
Abstract
Background
There is an increasing frequency of requests for cochlear implantation (CI) in deaf children and more detailed image information is necessary for selecting appropriate candidates. Cochlear nerve deficiency (CND) is a contraindication to CI. Magnetic resonance imaging (MRI) has been used to evaluate the integrity of the cochlear nerve. The abnormalities of the cochlear nerve canal (CNC) and internal auditory canal (IAC) have been reported to be associated with CND.
Purpose
To correlate CNC manifestation, size, and IAC diameter on high-resolution CT (HRCT) with CND diagnosed by MRI in children.
Material and Methods
HRCT images from 35 sensorineurally deaf children who had normal cochlea but bilateral or unilateral CND diagnosed by MRI were studied retrospectively. The CNC and IAC manifestation and size were assessed and correlated with CND.
Results
CND was diagnosed by MRI in 54/70 ears (77.1%). Thirty-two ears had an absent cochlear nerve (59.3%), while 22 ears had a small cochlear nerve (40.7%). The CNC diameter was, 1.5 mm in 36 ears (66.7%). The CNC diameter ranged between 1.5 and 2.0 mm in seven ears (13.0%) and was .2.0 mm in 11 ears (20.4%). The IAC diameter was, 3.0 mm in 25 ears (46.3%) and .3.0 mm in 29 ears (53.7%).
Conclusion
The hypoplastic CNC might be more highly indicative of CND than that of a narrow IAC.
Keywords
A variety of cochlear or retrocochlear abnormalities can lead to sensorineural hearing loss (SNHL) in children. Cochlear nerve deficiency (CND) is believed to be one of the causes of SNHL. Tang et al. reported that up to 10% of SNHL children suffer from CND (1). CND is characterized by small or absent eighth cranial nerve seen on magnetic resonance imaging (MRI), including both congenital deficiency and acquired degeneration (2). The causes of CND are complex. Several studies have suggested that CND is always associated with inner ear and brain abnormalities (3–5). In a recent report by Pagarkar et al. (6), most subjects (84%) with absent or hypoplastic cochlear nerve showed cochlear or vestibular abnormality. The acquired CND may result from degeneration of the nerve fibers after cochlear injuries. However, in our daily experience, there are many sensorineural deaf children who were diagnosed as having CND only with diametrical changes of cochlear nerve canal (CNC) and/or internal auditory canal (IAC) but without any other abnormalities.
In 2000, hypoplastic bony canal of the cochlear nerve was reported in patients with congenital SNHL (7). Recently, Kono also reported a relationship between cochlear nerve canal stenosis and SNHL (8). However, there have been no MRI results indicating whether cochlear nerve is hypo-plastic or not in their studies. The correlation of CND and CNC remains unclear. To the best of our knowledge, there have been a very few studies describing the correlation of CNC and IAC with CND. Sachiko and Mikiko conducted CT and MRI examinations of ears with SNHL and reported the correlation between CND and CNC (9, 10), but the sample size was relatively small.
In view of this, we conducted a retrospective study on children with SNHL, whose cochlear nerve was diagnosed deficient by MRI but no other congenital abnormalities of cochlea or inner ear could be detected. The purpose of this study was to evaluate the diameters of the CND and IAC of children with CND retrospectively. We also aimed to correlate CNC manifestation, size, and IAC dimensions with CND.
Material and Methods
Ethics statement
The institutional review board for this study involving human subjects approved the procedures. Written informed consent, in line with the Declaration of Helsinki, was obtained prior to all studies. CT was done as part of routine clinical care, while MRI was performed in addition as part of the approved protocol.
Patients
Thirty-five children with bilateral or unilateral CND diagnosed by MRI who also underwent HRCT from August 2009 to August 2011 were studied retrospectively (Table 1). The median age of the children was 4.5 years (range, 1–16 years), including 22 boys and 13 girls. All of them were diagnosed as having bilateral or unilateral SNHL by audio logical evaluation. Children with CND who had underlying disease or cochlear malformation, vestibular and/or semicircular canal dysplasia, or any other abnormalities beyond CNC and IAC were excluded.
Detailed MRI and CT data of children with bilateral or unilateral CND
A, absent; B, bilateral; CN, cochlear nerve; CNC, cochlear nerve canal; CND, cochlear nerve deficiency; F, female; FN, facial nerve; IAC, internal auditory canal; IVN, inferior vestibular nerve; L, left; M, male; N, normal; R, right; S, small; SNHL, sensorineural hearing loss; SVN, superior vestibular nerve
Data acquisition and measurement protocol
All patients underwent both HRCT and MRI of the temporal bone. The HRCT scans were performed using a 64-slice spiral CT scanner (Philips Brilliance 64, Philips Medical Systems, Best, The Netherlands). Volumetric acquisitions were reconstructed with 1-mm slice thickness throughout the temporal bone contiguously. The transverse imaging plane was parallel to the supraorbital-meatal line. This allowed creating multiplanar reconstructions in any plane. The images were reconstructed using a high-spatial-resolution bone algorithm with 0.33-mm slice thickness and a 18-cm field of view. The matrix size was 512 × 512, which resulted in an in-plane pixel size of 0.35 × 0.35 mm with a voxel size of 0.35 × 0.35 × 0.33 mm. Bone window settings were designed as window level of +700 HU and window width of +4000 HU.
