
Abstract
Background
Hepatobiliary paragonimiasis (HP) is not commonly encountered and may be confused with hepatobiliary tumors; however, computed tomography (CT) and magnetic resonance imaging (MRI) features of HP allow this entity to be distinguished from other diseases.
Purpose
To present the CT and MRI findings in patients with HP and to describe some specific imaging findings along with their pathological correlations.
Material and Methods
Imaging and clinical findings of 21 patients (9 boys/men and 12 girls/women; age range 3–67 years; mean age 40 years) who were diagnosed with HP were retrospectively evaluated. Among these patients, 16 underwent CT examination only, two had MR examination only, and three underwent both CT and MR. All patients underwent surgery, and the HP diagnosis was confirmed by the surgical and histopathologic results.
Results
Chronic abdominal pain or back pain was reported by 14 patients, severe abdominal pain with acute onset was reported by one patient, and six patients were asymptomatic and were discovered incidentally. Peripheral eosinophilia was present in 14 patients (14/21, 66.7%), and abnormal liver function tests were found in 16 patients (16/21, 76.2%). Of the 19 patients who underwent CT imaging, 17 patients showed multiple mixed hypodense lesions or multiple cysts with inlaying septation with separate irregular rims or circular enhancement on post-contrast CT images. Tunnel-shaped microabscesses and necrotic cavities were found in the lesions of 12 of those 17 patients. The other two patients showed smaller cystic masses. MRI showed faveolate T1 hypointense and T2 hyperintense areas in the liver parenchyma with rim or peripheral enhancement. Nodular or circular hyperintense materials were found scattered in the lesions on T1-weighted imaging.
Conclusion
CT and MRI can reveal the radiological-pathological features of HP. Together with laboratory findings, MRI and CT findings may provide diagnostic clues, especially in endemic areas, that are very important for the selection of treatment methods.
Paragonimiasis is a zoonosis caused by adult trematodes of the paragonimus genus, Paragonimus skrjabini, Paragonimus westermani, and related species. Hepatobiliary paragonimiasis (HP) is trematodiasis of the liver and bile tract caused by paragonimiasis infection. Most HP patients are infected with Paragonimus skrjabini (1). The diagnosis of HP can be difficult and is usually delayed because paragonimiasis is not commonly encountered, and the clinical manifestations may be non-specific. However, imaging studies may be specific and can demonstrate the severity of involvement. Moreover, definitive diagnosis can be made only by imaging studies.
The purpose of this retrospective study was to evaluate 21 consecutive HP patients, describe the magnetic resonance imaging (MRI) and computed tomography (CT) imaging patterns that are characteristic of HP, and to evaluate the correlations between imaging findings and pathology.
Material and Methods
Patients
The imaging and clinical findings of 21 consecutive patients who visited our hospital between January 2008 and May 2010 and were confirmed to have HP were analyzed retrospectively. The patient group included nine boys/men and 12 girls/women ranging in age from 3 to 67 years (mean age 40 years). This study was conducted according to the ethical standards of our institution and was approved by our review board. Hematological, alpha-fetoprotein (AFP), and liver function tests were performed in all patients. The CT and MR findings of all patients were confirmed by the surgical and histopathological findings.
CT and MR protocols
Of the 21 patients, 16 underwent abdominal CT examination, two underwent MR examination, and three underwent both CT and MR examinations. In the 19 patients who underwent CT examinations, nine were evaluated with a 64-channel multislice CT (MSCT) scanner (Brilliance 64, Philips, Best, The Netherlands), and 10 were imaged with a 16-channel MSCT scanner (Brilliance 16, Philips, Best, The Netherlands). All 19 patients underwent a non-contrast CT scan first, which was followed by administration of 2–3 mL/kg of an iodinated contrast material (Ultravist 300 mgI/mL, Bayer Schering Pharma AG, Berlin, Germany) via an antecubital vein at a rate of 3.0 mL/s using a 20-gauge needle and an automatic injector. The contrast-enhanced CT scan was routinely started 25 s after the contrast injection (arterial phase), as well as at 60 s after the injection (portal venous phase). All MR imaging exams were performed on a 1.5 T MR unit (Avanto, Siemens Medical Solutions, Erlangen, Germany). Five patients received 0.1 mmol/kg of gadopentetate dimeglumine contrast agent (Magnevist; Bayer Schering Pharma AG, Berlin, Germany) into the antecubital vein followed by a 10-mL flush with normal saline solution.
