
Abstract
Background
Despite its long history, the application of N-butyl cyanoacrylate (NBCA) has been limited compared to other materials such as particulate agents and coils. This possibly owes to a widespread misconception that NBCA is difficult to handle and carries a high risk of complications due to its liquid nature and rapid polymerization time. However, recent reports have shown that, with knowledge and experience, NBCA is safe and effective to use in visceral arteries.
Purpose
To review the outcome of transcatheter embolization of the renal artery using NBCA for varied etiologies in the kidney.
Material and Methods
Fourteen patients with varied etiologies in the kidney underwent renal artery embolization using NBCA as the sole embolic agent (64%) or in combination with an additional embolic material (36%). A review of medical charts and images were performed to gather information regarding underlying etiologies, clinical presentation, and outcome of embolization.
Results
Technical success was achieved in all patients (100%) while clinical success was achieved in 12 (85.7%). One failed case was managed by repeat embolization using microcoils, while the other underwent partial nephrectomy after failed reattempt at embolization. Three patients with recurrent bleeding after previously having undergone embolization using microcoils or gelatin sponge particles were successfully managed the second time using NBCA. NBCA embolization was also effective in three patients with hemostatic abnormality. Complications attributable to NBCA embolization were renal atrophy in one patient and microcatheter tip fracture in another.
Conclusion
The application of NBCA for transcatheter embolization of varied etiologies involving the renal artery is feasible and safe in the hands of an experienced interventional radiologist. It offers immediate and effective occlusion of the pathologic vessel and, while it can be used exclusively on its own, it can also be used to complement other embolic materials.
During the recent years, the application of N-butyl cyanoacrylate (NBCA) glue – a liquid adhesive – for transcatheter embolization has been steadily increasing and has secured a role in many institutions as the primary embolic material for endovascular management of varied vascular pathologies ranging from acute visceral hemorrhage to arteriovenous malformations (AVM) (1–4). More recently, numerous articles in literature have described the effective use of NBCA in visceral pseudoaneurysms (5–10). NBCA offers immediate occlusion of the vessel and, compared to the more commonly advocated microcoils, it can be delivered far distal to the delivery catheter owing to its conformable nature. Furthermore, the potential use of NBCA as a complementary embolic material to others such as coils has broadened its range of use. This retrospective review focuses on our experience with NBCA in transcatheter embolization of renal arteries over the past six years, where we have found it to be safe and effective in experienced hands.
Material and Methods
Patients
An approval by the institutional review board was sought for this study, and the requirement for informed consent was waived. We retrospectively analyzed our database of patients who underwent transcatheter embolization using NBCA from August 2005 to July 2011 revealing a total of 173 patients (Table 1). Among this group, NBCA embolization of the renal artery was performed in 14 patients (10 men and 4 women; mean age 58.2 years, range 40–75 years). In a single procedure, NBCA was used exclusively on its own in nine patients (64%), including three patients who had previously undergone embolization using gelatin sponge particles (Gelfoam) or microcoils. In five patients (36%), NBCA was used to complement other embolic material (microcoils in four patients and vascular plug in one). Medical charts and computed tomography (CT) images were reviewed to gather information regarding underlying etiologies, clinical presentation, and outcome after embolization. Laboratory data associated with hemostasis such as platelet counts and international normalized ratio (INR) were assessed, and medical history was reviewed to find out if any patient was under antiplatelet or anticoagulant therapy.
