
Abstract
Background
Today's gold standard for diagnostic imaging of inflammatory diseases of the paranasal sinus is computed tomography (CT).
Purpose
To evaluate diagnostic sensitivity and radiation dose of an ultra-low dose dual-source CT technique.
Material and Methods
Paranasal sinuses of 14 cadaveric heads were independently evaluated by two readers using a modern dual-source CT with lowest reasonable dosage in high-pitch mode (100 kV, 10 mAs, collimation 0.6 mm, pitch value 3.0). Additionally the head part of an anthropomorphic Alderson-Rando phantom was equipped with thermoluminiscent detectors to measure radiation exposure to the eye lenses and thyroid gland.
Results
Diagnostic accuracy regarding sinusoidal fluid, nasal septum deviation, and mucosal swelling was 100%. Mastoid fluid was detected in 76% and 92%, respectively. In the phantom study, average measured eye lens dosage was 0.64 mGy; radiation exposure of the thyroid gland was 0.085 mGy.
Conclusion
Regarding evaluation of inflammatory diseases of the paranasal sinus this study indicates sufficient accuracy of the proposed CT protocol at a very low dosage level.
Inflammatory diseases of the paranasal sinus have a relatively high prevalence in younger patients and often need antibiotic treatment, sometimes even surgical intervention (1, 2). Over the past decades, radiation-based imaging of the paranasal sinuses has evolved from plain X-rays to cross-sectional imaging by computed tomography (CT). CT has become the gold standard of diagnostic imaging providing sufficient spatial resolution while its data-set can be used for computer-assisted endoscopic sinus surgery (3, 4). However, CT in general is known to be responsible for most of the collective medical radiation dose of the population in modern societies (5). Regarding imaging of the paranasal sinuses, it is important to emphasize radiation sensitive tissue like eye lenses and the thyroid gland, because they get radiated by direct or scattered X-rays during the examination.
Since this patient collective is mostly of lower age and repetitive examinations might be done during follow-up examination, an increased balance in dosage of routine protocols is required. Over the past years efforts to lower radiation exposure have focused on reducing tube voltage and current (3, 6). This approach has been successful due to the high contrast in density of the paranasal air filled spaces to the surrounding bony structures.
The simultaneous use of two approximately 90° shifted X-ray tubes in CT (dual-source technology) is now in its second generation. Dual-source modes now allow pitch values up to 3.2 acquiring a gapless data-set and reliable image quality for various indications (7–10). Among a decreased examination time the high-pitch mode allows tube current values as low as 4 mAs. Such low tube currents should cause a consecutively diminished radiation exposure. Despite an expected increase in image noise, ultra-low tube current settings might still be worthwhile for sinus imaging when looking for inflammation. The proposed study examines the diagnostic value and radiation dose using an ultra-low dose CT protocol when examining the paranasal sinus.
Material and Methods
Examination technique
Using the proposed CT device (Somatom Definition Flash, Siemens, Erlangen, Germany) the skulls of 15 corpses were examined for this study. Local ethical board agreement was obtained prior to this project. A total of six examinations were conducted upon every cadaver with various tube voltage and current preferences (120 kV/50 mAs, 120 kV/20 mAs, 120 kV/4 mAs, 100 kV/20 mAs, 100 kV/10 mAs, 100 kV/4 mAs). Dual-source technique with increased table feed was always activated (pitch value 3.0). Collimation was 0.6 mm, rotation time set to 0.28 s and scan length between 12 and 14 cm according to varying anatomic dimensions. In detail the examination ranged from the roof of the frontal sinus to the maxillary sinus with the upper jaw being aligned to the gantry to minimize dental artifacts. The field of view was adapted to cover the paranasal sinuses, facial bones, and the mastoid region. The following multiplanar reconstructions were made from raw data: 3-mm slices with 3-mm image distance in transversal (bone and soft tissue kernel) and coronal view (bone kernel). Fig. 1 shows axial and coronal reformations of the different examination protocols. To assess image noise of every data-set, a ROI (region of interest) with a diameter of 10 mm was placed in air outside the skull at level of the maxillary sinus. ROI measurements took place on the axial bone kernel images; they were repeated twice and the mean result was noted. Measured standard deviation of Hounsfield units (HU) was used as noise ratio index.

