
Abstract
Background
Invasive lobular carcinoma (ILC) is more often multifocal and bilateral than invasive ductal carcinoma. MRI is usually recommended for detection of all ILC sites. The performance of known diagnostic breast MRI criteria for ILC characterization has not been evaluated to date using bilateral mastectomy specimens as gold standard.
Purpose
To determine the value of BI-RADS 2006 MRI criteria for ILC detection and characterization, using pathological examination of bilateral mastectomy specimens as the reference standard.
Material and Methods
Between 2004 and 2007, we retrospectively included all patients with pathologically documented ILC referred to our institution for bilateral mastectomy and preoperative bilateral breast MRI. The location, diameter, and characteristics (BI-RADS) of all lesions were compared with pathological findings. The sensitivity and positive predictive value of bilateral breast MRI for the diagnosis of ILC were calculated. Association of MRI BI-RADS categorical variables and characterization of ILC were assessed (Fisher exact test).
Results
Among 360 patients treated for ILC in 2004–2007, 15 patients qualified for this study. Thirty-one ILC foci were found on pathological examination (30 ipsilateral and 1 contralateral tumor; mean diameter 23 mm; range 2–60 mm) and all were identified on MRI, with 90% of masses and 10% non-mass-like enhancements; MRI features significantly associated with ILC included absence of smooth margins (P = 0.02) and rim-shaped enhancement (P = 0.039). Enhancement kinetics of the 31 foci were evenly distributed among wash-out, plateau, and persistent profiles. Eleven additional lesions were seen on MRI, mainly corresponding to fibrocystic disease; 91% presented as masses and 9% had a wash-out profile.
Conclusion
Based on the 2006 BI-RADS criteria, breast MRI shows a high sensitivity for ILC detection, at the expense of a 26% false-positive rate, suggesting that a pathological proof by US- or MR-guided biopsy is required in case of suspicious MRI images in this context.
Invasive lobular carcinoma (ILC) is the second most common breast malignancy after invasive ductal carcinoma (IDC), accounting for 5–20% of all breast cancers (1–3). Pathologically, ILC is characterized by diffuse infiltrative growth (4), with a stroma infiltrated by tumor cells arranged in a single row and no associated desmoplastic reaction (5), hindering its diagnosis by imaging methods (6). In Hilleren et al.'s study of 137 mammographies in patients with ILC (7), the findings were normal or showed only subtle abnormalities in 20% of cases, while the reported sensitivity of breast ultrasound for ILC ranges from 68% to 88% (3, 5).
Because of its diffuse infiltrative growth, ILC is generally larger than IDC at diagnosis (8). ILC is also more often multifocal (several lesions in the same quadrant) or multicentric (several lesions or one large lesion affecting more than one quadrant) than IDC (3, 5, 9), reaching up to 50% of multifocal/multicentric forms (7, 10) compared to reported 19% rates in IDC (10). ILC also has a greater tendency than IDC to be bilateral, with rates of 6–20% and 2%, respectively (11).
Positive pathological margins after conservative surgery are more frequent in ILC than in IDC (8), leading to more frequent re-excision and local recurrence risk (12). Some authors have suggested that optimal preoperative staging of ILC, including breast MRI, could improve patient outcome (12). MRI has been described as one of the most appropriate tools for ILC staging (3), because of its high sensitivity for ILC detection and staging (range 95–100%) (13, 14) and its high negative predictive value (NPV) (range 95–100%) (2, 5, 6, 13, 14). However, these values were based on core needle biopsies (CNB), lumpectomy, or ipsilateral mastectomy specimens. On CNB, it can be difficult to distinguish ILC from lobular neoplasia (LN), which comprises two subtypes, namely lobular carcinoma in situ (LCIS) and atypical lobular hyperplasia (ALH). In Brem et al.'s study, 23% of 164 lesions classified as lobular neoplasia on CNB in fact corresponded to true neoplastic lesions (DCIS or ILC) after surgical excision (15), and some authors thus recommend excision biopsy when LN is diagnosed on CNB (11, 16, 17).
Only few studies have examined the correlation between enhancing lesions on MRI and pathological examination of the surgical excision specimen (5, 13, 14). Likewise, no correlation studies of bilateral mastectomy specimens and MRI findings have been reported in this setting.
The aim of this study was to determine the value of MRI for ILC detection and characterization, based on the 2006 BI-RADS criteria, using pathologic examination of bilateral total mastectomy specimens as the reference standard.