Clinical characteristics and outcome of NBCA embolization in the renal artery in 14 patients
RA = renal artery, PNL = percutaneous nephrolithotripsy, PCN = percutaneous nephrostomy, RCC = renal cell carcinoma, CRF = chronic renal failure, AVF = arteriovenous fistula, AVM = arteriovenous malformation, AML = angiomyolipoma, INR = international normalized ratio, PLT = platelet count (×104), N = within normal range
Embolization technique
Transcatheter embolization was performed by six board-certified radiologists with 5 to 26 years of clinical experience in endovascular therapy. The right common femoral artery was routinely accessed and after selecting the right or left renal artery using a 0.035-inch hydrophilic guidewire (Radifocus; Terumo, Tokyo, Japan) and standard 5-F catheter, renal arteriography was performed. “Target” vessels for embolization were determined on digital subtraction angiography (DSA) by identifying extravasation of contrast medium, pseudoaneurysm, or, in case of an arteriovenous malformation (AVM), abnormal feeding arteries to the nidus. A microcatheter was advanced into all identifiable target vessels, which were subsequently embolized using NBCA (Histoacryl, B. Braun, Melsungen, Germany) alone or in combination with another embolic material such as coil or vascular plug. The selection of embolic material was made on a case-by-case basis based upon the decision of the interventional radiologist at the time of the procedure. With respect to the technique of NBCA embolization, a microcatheter was advanced as close to the site of vascular abnormality as possible, after which manual test injection of contrast medium was performed to confirm correct positioning of the microcatheter. Furthermore, in order to prevent backflow of NBCA that could consequently lead to inadvertent embolization of non-target vessels and to minimize the risk of distal embolization, adequate dose and injection rate of NBCA was estimated by simulating the procedure with manual injection of contrast medium. Depending on the distance from the tip of the microcatheter to the target lesion and rate of blood flow through the vessel, NBCA was diluted with iodized oil (Lipiodol; Andre Guerbet, Aulnay-Sous-Bois, France) at a ratio between 1:2 and 1:4. Before injecting the NBCA mixture, the microcatheter lumen was flushed manually with Dextrose 5% in water (D5W) in order to prevent early polymerization of NBCA upon contact with blood within the microcatheter. Thereafter, the NBCA mixture was carefully injected, at the same time, checking that there was no reflux into non-target vessels. The microcatheter was immediately removed after administration of NBCA mixture in a single quick motion before the tip of the microcatheter could adhere to the blood vessel. In some cases, the “sandwich” technique was applied where the microcatheter lumen was flushed with D5W before and after NBCA administration prior to removing the microcatheter. Re-utilization of the microcatheter was made possible by flushing the lumen a second time with D5W. When necessary, embolization was either repeated with additional doses of NBCA or complementary use of other embolic materials. In all cases, a final arteriogram was performed to confirm successful occlusion of the target vessel.
Evaluation of outcome and follow-up
Technical success was achieved by complete occlusion of the bleeding vessel or exclusion of the pseudoaneurysm, which were no longer opacified on immediate post-embolization angiography. Clinical success was achieved with resolution of presenting symptoms without the need for further intervention or surgical procedure.
The outcome of the procedure was assessed by reviewing changes in the patients' clinical status after embolization (including presenting symptoms, vital signs, laboratory data, and CT findings), and identifying any complications attributable to embolization. We also reviewed the long-term outcome of each patient who underwent follow-up in the outpatient clinic.
Results
The clinical characteristics of the 14 patients are summarized in Table 1. Technical success was achieved in all patients (100%) regardless of whether NBCA was used exclusively or in combination with an additional embolic material. Microcoils were the most commonly used embolic material (used in four patients) complementary to NBCA and were delivered through the microcatheter either before or after administration of NBCA. An Amplatzer® vascular plug (AGA Medical, Golden Valley, MN, USA) was used to complement NBCA in one patient (No. 6) who had developed bleeding from an angiomyolipoma in the right kidney after undergoing percutaneous biopsy.