Imaging analysis
All CT and MR images from each patient were evaluated with the consensus of two radiologists with 7 and 10 years of experience in abdominal radiology.
Results
Clinical presentations and laboratory results
Of the 21 patients, 14 presented with chronic abdominal pain or back pain accompanied by low-grade fever, nausea, weakness, or lack of appetite; one patient suffered from acute, severe abdominal pain, and six patients were asymptomatic and were discovered incidentally. The duration of the symptoms ranged from 8 days to 1 year. Peripheral eosinophilia was present in 14 patients (14/21, 66.7%), with a differential count ranging from 6–52%. Abnormal liver function tests were present in 16 patients (16/21, 76.2%), and one patient had an elevated AFP (this patient was initially misdiagnosed as hepatic carcinoma). A careful inquiry following surgery found only eight (8/21, 38.1%) patients with a definite history of ingesting uncooked freshwater crab or crayfish within 6 months. Stool examination for various parasitic eggs was negative in all patients.
CT and MRI manifestations
The CT/MRI manifestations of the HP lesions in the 21 patients were as follows: size (>3.0 cm, 15 patients; ≤3 cm, 6 patients); location (right lobe, 14 cases; left lobe, 3 cases; both lobes, 4 cases); margins (obscure, 15 cases; clear, 6 cases); and appearance (cluster, 19 cases; nodosity, 2 cases). Dilation of the bile duct and hyperemia of the surrounding liver tissues were found in seven (7/21, 33.3%) and three (3/21, 14.3%) patients, respectively. There was only one case of abdominal lymphadenopathy (1/21, 4.8%). Branches of the portal vein penetrating the lesions without stenosis or interruption were found in six patients (Fig. 1). The chest X-ray films were normal for all 21 patients. Plain chest CT scans were obtained in two patients, and their CT findings were also normal.
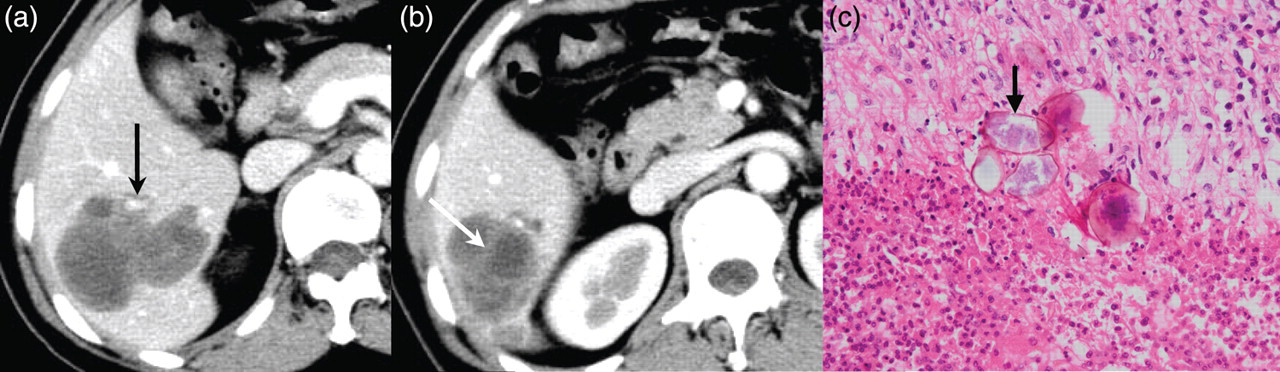
HP, 44-year-old woman. Contrast-enhanced CT obtained during the portal venous phase shows a clump of multiple mixed low-density lesions located in the right posterior lobe of the liver with sparing of the right posterior branch of the portal vein (a, black arrow) and the septa enhancing (b, white arrow). Photomicrograph of a specimen obtained near the liver lesions revealed paragonimus eggs (c, arrow) with chronic granulomatous inflammation (H-E stain, ×400)
Of the 19 patients who underwent CT examinations, 17 showed multiple mixed hypodense lesions or multiple cysts with inlaying septation with separate irregular rim or circular enhancement on post-contrast CT images. Tunnel-shaped microabscesses and necrotic cavities were found in the lesions in 12 of those 17 patients. The other two patients showed smaller cystic masses. All lesions became clearer on contrast-enhanced CT (Figs. 1–3). All CT values were between 20–45 HU on the unenhanced CT scans and were increased by approximately 10 HU or 20 HU on the arterial-phase and portal-phase contrast CTs, respectively.