MR images were obtained on either a 1.5 Tesla Signa scanner (GE Healthcare, Milwaukee, WI, USA) or a 3.0 Tesla Signa scanner (GE Healthcare) with the matched eight-channel phased array coils. The protocol was designed to obtain routine axial and coronal unenhanced T2-weighted image and axial T1-weighted image, as well as axial three-dimensional fast-imaging employing steady-state acquisition (3D FIESTA) images of temporal bones. Parameters for the 3D FIESTA sequence varied by scanner (repetition time/echo time/number of excitations, 4.88-5.08 ms/1.4-2.0 ms/1-2; flip angle, 60°; field of view, 160-180 mm; matrix size, 256 × 224-288 × 384; slice thickness, 0.6 mm; spacing, -0.3-0.6 mm). The total scanning time was approximately 20 min for each patient. The temporal bone sequences were reconstructed in the axial plane as well as in an oblique sagittal plane, approximately perpendicular to the long axis of each IAC for viewing. MR images were reviewed in consensus on a clinical PACS workstation by two senior radiologists. The facial nerve, superior vestibular nerve, inferior vestibular nerve, and cochlear nerve were recognized on the oblique sagittal MR images obtained through the lateral aspect of the IAC.
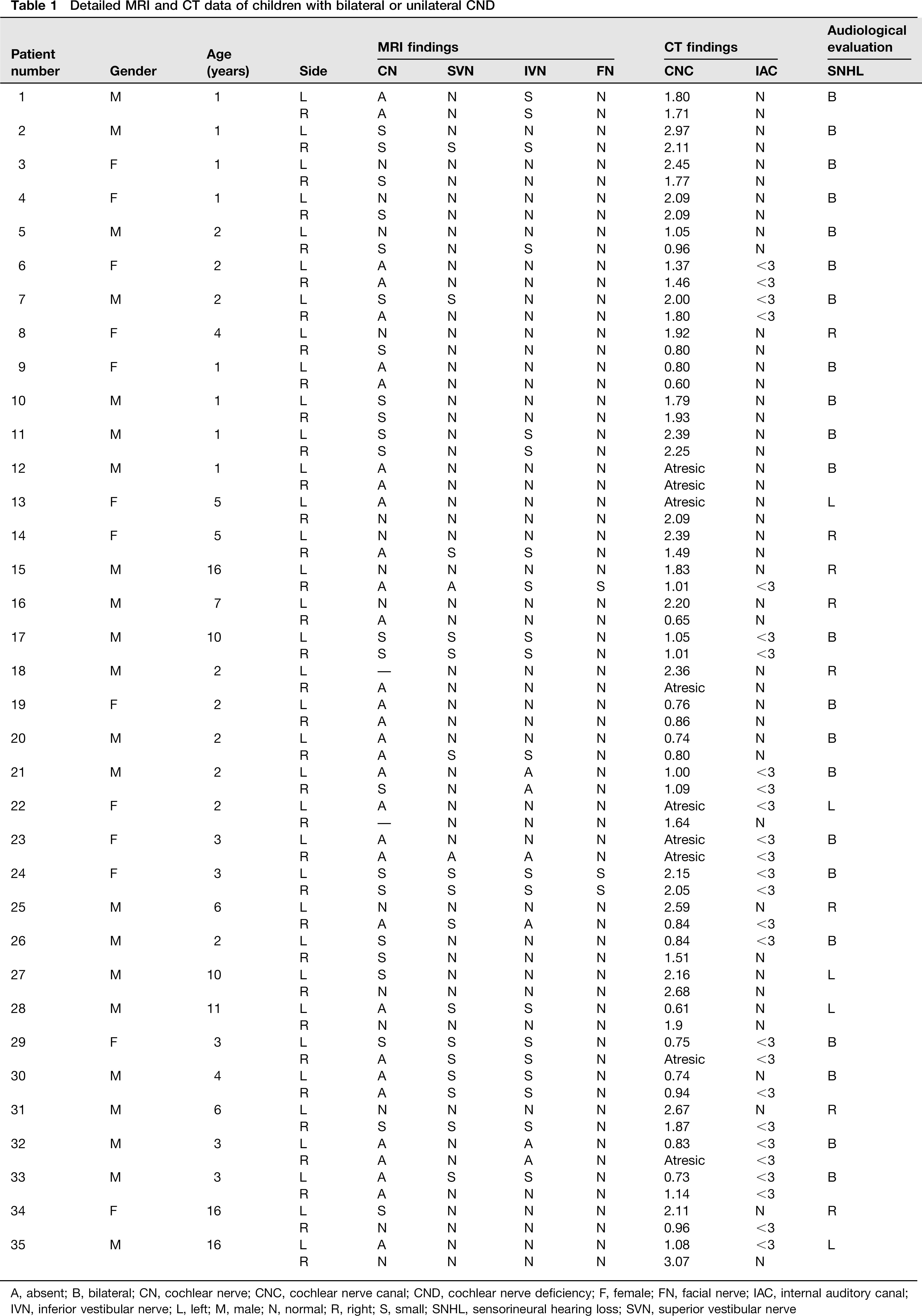
The normal cochlear nerve passes through the IAC along with the facial nerve and the vestibular nerve. The vestibular nerve deviates into the superior and inferior vestibular nerves distal to the IAC. Then the cochlear nerve goes alone from the fundus of the IAC to the base of the modiolus through CNC. In parasagittal images, four nerve routes were observed (Figs. 1a and 2a). According to a previous study, the cochlear nerve is larger than both the superior or inferior vestibular nerve in 90% of normal ears and is of similar size to or larger than the facial nerve in 64% of normal ears (11). In this study, CND was diagnosed when the cochlear nerve was absent or small. The cochlear nerve was considered absent when it could not be identified either on the