Clinical success was achieved in 12 out of 14 patients (85.7%), where good outcome in 12 patients was reflected by resolution of presenting symptoms such hematuria, anemia, or hemodynamic instability (Figs. 1 and 2). In the two failed cases (No. 4 and 13), recanalization of previously-embolized vessels were demonstrated on follow-up DSA. One of these patients (No. 13), who had developed renal artery bleeding after percutaneous renal biopsy, underwent embolization using NBCA, and success was confirmed on follow-up CT. However, the patient returned to the angiography suite due to recurrent bleeding one day later and, upon discovering a recanalized hemorrhagic vessel, embolization using microcoils was performed with clinical success. The second patient (No. 4) demonstrated massive extravasation from a ruptured aneurysm associated with an arteriovenous fistula (AVF) on DSA (Fig. 3). A combination of NBCA and microcoils were used to occlude the aneurysm and its parent artery. After confirming technical success on post-embolization DSA, the patient was sent to the intensive care unit only to return the next day for re-intervention due to recurred signs of bleeding. Embolization was repeated using NBCA and coils after detecting persistent blood flow around previously-placed coils and, by accessing the right femoral vein, the venous side of the AVF was also occluded with NBCA and coils. A final DSA confirmed complete occlusion of the AVF without further evidence of contrast extravasation. However, the patient eventually underwent radical nephrectomy 11 days later owing to another episode of bleeding. With the exception of these two cases, the remaining patients presented with no further clinical abnormalities in relation to the treated vessels during a mean follow-up period of 15.4 months (range 1.2–60.1 months).
