
Abstract
Background
The intimal flap of aortic dissection may extend to the abdominal branches and probably lead to malperfusion syndrome. Renal malperfusion and renal atrophy are significantly related to patient outcomes.
Purpose
To study the extent of the intimal flap and predisposing factors for renal atrophy in patients with aortic dissection.
Material and Methods
From January 2001 to June 2008, 176 (137 men, aged 21–86 years, mean 51.9 years) of 225 subjects with aortic dissection and computed tomography (CT) met the inclusion criteria for this study. Of these 176 patients, 35 (19.9%) developed unilateral renal atrophy. A review of the CT was conducted to classify aortic branch vessel perfusion into three types: type 1, in which the branch vessels are perfused exclusively from the true lumen; type 2, in which the branches are perfused from both the true and false lumens; and type 3, in which the branches are perfused exclusively from the false lumen. Variables including age, gender, type of aortic dissection, type of perfusion of the abdominal branches, and the presence of thrombi in the false lumen were analyzed to determine whether these factors were related to the left or right side and global or focal renal atrophy.
Results
Of 880 abdominal branches in 176 patients, 622 (70.7%) were classed as perfusion type 1, 50 (5.7%) as type 2, and 208 (23.6%) as type 3. Type 3 perfusion was most commonly observed in the left renal artery, at a frequency of 31.7% (66/208). Partial thrombosis in the false lumen above the level of the renal arteries was seen in 68.8% of patients; such thrombi and type 3 perfusion of the renal artery were significantly related to renal atrophy. The laterality (left or right) and extent (global or focal) of renal atrophy were not related to age, gender, type of aortic dissection, or perfusion type.
Conclusion
Type 3 perfusion is most frequent in the left renal artery, and such perfusion and partial thrombi in the false lumen above the renal arteries are significantly related to the development of renal atrophy.
Aortic dissection is a cardiovascular emergency that often results in a fatal outcome. Its incidence has been reported to range from 2.9 to 3.5 per 100,000 persons (1, 2). Based on the Stanford classification, acute type A aortic dissection requires surgical management, while medical treatment remains the first-line therapeutic approach for uncomplicated acute type B aortic dissection (3, 4). Nevertheless, high 1-month mortality rates are observed for both type A and B aortic dissections (5–7). Thus, treatment of aortic dissection is aimed at preventing lethal complications such as aortic aneurysm and rupture, compromised coronary arteries, cardiac tamponade, stroke, visceral malperfusion, and circulatory failure.
Visceral malperfusion syndrome results from obstruction of the aortic branches secondary to dissection. Variability in dissection flap propagation can produce multiple configurations of true and false lumens and many combinations of branch vessel involvement (8). This anatomic and hemodynamic compromise of the branch vessels was classified by Williams et al. as either static or dynamic obstruction (9). Static obstruction results from static extension of the dissection flap directly into a visceral branch, whereas dynamic obstruction results from prolapse of the dissection flap into the origin of vessel (9). Gaxotte et al. proposed an alternative image-based classification system of the position and extent of intimal flaps complicated by malperfusion syndrome involving reference to the axis of the collateral branches (10).
Renal malperfusion is one of the clinical features seen in visceral malperfusion syndrome caused by aortic dissection. Studies have established that impaired renal perfusion is associated with high surgical mortality and is a significant independent predictor of the operative mortality rate (11–13). Long-term renal malperfusion can lead to focal or global renal atrophy and renal insufficiency. Therefore, the risk of renal atrophy in patients with aortic dissection can be correlated with patient outcomes.
The aims of this study were, first, to assess the extent of the intimal flap of aortic dissection and type of perfusion in abdominal branches, especially the renal arteries, according to computed tomography angiography (CTA), and second, in the context of evidence-based medicine, to investigate the predictors of renal atrophy based on patient data and computed tomography (CT) findings, including the type of aortic dissection, perfusion type in the renal arteries, and status of the false lumen. To our knowledge, this is the largest series describing the correlation of aortic dissection with late renal atrophy to date.
Material and Methods
Patient selection
Between January 2001 and June 2008, 225 patients (171 men and 54 women) aged 21–88 years (mean 52.9 years) with aortic dissection underwent CT in our medical center. The clinical data and imaging studies were retrospectively studied and analyzed. The retrospective study was approved by the institutional review board and informed consent was obtained from all subjects who underwent CT. All cases featured intimal flaps and the presence of true and false lumens. All patients were followed up annually with CT angiography, with a follow-up period of 1–9 years (mean 3.28 years).