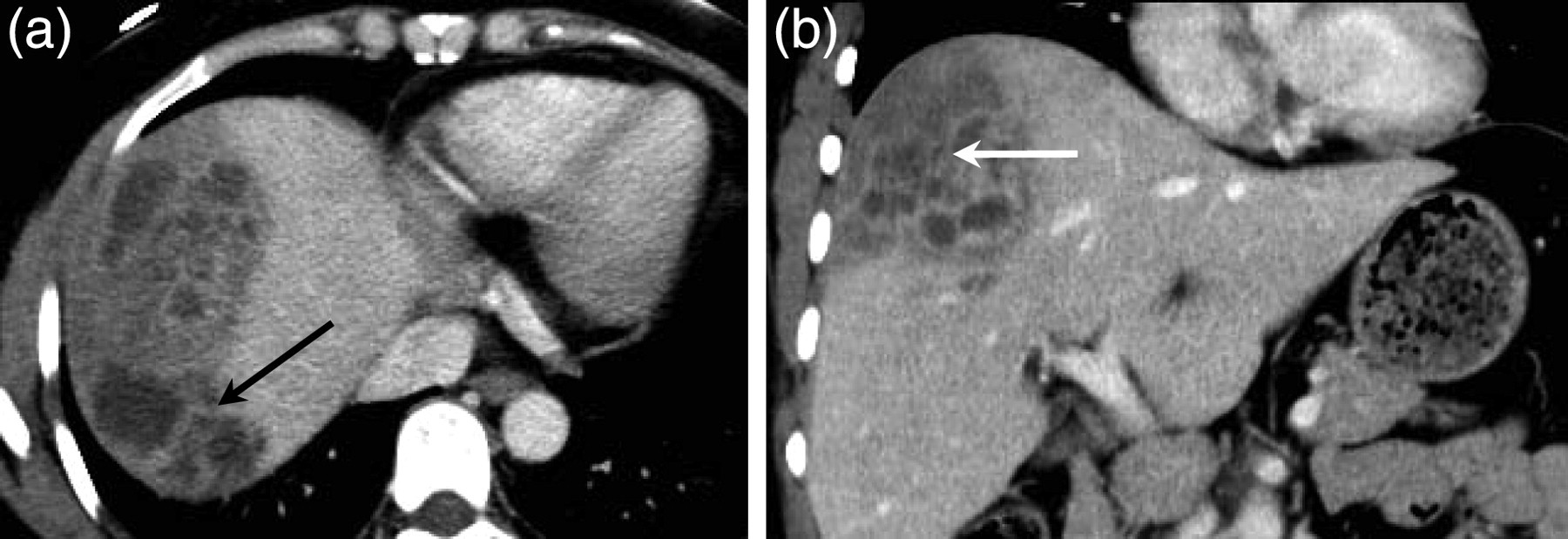
HP, 67-year-old man. Axial post-contrast CT image during the portal venous phase shows a cluster of multiple mixed low-density lesions with enhancing rims located in the left lobe of the liver. Note the mild dilation of the bile duct (a, black arrow) and multiple tunnel-shaped microabscesses extending to the subcapsular region at the periphery of liver (b) HP, 44-year-old woman. Axial and coronal post-contrast CT images during the portal venous phase (a, b) show a