Axial and coronal reformations (slice thickness 3 mm, increment 3 mm) of the same skull using the various examination-protocols. Coronal view is shown in bony windows with hard kernel; transversal images are calculated with a soft kernel and shown within soft tissue window. A polypoid swelling is located in the left sphenoidal sinus, fluid level is located in the left maxillary sinus (*marks the chosen ALARA-protocol). Note: The displayed pneumocephalus is a usual finding in cadavers
Evaluation of image quality and diagnostic validity
First the minimum acceptable image quality of the six dose protocols was identified by the authors in consensus on a single image set that did not contain any pathology. To preserve accurate diagnostic information, clear identifiability of the following anatomic landmarks was necessary: ostiomeatal complex (nasal outflow tracts of the paranasal sinus), septal branches of the ethmoidal sinus, crista galli, nasal conchae, course of the internal carotid artery and optical nerve next to the sphenoidal sinus, canalis infraorbitalis as well as a coarse overview of mastoid cells. In addition, sufficient tissue contrast within the orbital cavity had to be visible within the soft kernel images. As a consequence from the previous evaluation of the six dose protocols the examination using 100 kV/10 mAs was chosen as ALARA protocol (as low as reasonable achievable). Using a standard diagnostic monitor two readers (with 2 and 10 years of experience) evaluated the image sets of the remaining 14 cadavers independently using the proposed ultra-low dose technique. The following relevant radiological criteria regarding a possible inflammation of each sinus were focused on: sinusoidal fluid, circumferential or polypoid mucosal swelling within a paranasal sinus. Mucosal swelling was defined ≥2 mm in diameter, fluid level was defined over 3 mm. Regarding ethmoidal and mastoid cells a minimum of two obliterated cells were evaluated as a positive finding. Furthermore, important anatomic variants like pneumatization of the middle turbinate (concha bullosa), deviation of nasal septum, and the course of the internal carotid artery within the sphenoid sinus were noted. Among these typical alterations of the paranasal spaces occurring with rhinosinusitis all other pathologies detected by the readers were also noted to verify general diagnostic sensitivity of the protocol.
Subsequent to the CT examinations an autopsy was conducted upon the heads and the findings were used as gold standard to evaluate accuracy of the low dose protocol.
Radiation measurement
The anthropomorphic Rando phantom (The Phantom Laboratory, Salem, NY, USA) was utilized to determine radiation exposure of the chosen ALARA protocol. The first 25 slices were used which contain the anatomic head and neck region and thyroid gland. Pre-calibrated lithium-fluoride thermoluminiscent dosemeters (TLD, The Harshaw Chemical Company, Cleveland, OH, USA) were placed in boreholes of predefined anatomic regions. The TLDs were irradiated five times in order to achieve a significant dosage. After pre-annealing the rods at 100°C for 10 min, they were read out with a dedicated TLD-analytical aperture made by the same manufacturer as the TLDs. Finally each measured result was divided by 5 to achieve the average boreholder dose.