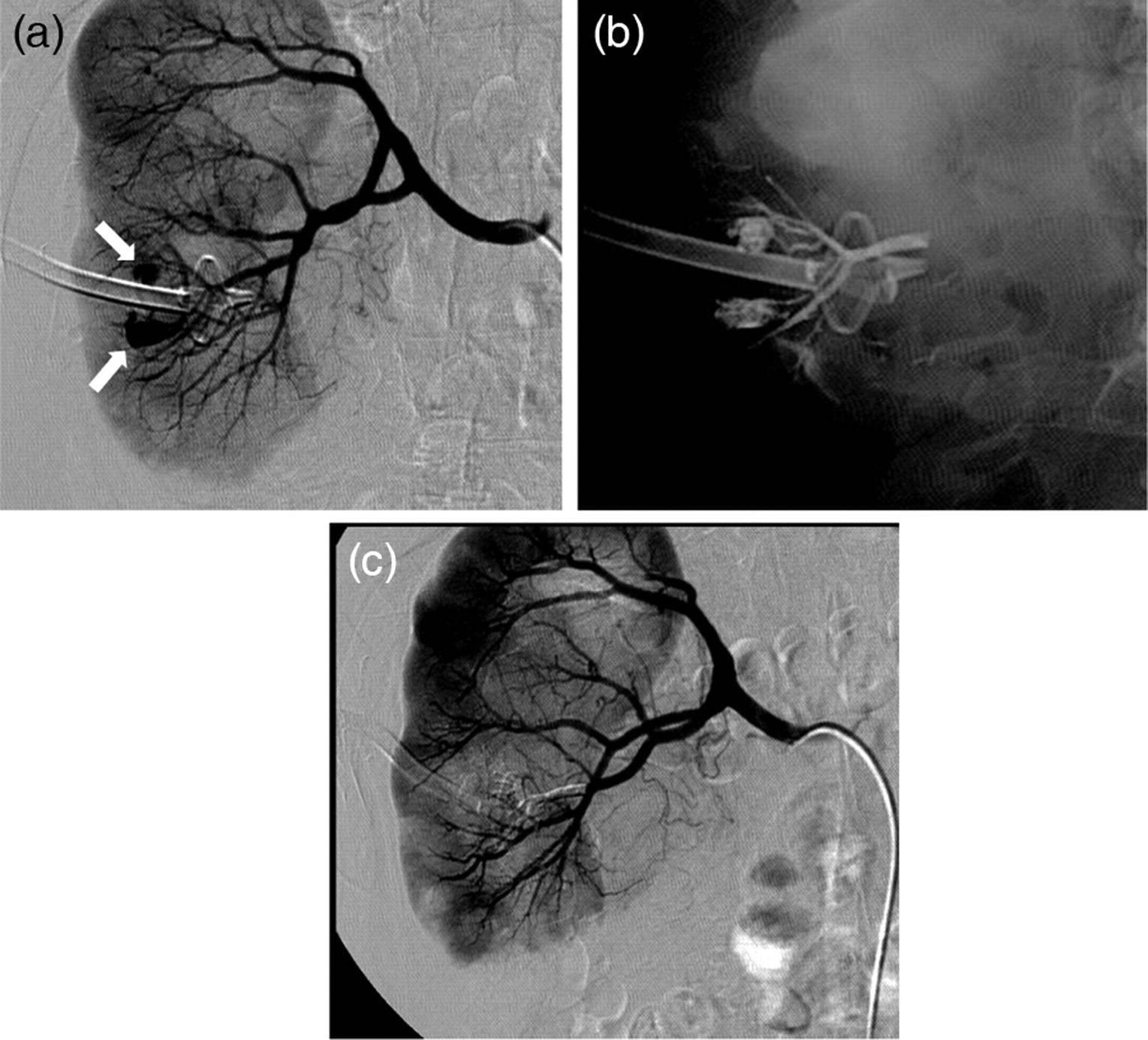
A 61-year-old male patient (No. 12) presented with hematuria after undergoing percutaneous nephrolithotripsy for a urinary stone in the right kidney. Arteriogram of the right renal artery (a) reveals two pseudoaneurysms (arrows) around the Malecot nephrostomy tube. A microcatheter was advanced into the branch harboring the pseudoaneurysms, after which embolization was performed using NBCA (b). The post-embolization arteriogram (c) confirms that the pseudoaneurysms and their parent artery have been successfully occluded. The patient was relieved from hematuria after embolization
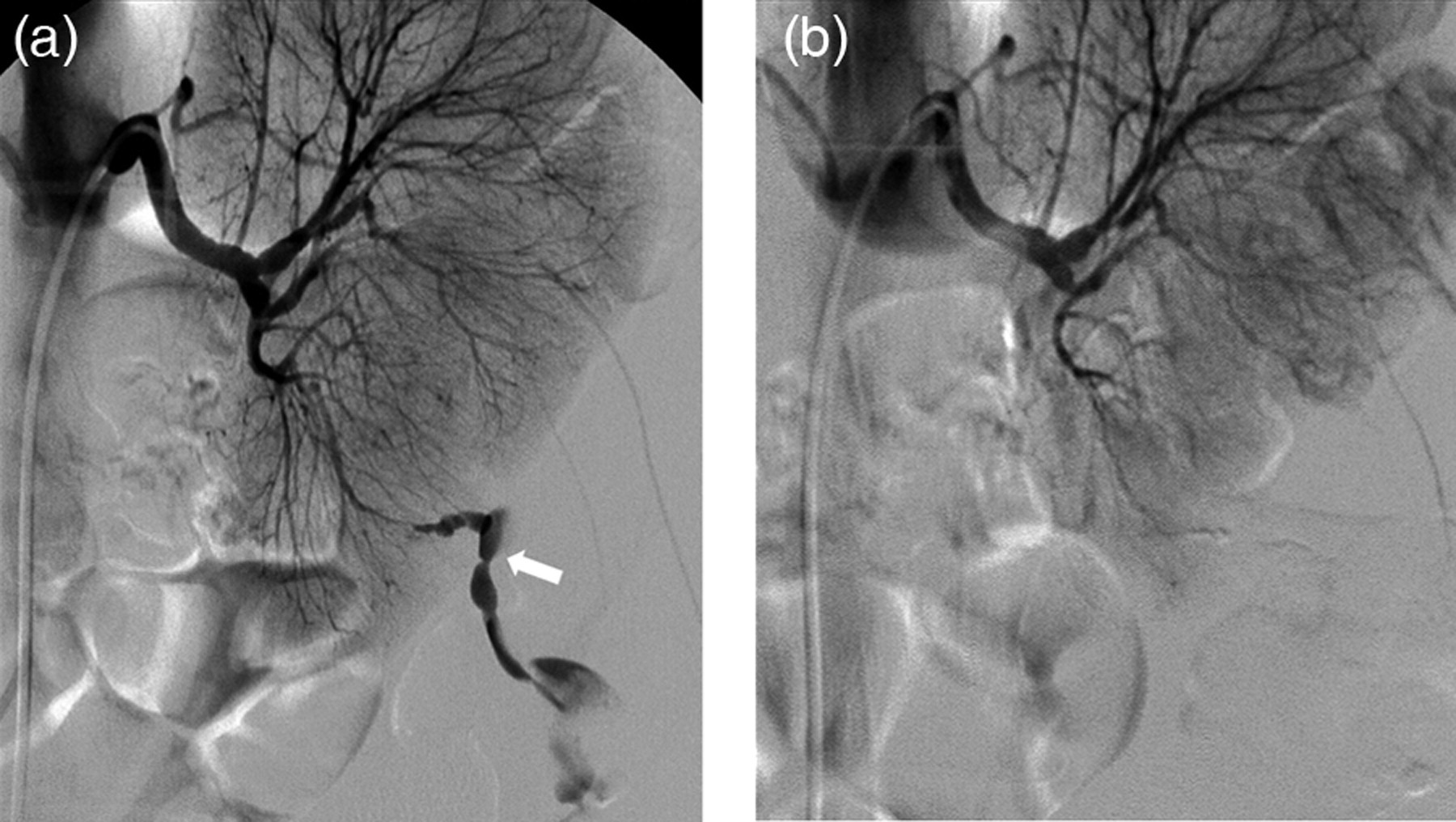
A 47-year-old female patient (No. 9) previously diagnosed with diffuse large B-cell lymphoma involving bilateral kidneys presented with left flank pain, decreased hemoglobin (5.3 g/dL) and hematocrit levels (16%), and hemodynamic instability (blood pressure 80/50 mmHg). Her INR was prolonged (1.8) due to chemotherapy. Arteriogram of the left renal artery (a) demonstrates active extravasation of contrast medium (arrow) in the lower pole of the left kidney. Selective embolization was performed using NBCA and success was confirmed on a final post-embolization arteriogram (b). After embolization, the patient become hemodynamically stable and was relieved from other symptoms

A 48-year-old male patient (No. 4) presented with bulging of the right flank, hematuria, and hemodynamic instability. Arteriogram of the right renal artery (a, b) demonstrates a markedly dilated and tortuous artery leading to a ruptured aneurysm (white arrows in a and b). Note the small caliber of the descending aorta and left renal artery (black arrow in a) associated with hypovolemic shock. The patient underwent embolization with