cluster of multiple cysts with inlaying septation (black arrow) and tunnel-shaped microabscesses with separate circular enhancement (white arrow) located in the hepatic subcapsular areas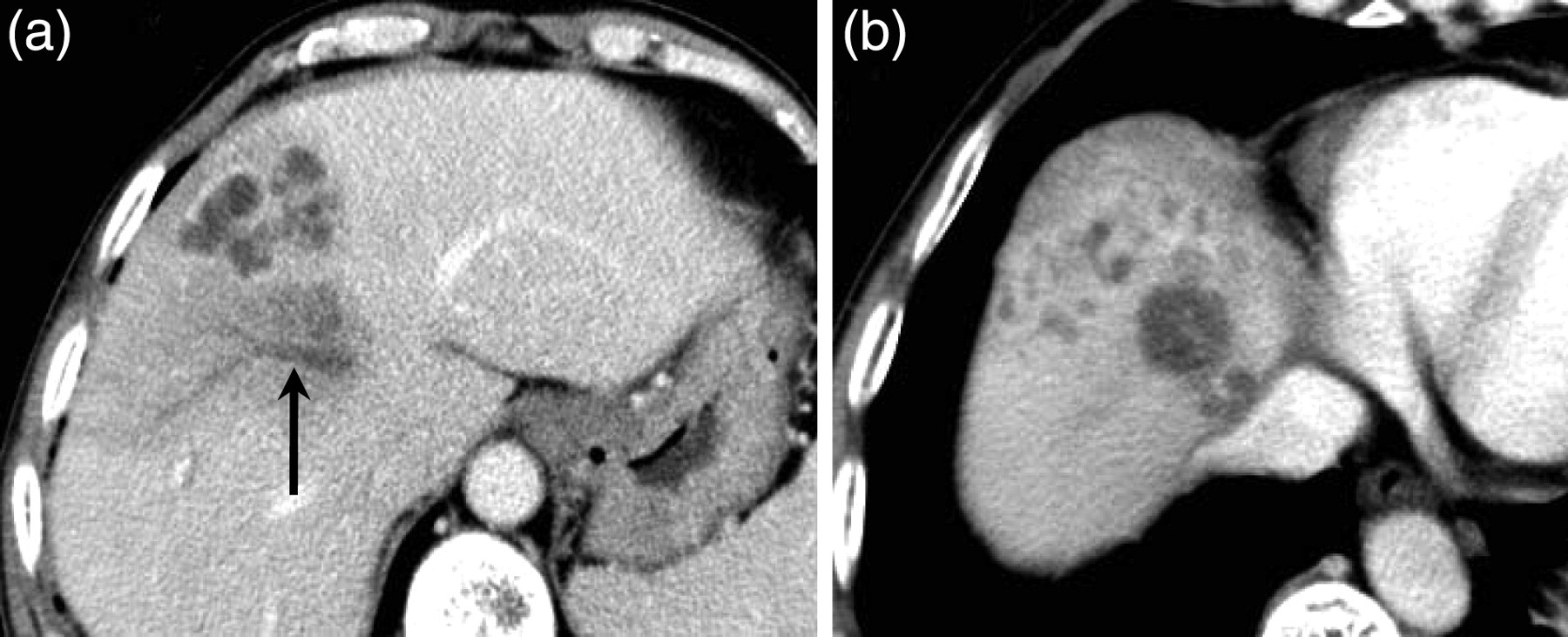
On the MRI examinations of five patients, MRI showed faveolate T1 hypointense and T2 hyperintense areas of the liver parenchyma with rim or peripheral enhancement. Nodular or circular hyperintense materials were found scattered in the lesions on T1-weighted imaging (T1WI) (Figs. 4 and 5).