Inclusion and exclusion criteria
Of the 225 patients, 49 patients (21.8%) were excluded for the following reasons: (a) the intimal flap did not extend to the abdominal aorta; (b) the patient had renal atrophy because of end-stage renal disease (ESRD) or an enlarged kidney due to polycystic kidney disease; or (c) there was a history of unilateral nephrectomy. The remaining 176 patients had aortic dissection that involved the abdominal branches including the celiac trunk, superior mesenteric artery (SMA), right renal artery (RRA), left renal artery (LRA), or inferior mesenteric artery (IMA) (Fig. 1). Of the 176 patients enrolled in this study, 137 were men. Their ages ranged from 21 to 86 years (mean 51.9 years). One hundred and four patients (59.1%) had type A aortic dissection and 72 patients (40.9%) had type B aortic dissection.
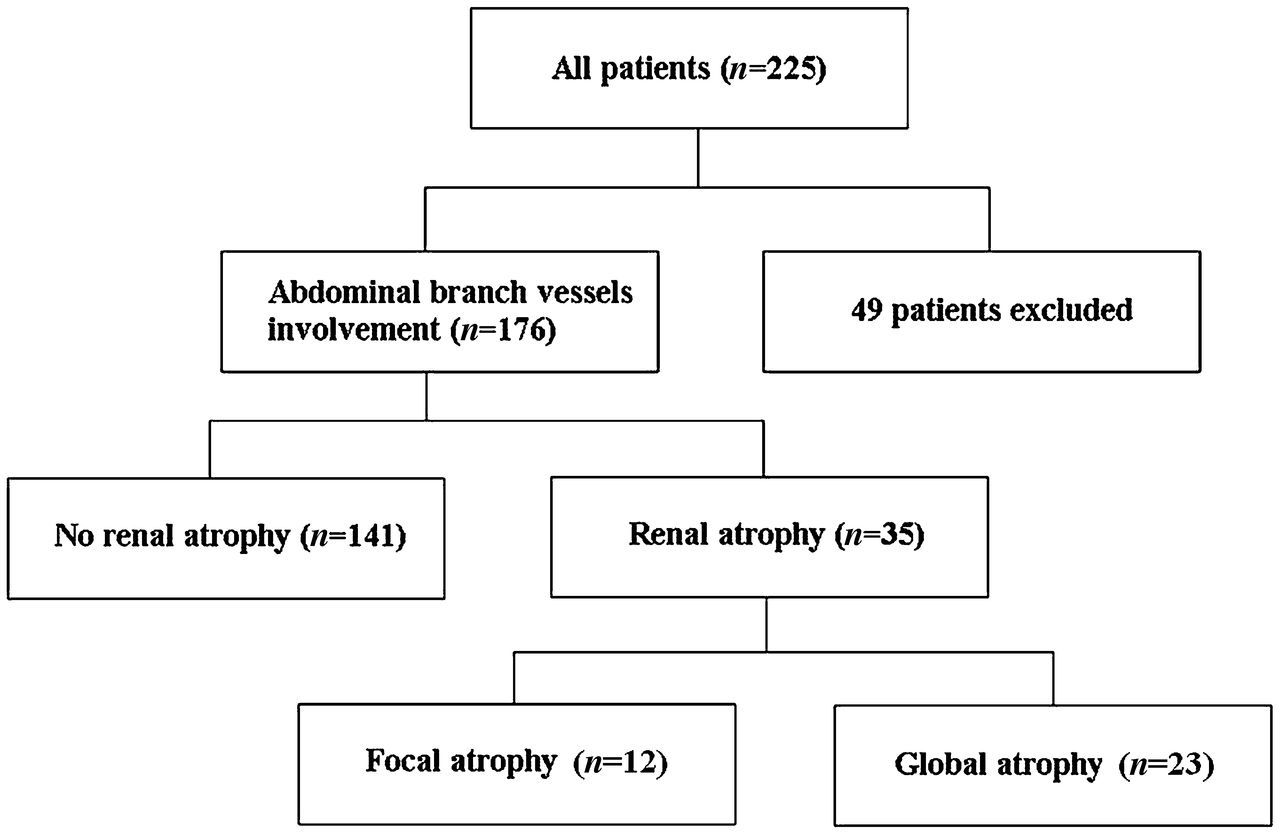
A branch diagram…summarizing the conditions and number of 225 patients with aortic dissection in this study
CT angiography
All examinations were performed using a 64-slice multidetector CT (MDCT) scanner (Aquilion 64, Toshiba Medical System, Tochigi, Japan), a 16-slice Siemens MDCT scanner (Somatom Sensation 16, Siemens Medical Solutions, Erlangen, Germany), or a 16-slice GE LightSpeed MDCT machine (GE Healthcare, Milwaukee, WI, USA) in the craniocaudal direction from the apical lung to the inferior aspect of the pubis. The scanning parameters were as follows: gantry rotations of 0.5 s, 120-kV tube voltage, 150 mAs, pitch 0.641 mm, collimation 64 × 0.5 mm for the Toshiba Aquilion scanner; gantry rotations of 0.5 s, 120-kV tube voltage, 120 mAs, pitch 1.25 mm, collimation 16 × 1.5 mm for the Siemens Somatom Sensation scanner; and gantry rotations of 0.5 s, 120-kV tube voltage, 50 to 160 mAs, pitch 1.375 mm, collimation 16 × 1.25 mm for the GE LightSpeed scanner.