Material and Methods
Study cohort
Between 2004 and 2007, 360 patients were diagnosed with ILC in our institution. We retrospectively included 15 women, with a mean age of 55 years (range 38–66 years) with CNB-proven ILC who were treated by bilateral total mastectomy and who underwent presurgical bilateral breast MRI. Among those 15 women, eight had known risk factors for breast cancer including five patients with a familial history of breast cancer and three patients who received postmenopausal hormonal therapy for 5 years. Nine women were referred to our institution because of clinical symptoms and six because of an abnormal conventional (mammographic or sonographic) imaging screening. Mammograms were abnormal in 11 cases and sonography was abnormal in 13 cases. Bilateral mastectomy was indicated for surgical and esthetic reasons in 11 cases including small breasts (n = 7 cases) and optimization of postoperative breast symmetry (n = 4). Four women opted for prophylactic bilateral mastectomy in order to avoid close postoperative follow-up. All decisions were approved by a multidisciplinary board of surgeons, oncologists, radiologists, psychologists, and radiation oncologists (18, 19). All patients had breast reconstruction, immediately in 14 cases and one year later in one case.
The mean interval between bilateral breast MRI and bilateral mastectomy was 2 months (0.5–3.5 months, median of 1.5 months) in 13 cases. In the two patients treated by neoadjuvant chemotherapy, respective intervals between surgery, pre-chemotherapy MRI and preoperative MRI were 6 and 1.5 months in one case, and 12 and 2.5 months in the other case.
All patients were alive and free of recurrence after a mean follow-up period of 56 months (range 28–73 months). The median period of disease-free survival was 56 months (range 28–73 months).
Pathology
Pathological analysis of bilateral mastectomy specimens was based on international criteria (20), and was performed by the same senior pathologist with 10 years' experience in breast pathology. Mastectomy specimens were carefully palpated and all indurated areas were located (quadrants, superficial, or deep area of breast) and removed. After that, mastectomy specimens were sliced entirely every centimeter in a transversal plane and all dystrophic or indurated areas were removed. Additional samples were systematically taken from the nipple skin and behind the areola.
Three samples of each dystrophic or indurated area were prepared from each tumor, including one transecting the maximum diameter of the tumor. All sections were analyzed macroscopically and then microscopically after hematoxillin-eosin (HE) staining. The maximum diameter and quadrant location of each tumor were recorded. In case of several closely located multifocal or multicentric tumors, the recorded maximum pathological diameter was defined as the largest distance between the two most distant lesions. The type of the neoplasm (ILC, IDC, or ductal carcinoma in situ [DCIS]) was determined. The quadrant location of lobular neoplasia (LN) associated with ILC was also noted and classified as lobular carcinoma in situ (LCIS) or atypical lobular hyperplasia (ALH) (17). The quadrant location of benign lesions such as fibrocystic disease and fibroadenoma was also recorded.
Breast MRI
MRI protocol
Bilateral breast MRI was performed on a 1.5T system (Siemens Avanto®, Erlangen, Germany), using a four-channel phased array coil, in keeping with international guidelines (21). Sagittal T1 fast spin echo (TR 530 msec, TE 9.8 msec, FOV [field of view] of 23 × 17 cm, matrix of 384 × 158, slice thickness of 4 mm); axial inversion recovery turbo spin echo T2 sequences (TR 9000 msec, TE 70 msec, TI [time of inversion] 120 msec, FOV 32 × 32, matrix 384 × 307, slice thickness 4 mm) were acquired. 3D fast gradient echo (Fast Low Angle SHot) fat-saturated T1 sequences (TR 11 msec, TE 5.6 msec, FOV 28 × 28, matrix 384 × 307, slice thickness 3D 3.3 mm) were acquired once before and seven times after bolus injection of 0.2 mmol/kg gadoteric acid (Dotarem®, Guerbet, Aulnay, France) at a 3 mL/s rate, flushed with 20 mL of saline administered by a power injector. The temporal resolution for each repetition was 49 s. Subtractions were obtained from unenhanced and enhanced dynamic 3D fast gradient echo T1 sequences. The last acquisition obtained was a sagittal T1 fast spin echo post-gadolinium sequence (TR 550, TE 9.8, FOV 23 × 17, matrix 384 × 158, slice thickness 4 mm).
Image analysis
All images were retrieved from the local PACS system and analyzed with Advantage Windows software version 4.4 (GE Healthcare, Milwaukee, WI, USA) by two radiologists (a junior resident with one year of experience and a senior radiologist with 10 years of experience in breast imaging), who were aware of the diagnosis of ILC but blinded to clinical and pathological data. All images were analyzed by consensus. In case of discordance, a consensus was reached with a third radiologist with 15 years of experience in breast MRI. All images were interpreted according to 2006 BI-RADS criteria, including morphological criteria on unenhanced T1WI and T2WI images and enhancement and kinetic profiles following gadolinium chelates injection (21–23). The criteria are summarized in Appendix 1.
