVT was 33.3% (5/15 type II sacs) and we referred the remaining 10 aneurysms to surgery due to their complex angioarchitecture (wide neck or branch coming from the sac). Without doubt this accurate selection of patients to treat by an endovascular route has contributed to our excellent final results.
Type III aneurysms can be treated with parent artery occlusion using coils or liquid embolic agents (5, 27, 28). We used an Amplatzer vascular plug to occlude the parent artery in one case, offering a rapid, efficacious and safe solution.
The reported rate of EVT related complications varied from 17% to 26% (3–5). Nonetheless, no permanent morbidity or mortality was recorded. In our series inadvertent, clinically silent, branch compromise occurred in 22.2% (2/9) of our procedures. In two other cases, branch sacrifice was deliberately performed as part of the treatment, therefore not considered as a real complication.
The issue of recurrence after RAA embolization has not been thoroughly discussed in the literature. In the current series, significant re-expansion occurred after 20 months post-coiling in one case. Similarly Koganemaru et al. (24) reported a case of recurrence after 15 months. We used to perform a follow-up CT angiography at 1 and 6 months. Afterwards, follow-up is only offered on a yearly basis for cases with incomplete aneurismal sac occlusion for 3 years. Enhanced MR angiography has shown a high sensitivity to detect recurrence (24), nevertheless we refer usually to CT angiography in our follow-up examinations, being sufficient, relatively cheap, and to serve as a baseline to be compared with every other CT examination the patient might do afterwards for any unrelated cause.
In conclusion, the unclear natural history of RAA makes the decision-making of treatment to be based on personal experience. Endovascular treatment can be proposed as the first line of treatment; however, some anatomical difficulties might limit its feasibility. Careful follow-up is necessary to determine the efficacy of these procedures and to obtain long-term follow-up results.