axial or the oblique sagittal plane (Fig. 1b). The cochlear nerve was designated as small when it was clearly visible but appeared decreased in size than the ipsi-lateral superior never, inferior vestibular nerves, facial nerve, and contralateral cochlear nerve of the IAC (Fig. 2b). The cochlear nerve was designated as absent when it could not be identified on axial, coronal, or reconstructed coronal oblique IAC images (12).
Oblique sagittal MRI for a 10-year-old boy with the left sensorineural hearing loss. (a) The right internal auditory canal is normal. The distal slice shows the facial (F), superior vestibular (SV), inferior vestibular (IV) and cochlear (C) nerves. (b) The left cochlear nerve is absent Oblique sagittal MRI for a 2-year-old girl with the right sensorineural hearing loss. (a) The left cochlear nerve is normal, while (b) the right cochlear nerve is small (arrows)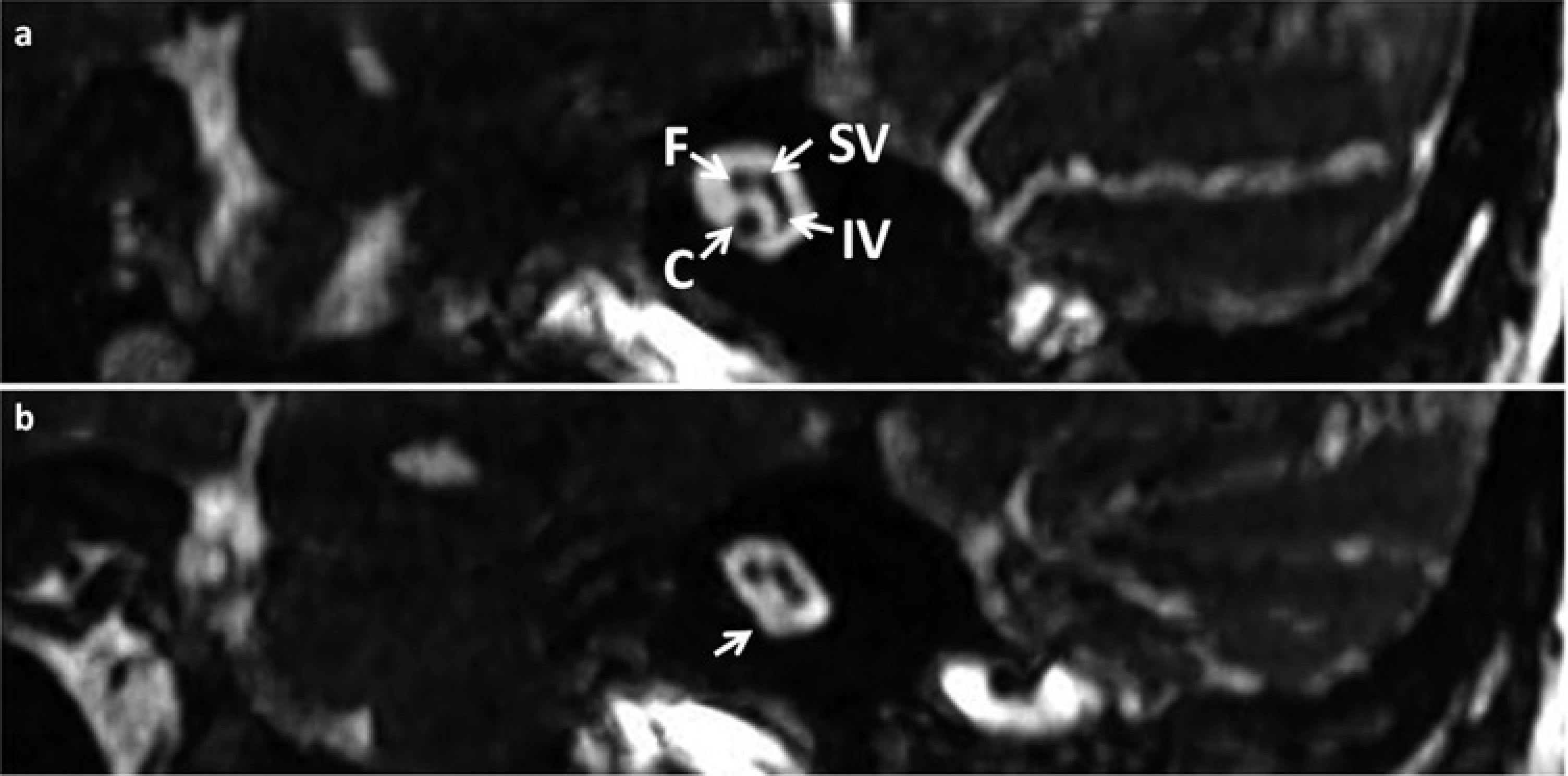
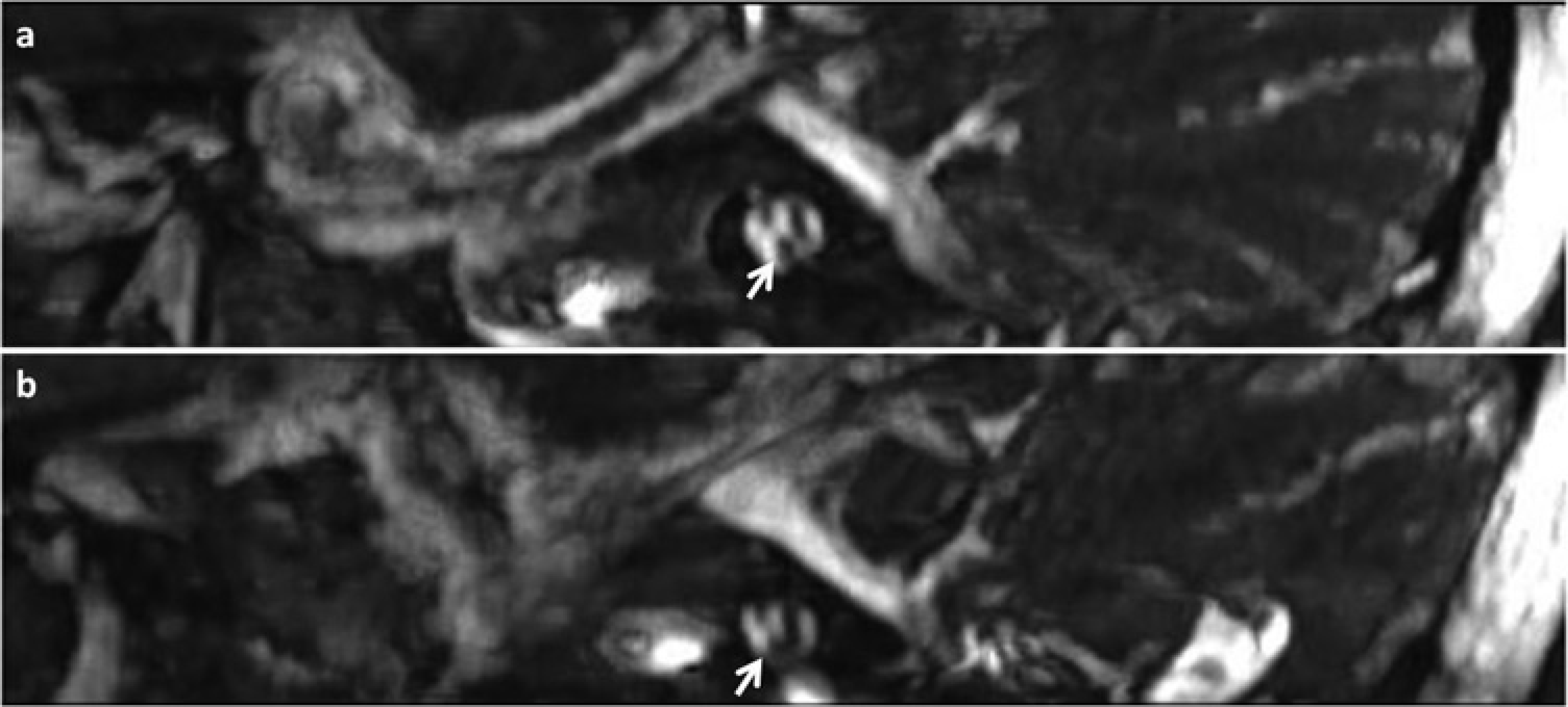
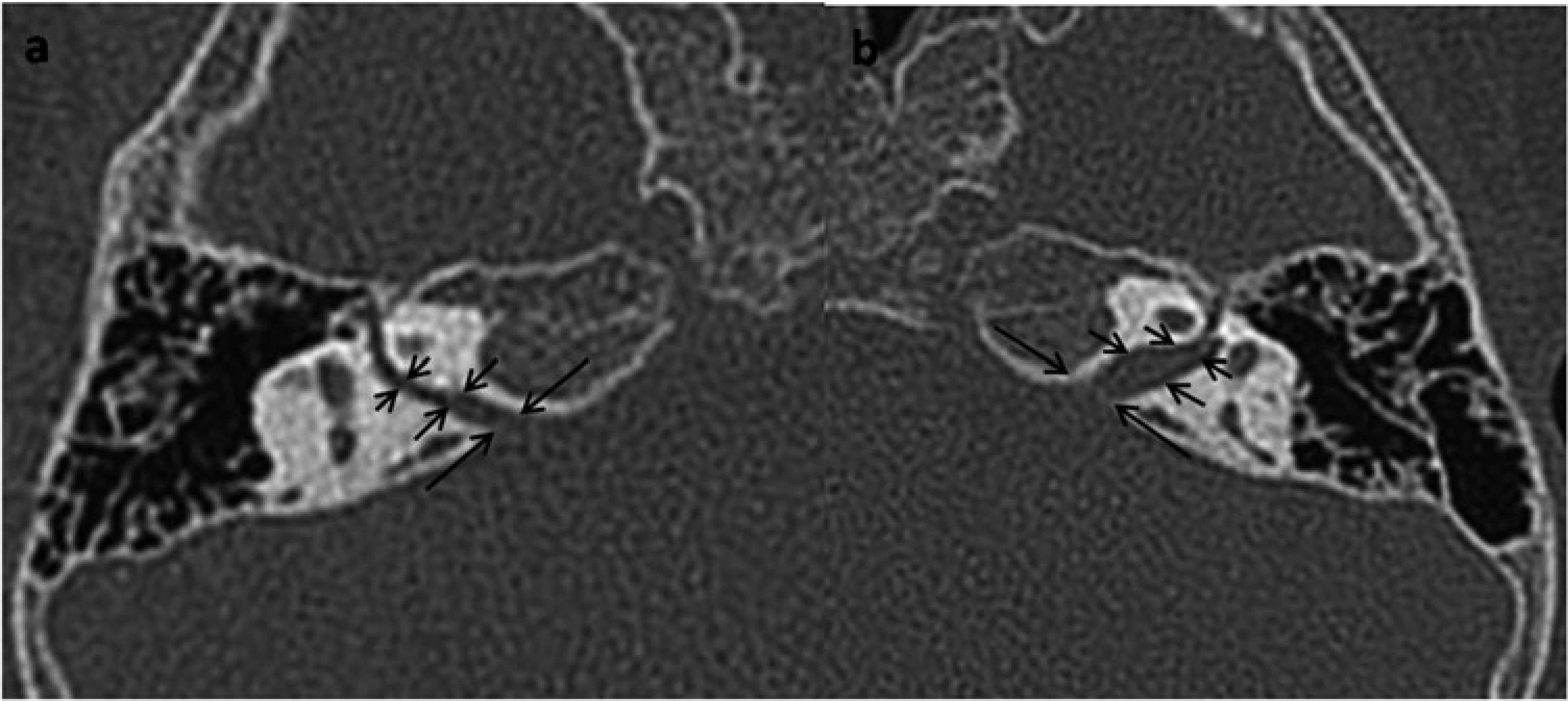
The HRCT images of children with CND were retrospectively reviewed and assessed, and the diameters of CNC and IAC were mainly measured. The CNC situating at the fundus of the internal acoustic meatus was measured in millimeters according to the method proposed by Stjernholm et al. in which the relatively exact data were measured using silicone rubber casts (13). In order to obtain the width of the CNC, two straight lines were drawn along the fundus of the IAC and the base of the modiolus, respectively. Then their midline was measured as the width of the CNC (Fig. 3a and b). CNC atresia was determined when the bone plate appeared at the corresponding location of the CNC (Fig. 3c). On the axial plane, the diameters of the midportion of the IAC were measured at the level of the porus acousticus from its posterior margin to the anterior wall of the IAC along a line orthogonal to the long axis of the IAC. A stenotic IAC was designated when the diameter of the midportion of the IAC was <3 mm (14) (Fig. 4).