The examination included both non-enhanced and contrast medium-enhanced CT. For enhanced CT images, 100 mL of non-ionic contrast medium, iohexol (Omnipaque, 350 mgI/mL; GE Healthcare, Cork, Ireland) or iodixanol (Visipaque, 320 mgI/mL; GE Healthcare, Cork, Ireland) or ionic contrast medium, iothalamate meglumine (Conray, 282 mgI/mL; Tyco Healthcare, Saint Louis, MO, USA) was administered intravenously at a rate of 3–4 mL/s through an 18- or 20-gauge catheter placed in the upper extremity. The enhanced transverse scan was performed 25–30 s after initiation of intravenous administration of contrast medium. The corticomedullary phase of renal enhancement was evaluated. We did not routinely perform delayed images for evaluation of excretory urogram.
All coronal and sagittal reformations were generated using a 3–5 mm slice thickness and 3–5 mm spacing. Multiplanar reconstructed images provided an overall view of the aortic dissection and demonstrated the anatomic relationship between the flap and the adjacent branch vessels.
Perfusion classification of abdominal branch vessels
For simplicity, we used a classification that divides aortic branch vessel perfusion based on CTA findings into three types: type 1, in which the branch vessels are perfused exclusively from the true lumen (left renal artery from true lumen in Fig. 2a); type 2, in which the branches are perfused from both true and false lumens (left renal artery in Fig. 2b); and type 3, in which the branches are perfused exclusively from the false lumen (left renal artery in Fig. 2c).

Perfusion types of left renal artery in different patients: (a) type 1, (b) type 2, and (c) type 3. T, true lumen; F, false lumen
Treatment
Depending on the type of aortic dissection, complications from malperfusion syndrome, and the patient's overall clinical condition, treatment options involved either an endovascular stent-graft placement or open surgical repair. Of the 176 patients, 134 patients underwent open graft repair surgery, seven received an endovascular stent graft, and 35 patients were medically treated.
Ninety-one of 104 patients with type A aortic dissection underwent surgical graft repair. Three patients received endovascular stent-grafting. Ten patients were medically treated due to co-morbid conditions, advanced age over 80 years old, or patient refusal. Of the 72 patients with type B aortic dissection, 43 patients underwent open graft repair (due to dissecting aneurysm in 41 and suspected aortic rupture in two), four patients underwent endovascular stent-grafting, and 25 patients were treated medically. Marfan syndrome was found in seven out of 176 patients, five with type A dissection and two with concomitant type B aortic dissection and annuloaortic ectasia. All seven patients underwent surgical graft repair. Using the interposition aortic grafting technique, felt strips were used to buttress the distal anastomosis via the “sandwich” technique. In patients with dissection involving the aortic valve, resuspension, or valve replacement was performed to treat aortic regurgitation. Felt pledgets were used to repair the bypass cannulation site in the native aorta. Surgical fenestration at the distal graft anastomosis was not routinely performed in our institute.
Retrospective image review
The CT angiograms were analyzed retrospectively by two experienced radiologists in consensus. By reviewing the different portions of the abdominal aorta and its branches, the observers assessed whether the renal arteries or accessory renal arteries were supplied by a true lumen, false lumen, or both. The contrast-enhanced images of initial CT at the time of dissection were reviewed to evaluate absent or delayed cortical nephrogram as a clue of suspected renal ischemia in the setting of acute aortic dissection.