MRI pathological correlation
All MRI were interpreted independently from pathological data, MRI abnormalities were matched retrospectively with pathologic data on the basis of their maximum diameter and quadrant location described in the pathologic reports. In the two patients who received neoadjuvant chemotherapy, maximum tumor diameter was evaluated on preoperative MR images. Shape, margins (for masses), distribution of non-mass-like enhancements, and dynamic profiles were evaluated on MR images acquired before chemotherapy. The sensitivity and positive predictive value (PPV) of bilateral breast MRI for the diagnosis of ILC were calculated, with pathological findings as the reference standard. Cases of discordance were analyzed.
Statistics
Correlation between the diameters of ILC found on MR and pathological measurements taken as gold standard was assessed (Spearman). The ILC diameter was used when the neoplasia was unifocal and the largest diameters of all ILC sites – from external border to external border of the two most distant lesions – was used when the neoplasia was multifocal or multicentric.
Comparisons of MRI BI-RADS categorical variables between ILC and false-positive were performed with the Fisher exact test. All statistical analyses were conducted using R Software (
Results
Pathological findings
Thirty-one foci of ILC were identified on pathology (Table 1). Seven patients had unifocal ILC (47%), six patients had multicentric/multifocal ILC (40%), and two patients had bilateral breast cancer (13%), including one patient with one ILC tumor in each breast (patient 11), and one patient with two ILC in one breast and DCIS in the other breast (patient 3).
MRI pathological correlation analysis based on bilateral mastectomy specimens and the 2006 BI-RADS MRI criteria
*The largest distance between the two most distant lesions was collected if ILC was multifocal/multicentric
†MRI characteristics of the lesions were collected before chemotherapy
‡Lesion diameter was collected after chemotherapy
P = patient number, M = mass, NM = non-mass-like enhancement, TP = true-positive, FP = false-positive, HL = ipsilateral to ILC, CL = contralateral to ILC, SEQ = supero-external quadrant, SIQ = supero-internal quadrant, IEQ = infero-external quadrant, IIQ = infero-internal quadrant, UinfQ = union of inferior quadrants, UintQ = union of internal quadrants, USupQ = union of superior quadrants, UExtQ = union of external quadrants, Rar = retroaureolar location, Irr = irregular margins, Spic = spiculated margins, Ductal = ductal distribution, Focal = focal distribution, Rim = rim-shaped internal enhancement, Ho = homoegeneous internal enhancement, Het = heterogeneous internal enhancement, Stip = stippled internal enhancement, Low = slow signal increase on early phase (<2 min), <70% of enhancement, Med = medium signal increase on early phase (<2 min), between 70 and 100% of enhancement, Hi = high signal increase on early phase (>2 min), >100% of enhancement, Type 1 = persistent profile on delayed phase, Type 2 = plateau profile on delayed phase, Type 3 = wash-out on delayed phase, ILC = invasive lobular carcinoma, DCIS = ductal carcinoma in situ, FD = fibrocystic disease, LCIS = lobular carcinoma in situ, FA = fibroadenoma, NA = not available
Nine (60%) of the 15 patients had lobular neoplasia in association with ILC, including the patient (patient 11) with bilateral ILC, who presented with bilateral lobular neoplasia. Two patients had ALH and seven patients had LCIS: all these nine foci were located no further than 1 cm from ILC foci.
MRI pathological correlation
All 31 ILC foci were identified on MRI (Table 1), as 28 masses and three non-mass-like enhancements. Mean MRI diameter of ILC was 27 mm (range 9–65 mm) and pathological mean ILC diameter was 23 mm (range 2–60 mm) with excellent correlation – Spearman correlation coefficient r = 0.92 (95% confidence interval 0.78–1); P < 0.0001 (Fig. 1). MRI showed a mean diameter over-estimation of 4.43 ± 4.38 mm. All ILC foci enhanced following Gd-chelates injection, and all mass lesions had irregular or spiculated margins. No ILC presented smooth margins (P = 0.02). Ten ILC masses showed rim-shaped enhancement (36%), 16 had homogeneous enhancement (57%), and two had heterogeneous enhancement (7%). Rim-shaped enhancement appeared as a distinctive feature of ILC (P = 0.039). Of the three non-mass-like enhancements, one had a ductal distribution with stippled internal enhancement, and two had a focal distribution with heterogeneous enhancement. The enhancement kinetics of these 31 ILC lesions, including masses and non-mass-like enhancements, were evenly distributed (P = 0.36), with 10 wash-out (32.5%), 10 plateau (32.5%), and 11 persistent profiles (35%) (Figs. 2 and 3).