Results
By decreasing tube current and voltage the image noise increases considerably (Fig 2). Using the examination protocol with a tube voltage of 120 kV at a current of 50 mAs, the lowest standard deviation of 34 HU was measured. The greatest image noise was measured using a setting of 100 kV and 4 mAs with an average image noise of 126 HU while the chosen ALARA examination protocol had an average measured standard deviation of 86 HU.
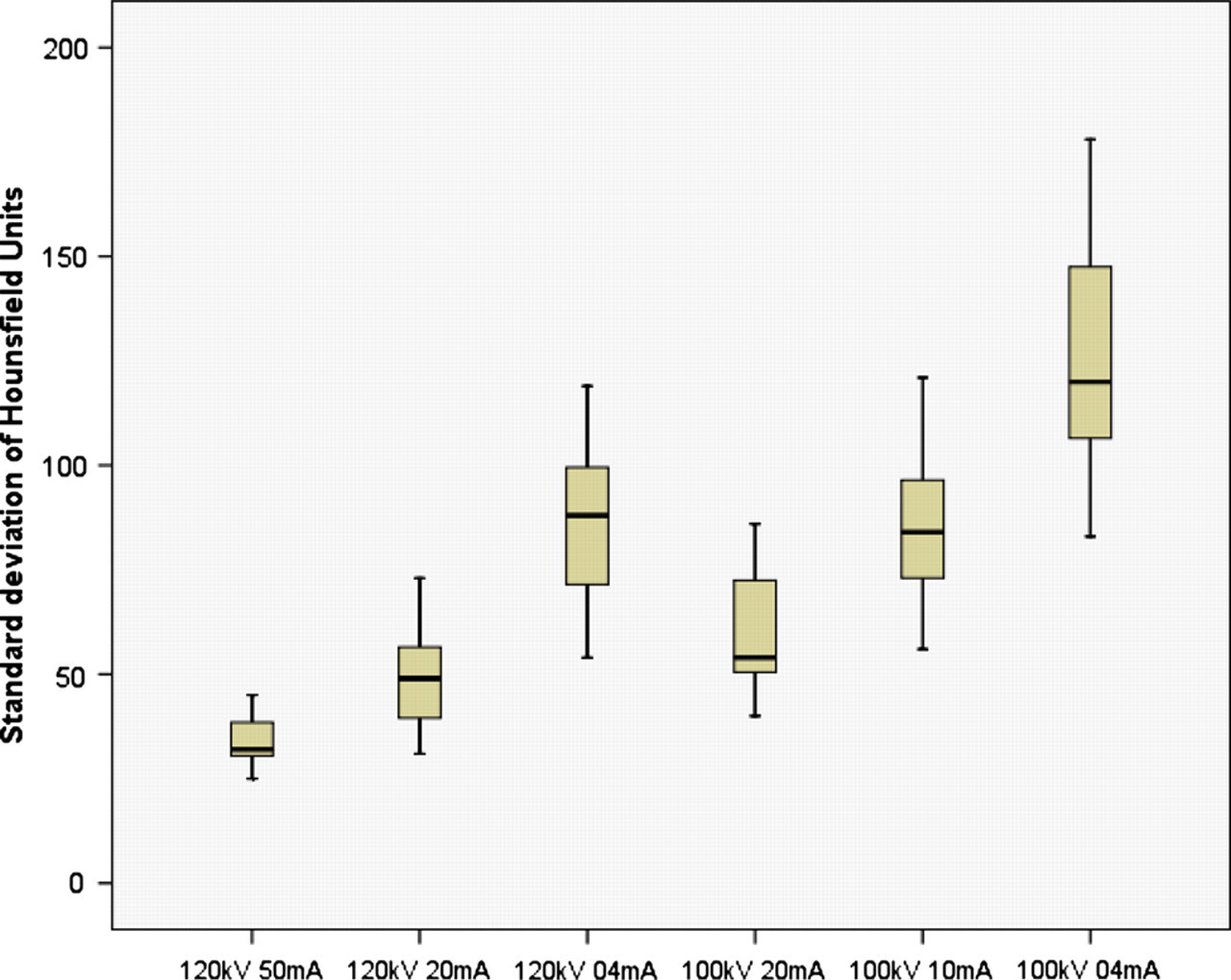
Image noise in relation to dose preferences measured in air
Derived from the autopsy a total number of 50 sinusoidal cavities of the 14 skulls had positive findings of fluid levels (Table 1). Sinus fluid was found most frequently in the maxillary sinus (16 cases) followed by the frontal sinus where fluid could be found 11 times. Eight cases had nasal septum deviation, fluid-filled mastoid cells were found 13 times. One skull had a non-dislocated fracture of the right temporal bone, and in another case a displaced fracture of the zygomatic arch could be found. Regarding typical morphological signs for rhinosinusitis the pathologies were identified correctly in all cases by using the proposed dual source high-pitch technique. Septum deviation as a possible cause for chronic inflammation of the paranasal spaces was also identified in all skulls. Reader 1 (2 years of experience) failed to detect fluid-filled mastoid cells three times and concha bullosa in two cases. Furthermore the less experienced reader did not detect the non-displaced temporal bone fracture.
Total number of pathologies found in the autopsy and positive findings of two readers by using the ALARA protocol
The phantom measurements regarding radiation were 0.67 mGy for the left eye lens, 0.61 mGy for the right lens, and 0.12 (resulting in an average exposure of 0.64 mGy), respectively, 0.05 mGy for the superior and inferior portions of the thyroid gland, resulting in an average exposure of 0.085 mGy (Table 2). Radiation of the different brain levels was 0.34–0.56 mGy.
Measured dosage of the proposed dual source high-pitch CT examination protocol by using the head part of a TLD equipped Alderson phantom
Discussion
Our results indicate that the proposed ultra-low dose dual-source protocol has sufficient diagnostic validity while causing only minimal radiation exposure to the patient. Mucosal swellings as well as fluid levels within the paranasal sinus were nearly completely identified by both readers. Regarding detection of rhinosinusitis the sensitivity of even discrete findings was 100%, implying a safe use for daily clinical practice. Important anatomic variants that may have influence for therapeutic management were also found frequently. The detection rate of both fractures as well as possible signs for mastoiditis was slightly lower with the ALARA protocol compared to finding sinusoidal inflammation, especially by the less experienced radiologist. Despite the fact that the reader could identify the few pathologies after they were pointed out to him, the diminished sensitivity could be a consequence for a relatively underpowered examination regarding tube current.