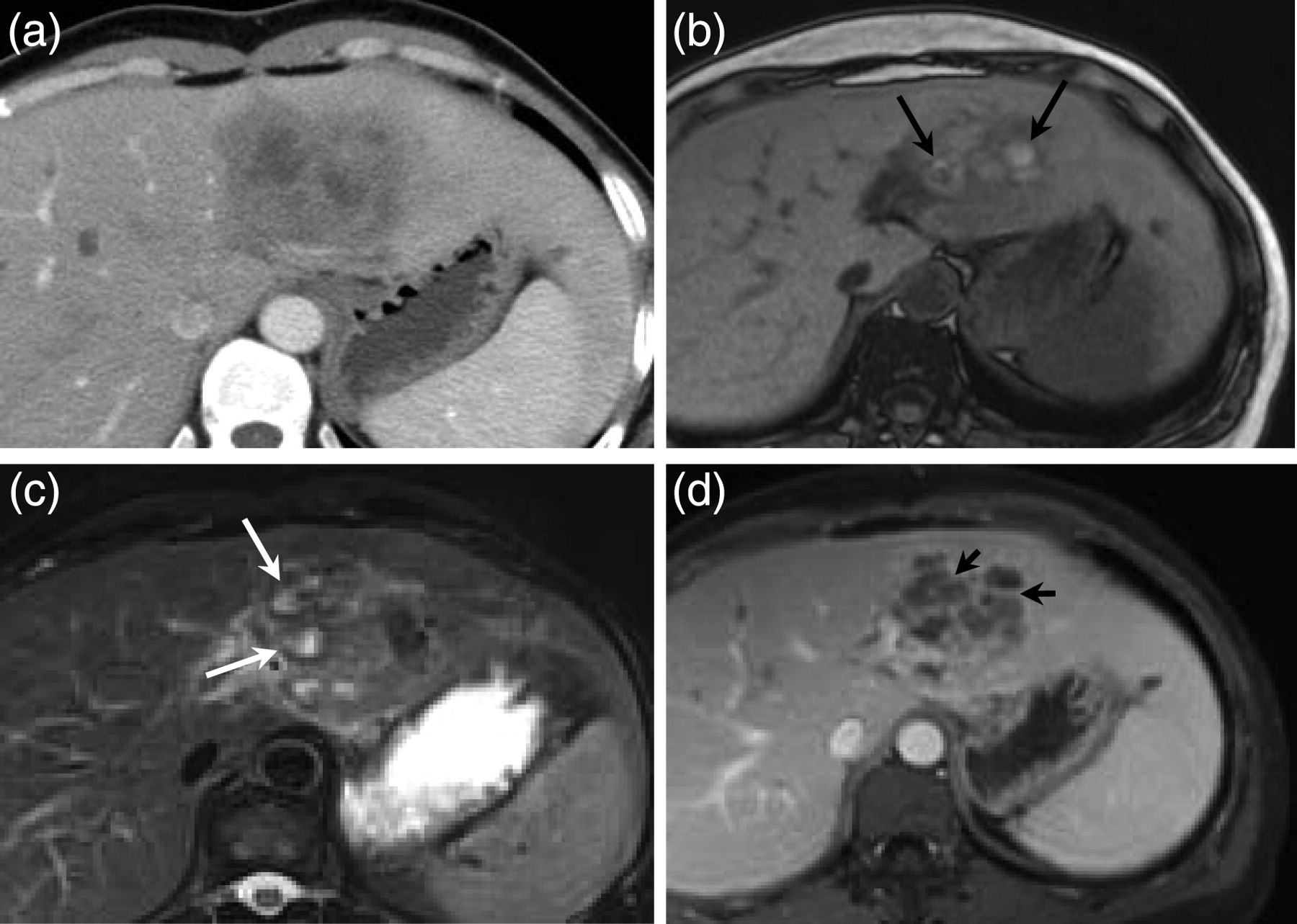
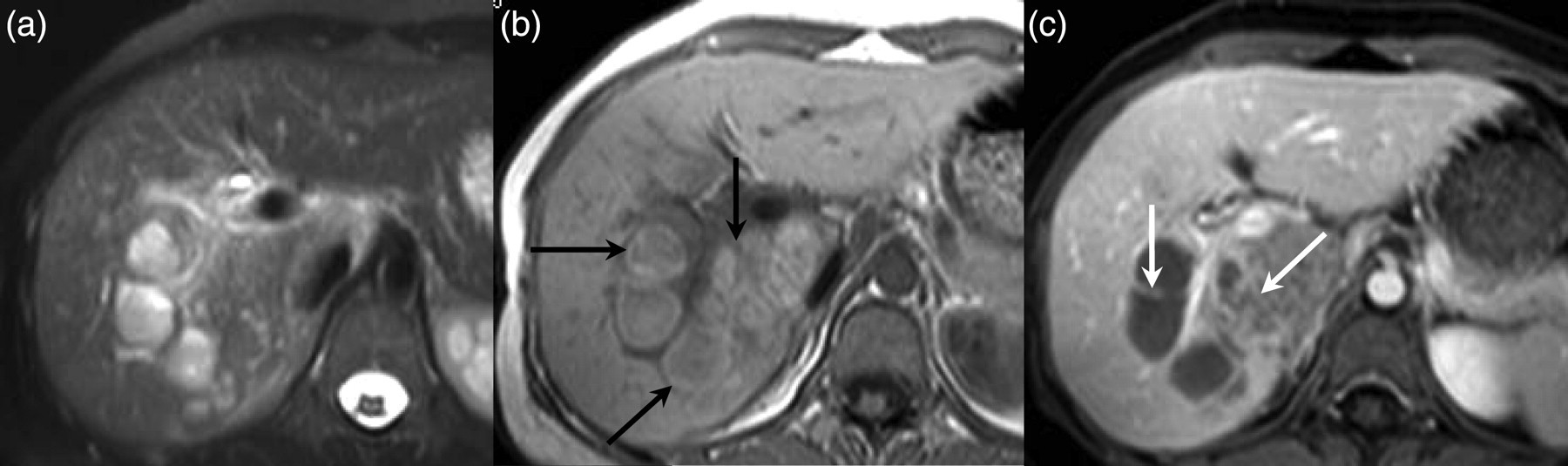
HP, 44-year-old woman. Enhanced CT image (a) shows an irregular mixed low-density lesion located in the left lobe of the liver. MRI demonstrates a low signal intensity lesion on T1WI, with nodular or circular hyperintense materials scattered in the lesions (b, black arrow) at the same sites as on CT, ill-defined slightly hyperintense areas of the liver and hyperintense nodular lesions with low signal ring on T2WI (c, white arrows), and circular and peripheral enhancing on contrast-T1WI (d, arrow)
HP, 35-year-old woman. MRI shows faveolate T2 hyperintense lesions located in the right lobe of the liver parenchyma (a), nodular or circular hyperintense materials scattered in the lesions on T1WI (b, black arrow), and rim or peripheral enhancement (c, white arrow)
Surgical and microscopic findings
The operative findings in the liver were as follows: the sizes of the masses ranged from 2.0 cm to 12 cm, and the masses were firm or cystic-firm mixed, irregular, or lobulated. The masses were yellowish or white-colored after dissection and after tawny fluid had flowed out.
Microscopic examination of the lesions of all patients showed the formation of extensive, irregular cave-like or tunnel-shape chronic eosinophilic abscesses accompanied by punctate calcification. Numerous eosinophils, coagulation necrosis debris, and Charcot-Leyden crystals were found in the centers of the lesions, and granulomatous inflammation and/or granulomas were found around the abscesses. The deposition of paragonimiasis eggs in the eosinophilic necrosis was found in seven patients.
Discussion
Paragonimus species are distributed globally. Infection in humans is the result of a complex transmission cycle that includes two obligate intermediate hosts, a snail and a crustacean or a crayfish, and a final mammalian host (2, 3). Humans usually acquire the disease by ingesting uncooked freshwater crab or crayfish (4). However, in our study, there were only eight (38.1%) patients with a history of ingesting uncooked freshwater crab or crayfish within the previous 6 months. Paragonimiasis classically presents with pulmonary manifestations as a result of the migration of the juvenile worms. Ectopic infection may occur and most commonly involves the brain and subcutaneous tissue (5). HP is rare although, there has been a worldwide increase in human HP in the last decade, especially in endemic areas.