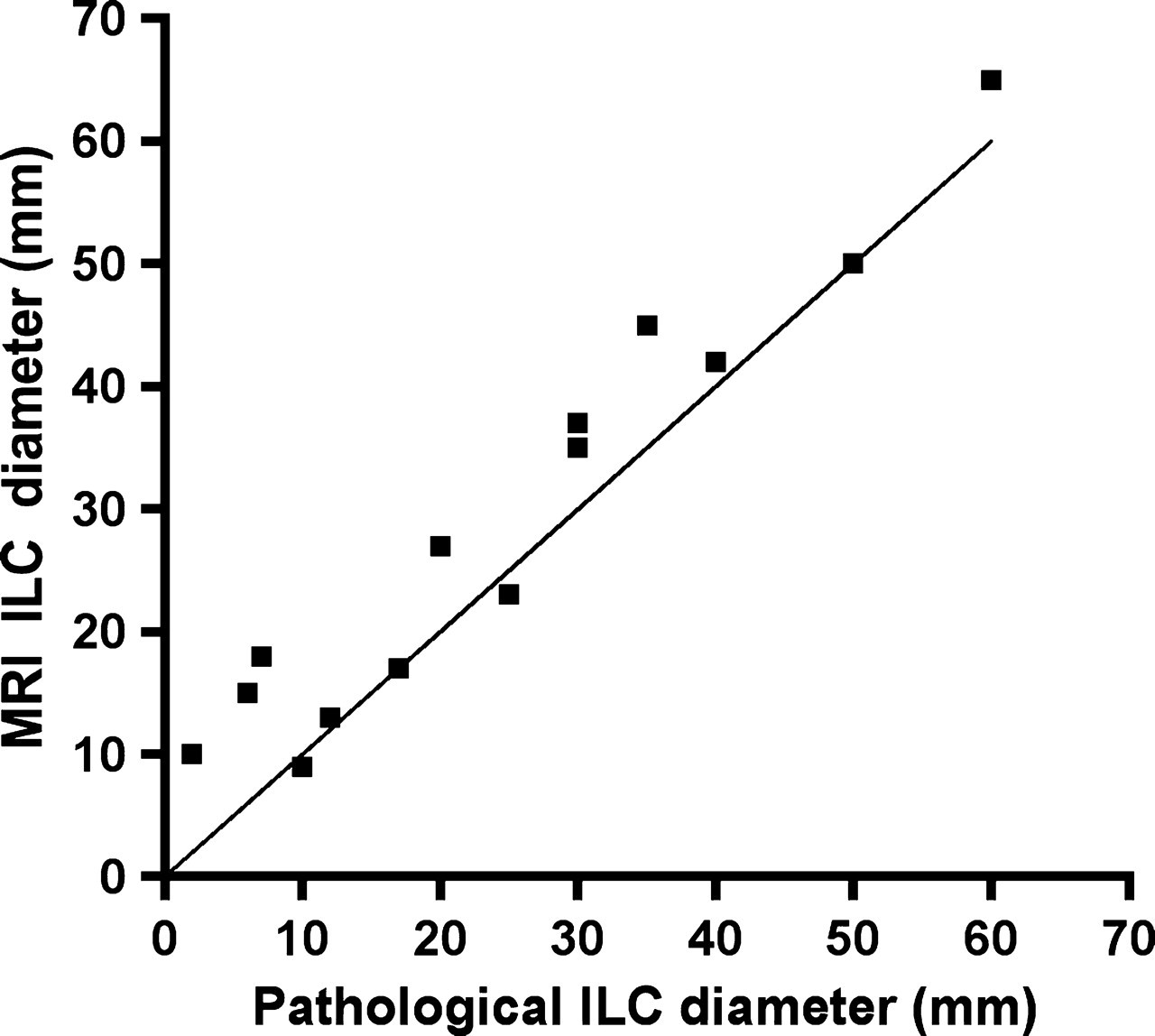
MRI and pathological ILC diameters. Scatter plot showing individual measurements of ILC performed on MRI with the pathological diameter of ILC as gold standard around the line of equality
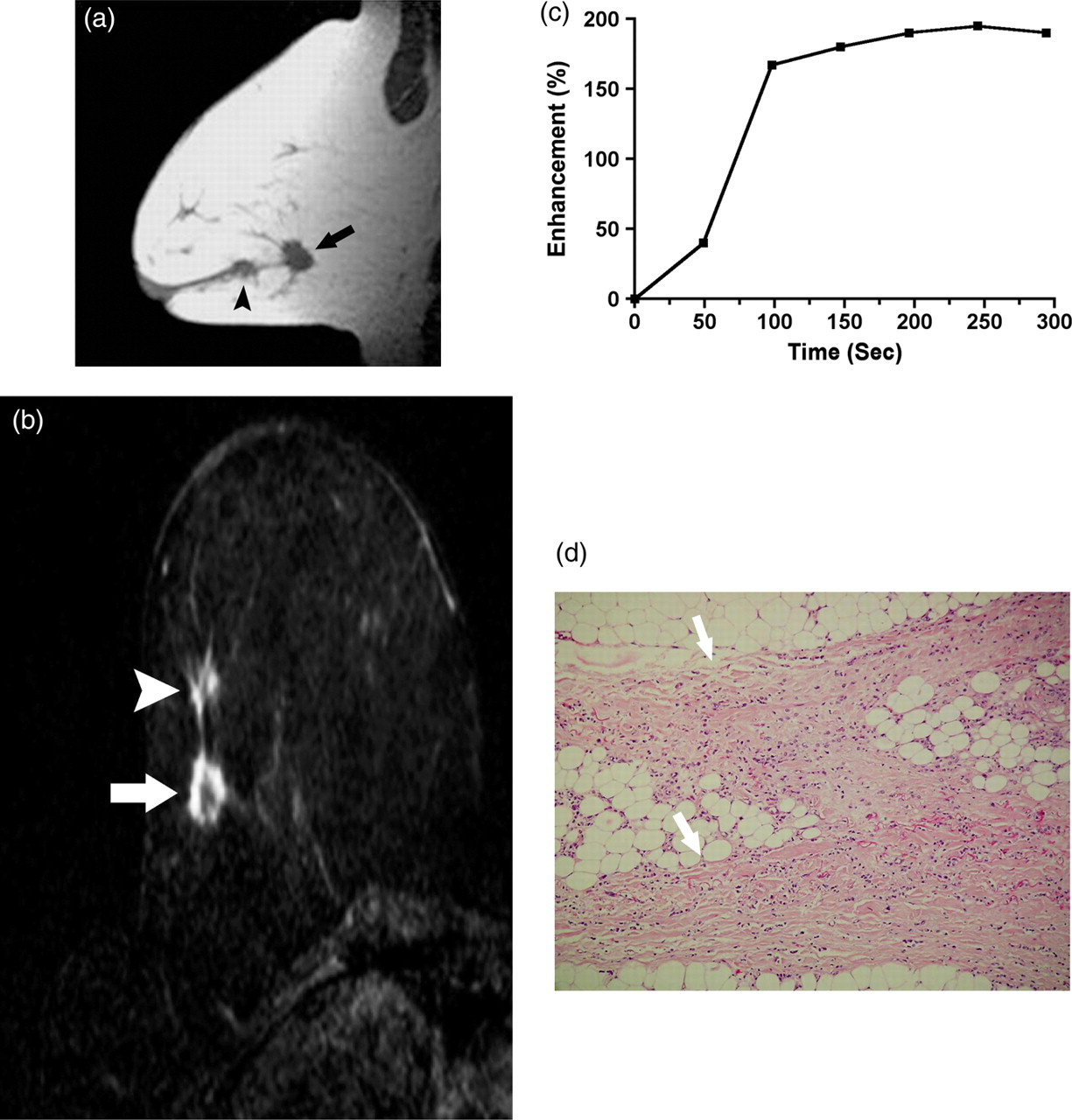
A 50-year-old woman with no personal or family history of breast cancer, with bifocal ILC of the right breast. MR images of the right breast showed two round masses with spiculated margins and with respective largest diameters of 22 and 15 mm (arrow and arrowhead) on sagittal T1WI (a), showing rim-shaped enhancement (arrow and arrowhead in b) after gadolinium chelates injection and type 2 curve (c); Lesions were defined as suspicious ILC lesions using 2006 BI-RADS MRI criteria. On pathology (×25) after HE staining, both tumors showed spiculated margins (arrows in d), and linear arrangement of ILC cells (d)

A 58-year-old woman with a family history of breast cancer, with a 2-cm unifocal non-mass-like enhancing ILC of the right breast. MR images of the right breast showed non-mass-like enhancement, isointense on sagittal T1WI when compared to adjacent breast parenchyma (circle in a). The ILC non-mass-like lesion exhibited a focal and heterogeneous enhancing pattern after gadolinium injection (arrowheads in b) with a type 1 enhancement curve (c) that was identified as a true-positive on 2006 BI-RADS MRI criteria. On pathology (×40) after HE staining, the tumor shows the linear file arrangement of ILC (‘Indian file pattern’) (black arrows in d)
Using 2006 BI-RADS criteria, 11 additional MRI abnormalities in six patients were wrongly classified as ILC (Tables 1 and 2, Figs. 4 and 5), corresponding either to fibrocystic disease (n = 8), fibroadenoma (n = 1), LCIS (n = 1), or DCIS (n = 1). Five false-positive (FP) abnormalities were seen in the ipsilateral breast of four patients, one patient had four contralateral FP abnormalities (patient 8), and one patient (patient 3) had one ipsilateral and one contralateral FP abnormality.