When using the proposed ALARA protocol a higher image noise seems to be the logical consequence for the low amount of photons used for image acquisition. Yet in our study this did not limit diagnostic validity of sinusoidal spaces which are characterized as high-contrast tissue. Discrimination of tissue with similar density (e.g. musculature versus tumor tissue) could be insufficient and lead to false-negative diagnoses; however, this has to be further researched. The clinical tradeoff dose vs. image quality, known as the second risk of radiation has to be kept in mind when choosing lowest dose parameters in particular examinations (11, 12). Regarding postoperative routine status of osteosynthesis material in the facial region the proposed protocol might as well be underpowered causing an increased amount of beam hardening artifacts; however, no data are available yet. For now the authors recommend using the proposed examination protocol solely when excluding rhinosinusitis.
Radiation exposure
Regarding the proposed ALARA protocol, only marginal dose values were measured. While eye dosage was 0.64 mGy the average exposure to the thyroid gland was as low as 0.085 mGy. Interestingly, measured radiation to both eye lenses differed in 0.06 mGy while TLDs of both sides of the cerebrum showed 0.03 mGy in dose difference. Apart from being a result of X-ray tube positions, this could also indicate a certain impreciseness of the utilized TLDs within these ultra-low radiation values. Further measurements with different head positions and tube current could help to verify these differences.
According to the International Commission on Radiological Protection (ICRP) radiation-induced cataract is scientifically based on a deterministic level (absolute threshold) with an exposure of 0.5–2 Gy on a short-term base (13). This value cannot be achieved with the proposed examination technique if appropriately administered, even with repeated examinations. The risk of radiation induced malignant neoplasms of the thyroid gland is based on a stochastic risk, which is stated to be 0.0075 per Gray (14, 15). With regards to the phantom measurements the stochastic risk to induce thyroid cancer after being examined with the proposed ALARA protocol would be negligible even after multiple follow-up CTs. Furthermore the use of an appropriate shielding, like a lead neck collar, could further decrease radiation exposure to nearly zero although there might still be a relevant amount of scattered radiation induced the skull itself.
Alternative imaging modalities
Cone-beam computed tomography (CBCT), primarily introduced for orthodentic indications, as an alternative image modality is ought to have reasonable diagnostic value for diagnostic of rhinosinusitis (16, 17). According to the literature CBCT is ought to have great advantage over multislice CT concerning radiation exposure (18–20). Compared to these former single source sinus CT studies eye dosages of the proposed protocol is lower by factor 19 to 23. Even more drastic is the difference in dose of the thyroid gland caused by scattered radiation, which are 30–130 times higher compared to our protocol. However, it has to be stated that the CT devices used in these studies are technically outdated or the examinations were set up with an over-assessed tube voltage and current seen from a today's perspective. Schell et al. utilized the same high-pitch technique for evaluation of sinusitis and found diagnostically conclusive image quality (10). On the contrary, our study shows successful imaging of this region with dose preferences that are certain magnitudes lower.
Our proposed dual-source high-pitch CT protocol caused radiation doses to the lens that were mostly lower or equivalent to the CBCT values provided by the literature. Future studies with optimized CBCT parameters and direct comparison of signal to noise ratio to low dose CT studies are necessary to judge photon effectiveness.
Though monetary reasons may induce to request plain X-ray images for rhinosinusitis indications, the overall low diagnostic validity should be pointed out to the clinicians (21, 22). The authors agree with the general view of the literature that evaluating the complex anatomy of the paranasal sinus cannot be sufficiently done with projection radiography and therefore should be avoided whenever possible.
Theoretically magnetic resonance imaging (MRI) can also be used for exclusion of inflammatory sinusoidal disease. However, due to a diminished visualization of bony structures, increased costs, and longer examination time the use of that image modality would be an exceptional case.
Compared to the literature our results show an impressing advantage in dose reduction by utilizing an adapted dual source high-pitch examination technique. The ultra-low tube current preference caused only little radiation exposure compared to other sinus CT studies. Due to the increased table feed, the examination time is consecutively diminished to under a second. For non-compliant patients, this technique could conceivable provide images with less motion degradations. The authors use the proposed examination protocol successfully as standard screening technique to diagnose rhinosinusitis in patients without any surgical history of the sinus.
In conclusion, modern CT devices permit a significant amount of preferences, making it necessary to develop dedicated examination protocols for special indications. While the proposed ultra-low dose examination protocol can easily be used as a screening method for inflammation of the paranasal sinus, tube current preferences should be carefully evaluated for different clinical indications in the same anatomic region.