Measurement of the diameter of the CNC. Axial thin-section CT scan of the temporal bone. (a) The width of the cochlear nerve canal (CNC) was measured along the inner margin of its bony walls at its mid-portion (arrows). In a 5-year-old girl with SNHL and the small cochlear nerve on the right, the width of the left CNC measured between the arrows is 2.39 mm. (b) The same case as in (a), the right CNC is hypoplastic with the width of 1.4 mm. (c) Another case, a 3-year-old girl with profound SNHL and bilateral cochlear nerve absence shows severe CNC atresia (the right CNC was also unopened, only the left was demonstrated here) High-resolution CT image for a 4-year-old boy with sensorineural hearing loss showing cochlear nerve absence and bilateral cochlear nerve canal atresia. Medial (long arrows), lateral (short arrows), and middle (medium arrows) portions of the internal auditory canal (IAC), as determined by drawing a perpendicular line orthogonal to the long axis of the IAC on a transverse image. (a) The diameter of the mid-portion of the right IAC is 1.3 mm. (b) The diameter of the mid-portion of the left IAC is 2.5 mm
Results
Manifestation of cochlear nerve absence on MRI
The cochlear nerve of all ears could be evaluated on MRI. Of the 35 subjects (70 ears) with unilateral or bilateral profound SNHL, unilateral CND were diagnosed in 16 subjects (45.7%) while bilateral CND were diagnosed in 19 subjects (54.3%) according to MRI. Thus 54 out of 70 ears (77.1%) were diagnosed as CND. Thirty-two of these ears had an absent cochlear nerve (59.3%), while 22 ears of these had a small cochlear nerve (40.7%). Twenty-seven ears with CND were associated with the superior or inferior vestibular nerve hypoplasia or aplasia (50%), and three ears were associated with facial nerve abnormality (5.6%) (1).
CND and CNC measurements on HRCT
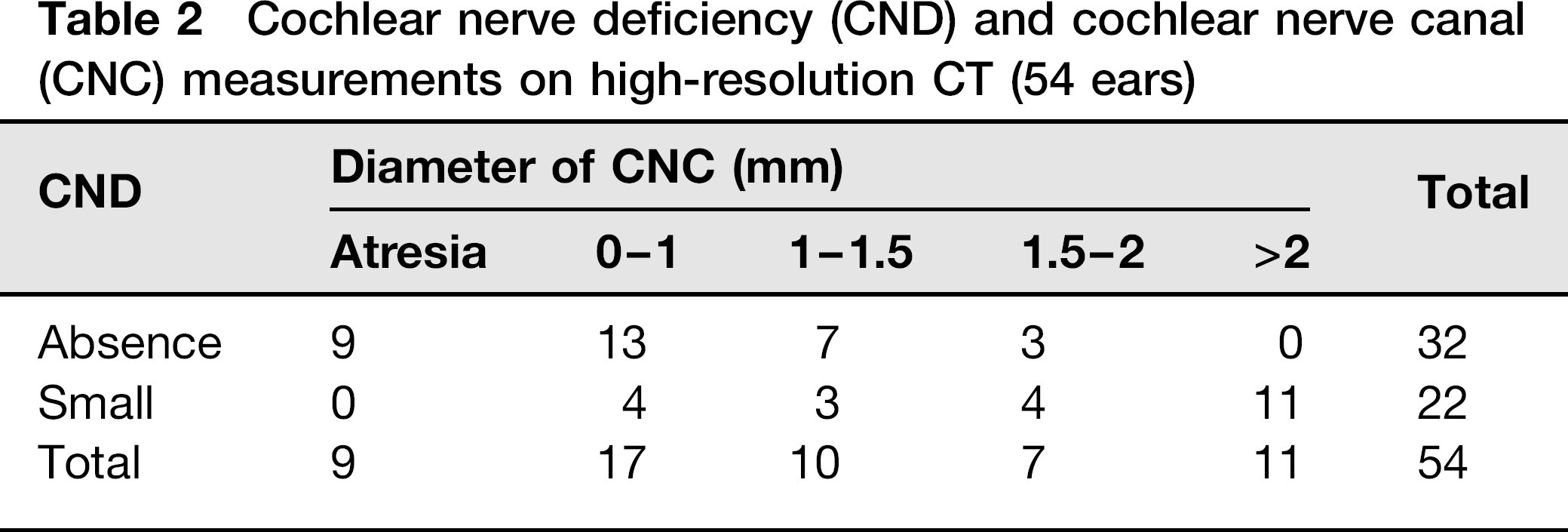
Of the 32 ears with cochlear nerve absence, nine ears (28.1%) had CNC atresia, CNCs of 13 ears were present but their diameters were <1.0 mm (40.6%). The diameter of CNCs ranged between 1 and 1.5 mm in seven ears (21.9%) and 1.5 and 2.0 mm in three ears (9.4%). None of the CNCs had a diameter >2.0 mm. Thus 90.6% of ears had cochlear nerve absence with a CNC diameter <1.5 mm.