A 41-year-old woman with a family history of breast cancer, with multicentric ILC (four sites of cancer spreading over 35 mm) of the left breast, with a suspicious ipsilateral MR image: MR images of the left breast showed a mass with spiculated margins, hypointense on sagittal T1WI (arrowheads in a) with intense and homogeneous enhancement (arrow in b) and a type 2 curve, erroneously classified as suspicious on 2006 BI-RADS MRI criteria (false-positive image). Pathology (×10) after HE staining showed cystic and dystrophic ducts (black arrows) surrounded by fibrosis, consistent with fibrocystic disease (c)
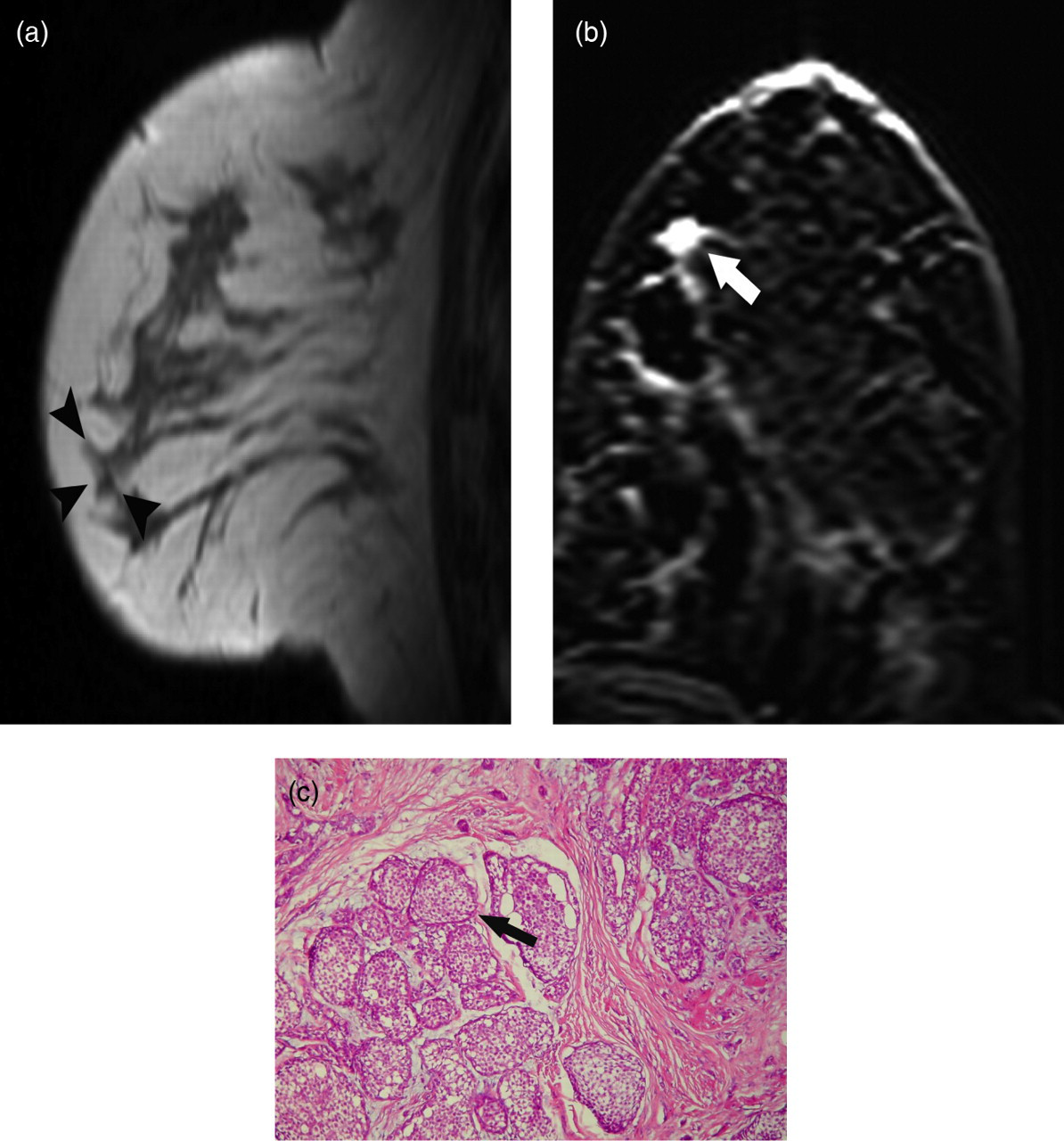
A 51-year-old woman with a family history of breast cancer, with a 15-mm unifocal ILC of the left breast and an additional suspicious MR image on the ipsilateral breast: MR images of the left breast showed a mass with spiculated margins, isointense on sagittal T1WI (arrowheads in a), with homogenous intense enhancement after gadolinium injection (arrow in b) and type 1 curve; the lesion was classified as suspicious using 2006 BI-RADS MRI criteria. Pathology (×40) after HE staining showed ducts filled and distended by non-cohesive tumoral cells, consistent with lobular carcinoma in situ (arrow in c)
Morphologic and kinetic profiles of ILC and false-positive lesions on MRI
M = mass, NM = non-mass-like enhancement, Spic = spiculated margins, Irr = irregular margins, Smooth = smooth margins, Focal = focal distribution, Ductal = ductal distribution, Rim = rim-shaped internal enhancement, Ho = homogeneous internal enhancement, Het = heterogeneous internal enhancement, Stippled = stippled internal enhancement, Curve type on delayed phase = 1: persistent profile on delayed phase, 2: plateau on delayed phase, 3: wash-out on delayed phase
The false-positive abnormalities corresponded to 10 masses (91%) and one non-mass-like enhancement (9%) with a mean diameter of 9 mm (range 5–16 mm). All enhanced after Gd-chelates injection. The enhancement kinetics of these 11 FP lesions corresponded to one wash-out (9%), four plateau (36%), and six persistent profiles (55%). Five FP masses had spiculated margins (50%), two had irregular margins (20%), and three had smooth margins (30%). Presence of smooth margins appeared as a distinctive feature of false-positive finding (P = 0.039).