multiple microcoils and NBCA. An arteriogram repeated on the next day due to rebleeding demonstrated residual blood flow around previously-placed microcoils along with persistent filling of the aneurysm. Early venous drainage through the right renal vein and inferior vena cava (white arrows), consistent with features of AVF, is well-demonstrated (c). After embolizing the renal artery a second time with microcoils and NBCA, the right femoral vein was accessed (d) in order to embolize the venous side of the AVF with microcoils and NBCA (white arrow). Although the post-embolization aortogram (e) suggested a successful procedure, the patient eventually underwent radical nephrectomy of the right kidney 11 days later due to refractory bleeding
Three patients in our series had previously undergone embolization with either microcoils or gelatin sponge particles before undergoing NBCA embolization. Two of these patients had recurrent bleeding from previously-embolized vessels which were successfully occluded the second time with NBCA (No. 7 and 14). One of these cases (No. 7) involved a hemorrhagic transplant kidney in a patient who had previously been diagnosed with chronic renal graft rejection. Arteriography performed through the renal artery of the graft demonstrated multifocal bleeding foci for which embolization using NBCA was successfully performed following an initial attempt at hemostasis using gelatin sponge particles nine days earlier. The third patient (No. 10) who was diagnosed with an arteriovenous malformation (AVM) of the right kidney underwent a second embolization procedure using NBCA due to hematuria that was refractory to coil embolization of multiple feeding arteries performed 24 days previously. NBCA successfully occluded the remaining feeding arteries of the AVM.