Small cochlear nerve manifestations and CNC measurements on HRCT
There were 22 ears showing a small cochlear nerve. None of them had CNC atresia, but four ears exhibited a CNC diameter <1.0 mm (18.1%). The diameter of CNCs ranged between 1 and 1.5 mm in three ears (13.6%) and 1.5 and 2.0 mm in four ears (18.2%). The CNC diameter of 11 ears was >2.0 mm (50%).
Among the 54 ears with CND, 36 ears (66.7%) had a CNC diameter <1.5 mm, seven (13.0%) had a CNC diameter range of 1.5–2.0 mm, and 11 (20.4%) had a CNC diameter >2.0 mm (Tables 1 and 2).
Cochlear nerve deficiency (CND) and cochlear nerve canal (CNC) measurements on high-resolution CT (54 ears)
CND and IAC measurements on HRCT
Of the 32 ears with absent cochlear nerve, 16 ears had an IAC with a diameter of <3 mm (50%), while the IAC diameter of the remaining 16 ears was >3 mm. Of the 22 ears with small cochlear nerve, nine ears had an IAC with a diameter of <3 mm, while the IAC diameter of the remaining 13 ears was >3 mm. Altogether, of the 54 ears with CND, 25 ears (46.3%) had an IAC diameter of <3.0 mm and 29 ears (53.7%) had an IAC diameter of >3.0 mm (Tables 1 and 3).
Cochlear nerve deficiency (CND) and internal auditory canal (IAC) measurements on high-resolution CT (54 ears)

Discussion
Development of CNC and IAC
During embryonic development, the mesodermal layer surrounds the vestibulocochlear complex. The mesodermal layer becomes cartilaginous and ultimately transforms into bone as the IAC. Rothschild et al. reported that the IAC develops with a smaller caliber when there is a problem with embryogenesis of the vestibulocochlear complex and the small caliber IAC may consequently cause dysfunction of the auditory or vestibular nerves by compressive damage (15). Larson reported that the vestibulocochlear nerve starts to develop at approximately 3 weeks of gestational development (16). At 9 weeks of gestational development, the IAC is formed by the buildup of cartilage with normal development of the nerve (17). That is, the IAC cannot be formed in the absence of the nerve. The CNC is also thought to be formed at this time and requires stimulation by its contents for normal development. Accordingly, CNC stenosis might be secondary to cochlear nerve hypoplasia (8). If cochlear nerve hypoplasia results in a smaller caliber of the IAC during development, then certainly a narrowing of the endpoint of the IAC may also be associated with some auditory nerve anomalies. If a small IAC can cause damage or dysfunction to the vestibulocochlear complex, a narrow aperture where the cochlear nerve leaves the IAC and enters the cochlea could easily cause analogous or unique auditory problems.
Correlation of CND and CNC
The CNC is an important structure, which needs to be noticed in the assessment of a CT study of the temporal bone. The CNC is the short canal between the fundus of the IAC and the base of the modiolus, which carries the cochlear nerve fibres from the spiral ganglion to the cochlear nerve (18). Evidence suggested that when the CNC is stenotic, the cochlear nerve is often hypoplastic (9, 18). Authors reported that the CNC is smaller in deaf compared with normal hearing subjects. However, there is no consensus regarding the threshold which can be used to indicate CND. Stjernholm and Muren concluded that the possibility of a CND should be considered if the diameter of CNC was <1.4 mm (13). Bamiou and McClay suggested that when the CNC is <2 mm, the presence of a cochlear nerve should be determined by MRI, in particular in the case of pre-cochlear implant assessment (19–21). Komatsubara et al. reported that patients with a CNC <1.5 mm examined by CT would be diagnosed as having CND by MRI with 88.9% sensitivity and 88.9% specificity (9). In a report by Kono, a CNC diameter <1.7 mm suggested cochlear nerve hypoplasia, even if no cochlear abnormality could be seen on CT (8). Teissier et al. considered that 1.8 mm was a satisfactory threshold (22).