The symptoms of HP are usually variable and non-specific, such as chronic abdominal pain in the right upper quadrant or back pain, and may remain asymptomatic until the HP is discovered incidentally. Therefore, the diagnosis of HP can be difficult, especially in non-endemic areas, and many diseases must be excluded in the differential diagnosis. Peripheral eosinophilia with a differential count and abnormal liver function tests can be found in most patients. Elevation of AFP is rare, and we reported one case in our study (the patient was initially misdiagnosed as hepatic carcinoma). The cause of the AFP elevation in that case is not yet known.
Although the precise diagnosis of paragonimiasis should be based on detecting eggs in sputum and/or stool or parasitology antibody tests (6, 7), radiologic findings are specific and facilitate an accurate diagnosis. According to Hu, Lee, and Kim (1, 7, 8), the parasites penetrate the intestinal wall and may migrate through the peritoneal cavity to the central liver parenchyma after perforating the Glisson sheath. Thus, lesions are initially located mainly at the subcapsular region on CT or MRI, and this finding seems to be characteristic of hepatic paragonimiasis.
Because of the migration of the parasites, CT images showed multiple mixed hypodense lesions accompanied by tunnel-shaped microabscesses, and MRI showed faveolate T1 hypointense and T2 hyperintense lesions, which correspond to the extensive, irregular cave-like chronic eosinophilic abscesses observed on the microscopic examination. Granulomatous inflammation and/or granulomas around the abscesses, as observed on the microscopic examination, were responsible for the separate irregular rim or circular enhancement of the lesions on contrast CT and MR images, which is similar to the findings reported by Hu et al. (1, 9, 10). In invasive paragonimiasis, the parasites migrate through the hepatic parenchyma, invade the bile duct and cause chronic cholangitis. In our study, seven patients had a mildly dilated bile duct. Some nodular or circular hyperintense materials were found scattered in the lesions on MR T1WI. We presumed that the numerous coagulation necrosis debris and the Charcot-Leyden crystals caused these hyperintensities.
The differential diagnoses for low-attenuating, tubular, or mass lesions with peripheral enhancement in the liver include pyogenic abscess, cholangiocarcinoma (CCA). The key points for the differential diagnosis are as follows: most of the pyogenic hepatic abscesses are usually solitary, are located in the right lobe of the liver, and coalesce to form a large abscess cavity, especially without treatment, which results from the disintegration and necrosis of hepatic tissues by suppurative infection (11–13). The walls of liver abscesses are inhomogeneously thickened, obviously enhanced and are accompanied by apparent hyperemia reaction and edema of surrounding liver tissues. However, inflammation and hyperemia of surrounding liver tissues in HP are not common on arterial or portal-phase enhanced CT or MRI. Because inflammation and hyperemia occurred in only three patients in our study, we presume that this atypical appearance may be caused by the chronic processes of HP. Intrahepatic cholangiocarcinoma (CCA) is the second most common primary hepatic tumor and derives from the epithelial cells of the bile ducts. On CT, mass-forming intrahepatic CCA usually appears as an inhomogeneous low-attenuation mass with irregular peripheral enhancement and can be accompanied by satellite nodules, peripheral intrahepatic duct dilatation, and periductal thickening (14, 15). CCA may also involve the vascular system, invade local lymph nodes or metastasise regionally or distantly (16). However, vascular and lymph node involvement are rare in HP. Because fascioliasis and paragonimiasis are both caused by flukes, their radiological manifestations are similar and their final diagnosis depends on the histopathologic results.
This study has some limitations. First, this retrospective study fails to provide more characteristic information with regard to the CT findings that are already known. Second, a small number of patients underwent MR examination; therefore, the MRI findings we observed and the presumptions we made need to be confirmed in large, prospective imaging-specimen comparative studies.
In conclusion, HP is a rare disease, but it may have some distinctive CT or MR imaging findings in the liver, as observed in our patients. For patients with eosinophilia and abnormal liver function, with or without right upper abdominal pain, imaging of the liver parenchyma may provide diagnostic clues, especially in endemic areas, and help avoid unnecessary and invasive procedures such as biopsy and surgery.