Three patients had mildly prolonged INR which was associated with liver cirrhosis in one patient (No. 6), chemotherapy for lymphoma in another (No. 9), and sepsis superimposed on chronic renal transplant rejection in a third (No. 7). Among the three, the patient with liver cirrhosis (No. 6) was additionally found to have a low platelet count. No patients were under influence of anticoagulant and antiplatelet medication around the time of the procedure. Embolization with NBCA was technically and clinically successful in all of these patients.
There were two complications directly related to the procedure. The first one was global renal atrophy after embolizing multiple feeding arteries of a large AVM in the aforementioned patient (No. 10). The second one was associated with a fracture in the tip of the microcatheter during the process of embolization with NBCA (No. 5). The tip of the microcatheter fractured after adhering to the polymerized NBCA within the vessel. Although a small fragment of the catheter was retained within the patient's kidney, it did not cause any clinical problems during a follow-up period of 10 months.
For patients with follow-up CT images acquired after NBCA embolization, technical success was supported by findings such as resolution of contrast extravasation, pseudoaneurysm, or perirenal hematoma. Among the two failed cases, follow-up CT was available for one patient (No. 4). In this patient, post-embolization CT performed one day after the initial embolization procedure demonstrated persistent contrast enhancement of the AVF and aneurysm sac even though the post-embolization angiogram performed at the time of intervention suggested technical success.
Discussion
Transcatheter embolization of the visceral arteries is an attractive alternative to surgery and is now considered the gold standard treatment in a variety of situations because it is feasible and minimally invasive, while offering effective hemostasis. Numerous embolic materials are commercially available and each possesses its advantages and disadvantages. The choice of embolic material is usually made on a case-by-case basis, depending on various factors such as vascular anatomy and pathology, as well as personal preference of the interventional radiologist performing the procedure. Compared to the more commonly advocated metallic coils and particulates (such as gelatin sponge or polyvinyl alcohol particles), there has been limited use of NBCA in peripheral endovascular intervention. Recently, however, an increasing number of articles have focused on the use of NBCA for transcatheter embolization of various vascular pathologies ranging from post-traumatic bleeding to tumors and its range of application continues to expand (1–6, 8, 9, 11, 12). Kish et al. reported a successful hemostasis rate of 87.5% for transcatheter NBCA embolization of acute arterial bleeding (13). Their study shows that NBCA embolization can be effective even for hemorrhage recurring after embolization with gelatin sponge particles or coils. The main advantage of NBCA is that it is a liquid sclerosant that is capable of conforming within the vessel and occludes the vessel lumen rapidly. However, many interventional radiologists have avoided its use for the same reasons (inadvertent embolization of non-target vessels due to lack of control owing to its liquidity and, for some, quicker-than-desired rate of occlusion). As with any procedure, better control of the material comes with more experience, after which complications can be reduced while the results are enhanced.
Although transcatheter embolization of renal arteries has been described frequently in past literature, the renal artery was usually one among many other visceral arteries included within a single series (4, 6, 7, 9, 10). Meanwhile, few articles that have addressed the renal artery separately have presented the outcome of transcatheter embolization in the renal artery using a variety of embolic materials (14–17). A review of English literature disclosed only one article where embolization of the renal artery using NBCA was exclusively reviewed (18). The article describes five patients who had undergone NBCA embolization for management of traumatic intrarenal arterial pseudoaneurysms with successful outcome in all patients. In our series, we have exclusively focused on NBCA embolization of the renal arteries in 14 patients with varied underlying etiologies.
There were no technical failures in our series, which supports the suggestion in prior articles that transcatheter embolization with NBCA is feasible and effective. Regarding complications, such as inadvertent distal embolization and undesired embolization of non-target vessels due to backflow, we experienced none. This was most probably because the interventional radiologists who performed the procedures were familiar with the characteristics of NBCA through past experience. Global renal atrophy that occurred in one of our patients was a consequence of embolizing multiple feeding arteries supplying a large AVM over two sessions using microcoils and NBCA. One avoidable event did occur when the distal tip of the microcatheter adhered to the polymerized NBCA within the vessel and fractured as the catheter was pulled out. Although the catheter fragment was retained within the vessel, this did not affect the outcome of embolization nor did it cause any clinical problems during the follow-up period. Miscalculation regarding the ratio of NBCA mixture (high NBCA:Lipiodol ratio) or time to polymerization is suspected to have resulted in such an event.