In this study, we examined HRCT scans of children with CND diagnosed by MRI and measured the diameter of CNCs to study the relationship between CND and CNC. Our results showed that more than half (66.7%) of ears with CND had a CNC diameter <1.5 mm on HRCT. This is in agreement with an earlier result reported by Komatsubara et al. (9). Our results also showed that not all the CND had a CNC <1.5 mm, and 20.4% CND had a CNC diameter >2.0 mm. According to our results, the possibility of a CND should be considered when the diameter of the CNC is <1.5 mm. Then, a further evaluation with MRI should be performed to confirm. The diameter of the CNC can be used as a supportive indicator of the CND but it does not always indicate the presence of CND.
The cochleas of the patients with CND enrolled in this study were normal on either MRI or CT. This suggests that the cochlear structure may develop irrespective of afferent and efferent innervations (23).
The cause of a small and atresic CNC in patients with SNHL is not clear. As is the case for development of the IAC, the normal development of CNC may also require stimulation by the cochlear nerve. Accordingly, hypoplasia of the CNC may be secondary to a hypoplastic cochlear nerve (8). In this study, all of the nine ears with an atresic CNC accompany with an absence of the cochlear nerve. The data of the present study allow us to propose that the presence of the cochlear nerve is essential for CNC to develop normally.
Correlation of CND and narrow IAC
Previous studies have suggested that a narrow IAC on HRCT is often an indication of CND (2, 13). However, it has been shown that the cochlear nerve branch may be absent on MRI despite a normal IAC (24, 25) and the intact cochlear nerve has been reported in the narrow IAC (26–28). In the present study, the diameter of the IAC was >3 mm in 29 ears of 54 ears with CND (53.7%), while 25 ears of 54 ears with CND had a narrow IAC (46.3%). Results from this study have suggested that more than half of the CND had a normal IAC. From a developmental perspective, the findings of a normal-size IAC with CND may suggest an acquired cause, while a narrow IAC with CND may be due to nutritional deficiencies before the 24th week of pregnancy. Therefore, children with a narrow IAC seen on HRCT were diagnosed as having CND with only 46.3% (25/54) sensitivity. This study highlights that the narrow IAC does not necessarily indicate the presence of CND.
CND and the cochlear implantation
Identification of an intact cochlear nerve is crucial for cochlear implant candidates because it may affect the improvement in hearing performance. Papsin found that children with narrow IAC and/or cochlear canal performed more poorly than all other groups of children with anomalous cochlea in speech perception scores after cochlear implantation (29). There is recent evidence that patients with hypoplasia of the CNC may not benefit from cochlear implantation to the same extent as those with a normal CNC. A narrow CNC may lead to diminished ability to use auditory information delivered through a cochlear implant (6).
Diagnostic imaging of the CND
The optimal imaging method for children with SNHL has been debated for many years. Bettman et al. recommended that CT alone was sufficient, because CT can be used to measure the width of the CNC and then predict the possibility of CND easily and quickly in almost all situations (30). Additionally, CT allows a precise identification of congenital malformations, temporal bone fractures, cochlear ossification, and the position of the facial nerve. It can also be used to analyze the CNC, although only MRI adequately visualizes the cochlear nerve itself. Third, it is difficult to perform a MRI examination in every hospital. It is still difficult to examine younger patients using MRI, but it is very useful and important to assume CND on CT (31).
Bamiou et al. suggested that the cochlear nerve itself should be evaluated using MR in patients with suspected hypoplasia of the bony canal of the cochlear nerve on CT scans (26). MRI can visualize the scala vestibuli media, the scala tympani, and the vestibulocochlear bundle as well as its branches in the IAC and intracranial structure directly. In the assessment of the cochlear implant candidates, MRI is necessary whatever the size of the canal on CT to determine the integrity of the nerve because successful implantation depends on the intact cochlear nerve fibers. Both CT and MRI images of ears with congenital SNHL were examined in this study. We recommend that MRI should be performed in addition to CT scans for all cases of pre-cochlear implant assessment. A combined application of CT and MRI can provide useful complementary information.
In conclusion, this study highlights that the CND can occur in children with SNHL despite the demonstration of a normal cochlea. A narrow IAC may not always indicate CND. The diameter of the CNC which is <1.5 mm can be used as an indicator of CND.
Footnotes
Acknowledgements
This study was supported by Jieping Wu Medical Foundation. We would like to thank all the volunteers participated in this study and to gratefully acknowledge Helen Zhang and Xiaomei Lu for paper writing and constructive suggestions. Jianhong Li and Fei Yan contributed equally to this paper.