Based on lesion-to-lesion correlation, the FP rate of MRI for ILC diagnosis was 26% (11/42). Based on 2006 BI-RADS criteria, the sensitivity of MRI for ILC detection was 100%. The PPV of MRI for ILC detection was 74% (31/42) overall, with an ipsilateral PPV of 83% (30/36) and a contralateral PPV of 17% (1/6). If DCIS was included in the calculation of the PPV of MRI for neoplastic foci, the contralateral PPV reached 33% (2/6).
When excluding known ILC from the analysis, the PPV of BI-RADS 4 and 5 additional suspicious images detected on MR for ILC diagnosis was 59% (16/27); if DCIS was included as true-positive MRI findings, the PPV of MR suspicious images reached 63% (17/27). As a result, additional neoplasia foci were detected in 47% (7/15) of the study population.
Discussion
This MRI pathological study based on bilateral mastectomy specimens confirms the known sensitivity of preoperative MRI BI-RADS criteria for ILC detection and characterization, previously reported using only pathological examination of CNB or lumpectomy specimens (24, 25). However, the sensitivity figures might have been overestimated in this study because all radiologists were aware of an existing ILC proven on biopsy. MRI features significantly associated with ILC diagnosis included absence of smooth margins and rim enhancement, figures similar to those reported by Kim et al. (26).
A 26% FP rate was found in our study using 2006 BI-RADS criteria, similar to that reported by Berg et al. (25). Fibrocystic disease accounted for most of these false-positive findings, data similar to that of Baltzer et al. (27). Wash-out enhancement profiles were present in 32% of ILC lesions. Only one focus of fibrocystic disease displayed a wash-out curve, yielding a 91% PPV of wash-out for ILC. Similar figures have been reported by Kinkel et al., suggesting that enhancement kinetics can help to distinguish between benign lesions and ILC (28).
Multifocal and/or multicentric ILC lesions were present in 40% of our patients. All ILC sites were detected on MRI, which is rarely the case of conventional mammograms or sonograms (3, 25). Moreover, some studies (29, 30) have suggested that the rate of local recurrences is higher in patients who undergo re-excision than in patients who are initially successfully treated, and our findings therefore imply that preoperative MRI could improve local control (12).