Lipiodol is used for two reasons: first, to make the NBCA mixture radio-opaque and, second, to dilute the NBCA to the desired concentration depending on how much the interventional radiologist wants to prolong the time to polymerization (2, 5, 8, 11, 18, 19). A higher NBCA:Lipiodol ratio – by adding less amount of Lipiodol – offers quicker occlusion time while restricting time to inject the NBCA mixture through the catheter before it has to be removed. On the other hand, a lower NBCA:Lipiodol ratio will allow more time for injection while increasing the risk of distal embolization. Another important point to consider is the injection rate of NBCA mixture. Careless injection at a high rate will cause reflux of the mixture into non-target vessels exposing the end-organ to potential risk of infarction.
In our series, NBCA was used to complement microcoils in four patients. Neither our study nor any other in literature is able to confirm whether such a combination enhances the rate of vessel occlusion compared to the use of NBCA alone. However, the ability to use NBCA can become practical either when technical difficulties are encountered during placement of microcoils or when residual patency is observed after primarily embolizing the vessel lumen with microcoils. Such a scenario was encountered in one of our patients with a pseudoaneurysm (No. 8) whose tortuous vascular anatomy resulted in suboptimal positioning of the microcoil and residual blood flow in the target vessel. NBCA was administered through the microcatheter at the same location; however, this time, the NBCA mixture was successfully delivered to the site of the pseudoaneurysm. It has also been suggested that it is safer to use NBCA in combination with coils, for applying coils before administrating NBCA potentially reduces the risk of distal embolization by slowing down blood flow (10). In our experience, we believe this is partly true, especially in high-flow vessels. However, when the blood flow is not too rapid, NBCA embolization can be safely performed by using the correct NBCA:Lipiodol ratio. Furthermore, when performing a superselective procedure, wedging of the microcatheter tip within the vascular lumen is often possible in order to reduce pericatheter flow. This method decreases the risk of reflux of NBCA, thereby facilitating safe injection of NBCA (2).
The reason for clinical failure in two of our patients is unknown. However, in the patient with massive hemorrhage from the AVF (No. 4), vessel recanalization may possibly be attributable to rapid blood flow through the arteriovenous communication or to relative increase in the diameter of the embolized vessel lumen during recovery from hypovolemic shock.
In the past, a few reports have described the relationship between coagulopathy and outcome of transcatheter embolization (19, 20). While it has generally been accepted that coagulopathy is considered a negative factor in the control of hemorrhage, Yonemitsu et al. have shown in their study that transcatheter embolization with NBCA was effective in arresting acute arterial bleeding in a setting of coagulopathy (21). In our series, the outcome of NBCA embolization in three patients with INR prolongation was successful. One of these patients with a hemorrhagic transplant kidney had previously undergone transcatheter embolization using gelatin sponge particles just after recovering from sepsis, after which the embolized vessels had recanalized. Although we are not able to draw any conclusions on the matter due to the small sample size of our study, the outcome of these patients agree with that described by Yonemitsu et al. where they concluded that transcatheter embolization using NBCA (with or without microcoils) in coagulopathic patients was comparatively more effective than that using gelatin sponge particles with respect to hemostasis and prevention of recurrent hemorrhage.
There are some limitations to this study, such as its retrospective nature and the small number of subjects included in the series. In addition, six different radiologists performed the procedures in this case series and, therefore, we cannot exclude the possibility that there may have been minor differences in the technique of embolization.
In conclusion, transcatheter NBCA embolization of the renal artery is a safe and feasible procedure that offers effective occlusion of the pathologic vessel. Beyond being an alternative embolic material, NBCA can be used to complement other embolic materials, especially in patients with coagulopathies.