The overall PPV of breast MRI interpreted with 2006 BI-RADS criteria was 74%, a figure close to that previously reported (5). However, although the prevalence of multifocal/multicentric ILC in our study matched that of previous studies (4, 29), only one contralateral ILC lesion was found in our bilateral mastectomy specimens. We acknowledge that we did not include all consecutive patients with ILC who underwent breast MRI at our institution, but rather only patients who underwent bilateral mastectomy, providing a unique pathological correlation. Our aim was indeed not to determine the prevalence of contralateral lesion, but rather to confirm the known sensitivity of breast MRI in ILC detection not only on biopsy or follow-up data. This selection bias could explain in part the low contralateral PPV of breast MRI for ILC detection (17%) in our study (14–17, 21). Furthermore, we focused solely on the detection of ILC, and not all neoplastic lesions, which further lowered the contralateral PPV, DCIS being considered as a false-positive finding. Given the 100% sensitivity and 26% false-positive rate of breast MRI in our study, atypical MRI findings, especially in the contralateral breast, should be pathologically documented by second-look US- or MR-guided biopsy. Indeed, several studies confirm that the high false-positive rate of MRI for ILC detection is still a challenge; our results further highlight that suspicious images on breast MRI should be documented on pathology before any therapeutic decision (10, 13, 14).
Lobular neoplasia was strongly associated with ILC on pathological analysis in our study. Elsheikh et al. reported lobular neoplasia in 27% of patients with invasive cancer (IDC and ILC) (16). Some authors have underlined the difficulty of distinguishing lobular neoplasms from ILC on CNB (15), while other consider lobular neoplasia to be a risk factor or even an indolent precursor of ILC, warranting its surgical excision (6). In our study, all foci of lobular neoplasia were located no further than 1 cm from ILC foci. Thus, the detection of lobular neoplasia on CNB may point to the presence of closely located ILC foci. Besides, it can also explain why diameters of ILC on MR were overestimated compared to pathology in most of the cases but that the over-estimation is relatively constant and mild, and does not increase with the diameter of the tumor.
One limit of this study is its retrospective design, which did not allow pathological examination to be guided by MRI. The small number of patients is also a drawback, but bilateral mastectomy is rarely indicated for patients with unifocal, multifocal or multicentric ILC. To our knowledge, our study is the first to provide pathological correlations based not only on follow-up and CNB but rather on full mastectomy specimens. As previously mentioned, the sensitivity of MRI for ILC might have been overestimated, because the radiologists were aware that each patient had at least one focus of ILC detected on CNB. Our study design was, however, not intended to provide prevalence data of ILC. PPV of additional neoplastic lesions discovered on MRI is of critical importance in the clinical management of ILC patients. Our study based on analysis of bilateral mastectomy specimen led to the detection of new sites of tumor for 47% of the 15 patients. Again, these figures could have been impacted by the selection bias: only patients who underwent bilateral mastectomy were included. Thus the overall contralateral prevalence of ILC cannot be determined using this study. On the opposite, our findings suggest that all BI-RADS 4 and 5 suspicious MR findings should not be overlooked as suggestive of ILC lesions (26% of false-positive lesions in our study) and require MR- or US-guided second-look biopsies (10, 13, 14). Taken together, our data first confirm that bilateral breast MRI allows detection of all ILC foci, even with bilateral mastectomy specimens as the reference standard, but at the expense of additional invasive diagnostic procedures in order to rule out malignancy in equivocal contralateral abnormalities.
In conclusion, MRI showed sensitivity figures in line with previously published data for additional ILC sites detection and characterization, using bilateral mastectomy specimens as the reference standard. Ninety percent of ILC foci corresponded to masses, all of which had irregular or spiculated margins. MRI detected all multifocal, multicentric or bilateral ILC foci. However, the high false-positive rate (26%) suggests that suspicious MRI images should be verified by US- or MRI-guided biopsy.
Footnotes
2006 BI-RADS criteria for MRI (21)
Mass = A mass is a space-occupying tumor that has three dimensions. Usually, it has a visible correlate on pre-contrast T1- or T2-weighted images
Non-mass-like enhancement = Non-mass-like enhancement means that enhancement occurs in an area of the fibroglandular tissue that otherwise appears normal on pre-contrast images. There is no space-occupying effect. The enhancing area usually has no correlate on fat-suppressed or non–fat-suppressed T2-weighted images
Type 1 = kinetic curve showing persistant profile on delayed phase
Type 2 = kinetic curve showing a plateau on delayed phase
Type 3 = kinetic curve showing a wash-out on delayed phase (31)