Definition
Renal atrophy was classified as either focal or global (Fig. 3). Focal renal atrophy was defined as loss of renal parenchyma with no reduction in renal length (Figs. 3a and 4e). Global renal atrophy was defined as a reduction in renal length of more than 20% despite thinning of the renal parenchyma (Figs. 3b and 5e). All cases were measured during follow-up examination and were compared with initial CT images taken at the time the aortic dissection occurred. The renal length was measured on the long axis of the kidney on a CT workstation.
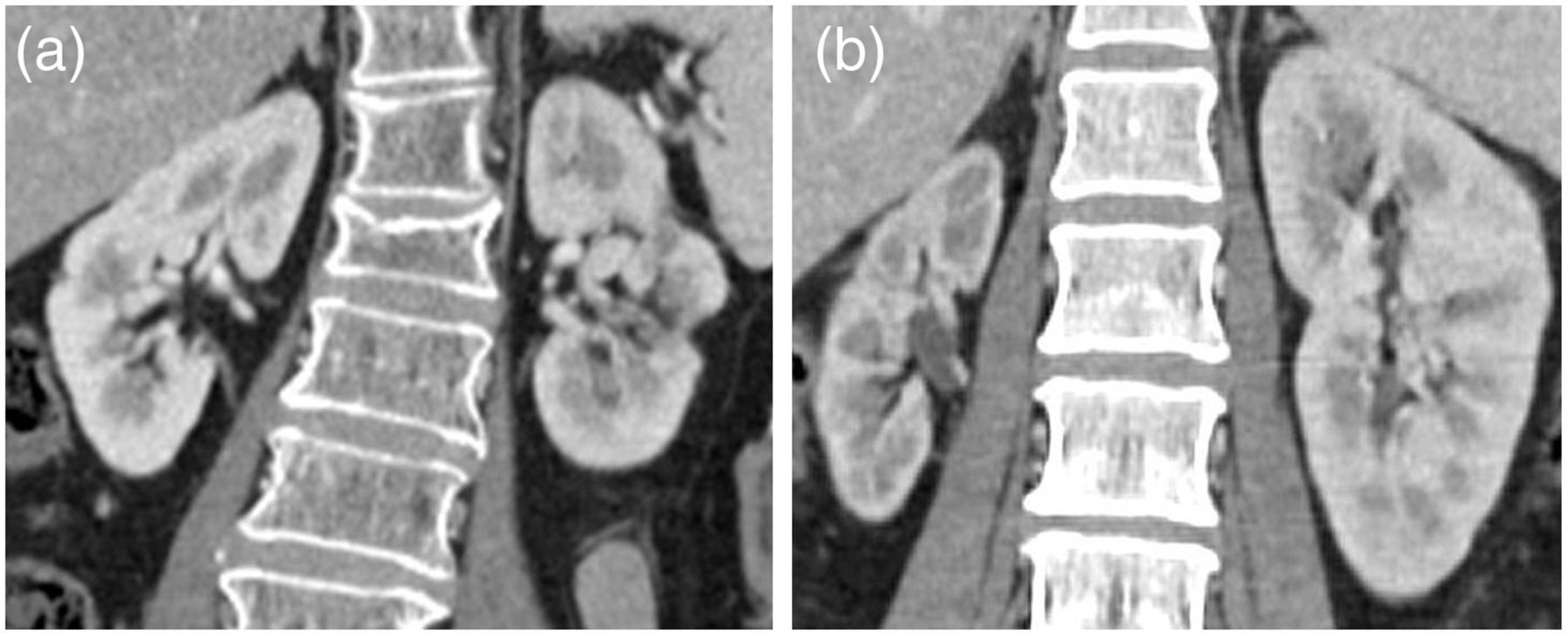
Enhanced CT of kidneys in coronal reconstructed images shows (a) focal atrophy of the left kidney and (b) global atrophy of the right kidney
The false lumen proximal to the renal arteries on postoperative CT was classified as patent if flow was present without thrombus, as partial thrombosis if both flow and thrombus were present, or as complete thrombosis if no flow was present (6).
Statistical analysis
Values are presented as the mean ± standard deviation, and statistical significance was set at P < 0.05. Simple and multiple logistic regression analyses were used to examine the relationships between age, gender, aortic dissection type, type of perfusion of branch vessels, false-lumen status and presence of renal atrophy, laterality (right or left), and extent (focal or global) of renal atrophy. Multiple logistic regression analyses were performed using a forward stepwise selection process to study the independent influence of the above variables. The variables were analyzed and the strongest association with the presence of renal atrophy, laterality (right or left), and extent (focal or global) of renal atrophy was determined. All statistical analyses were conducted using the SPSS v. 14 statistical package (SPSS Inc., Chicago, IL, USA).
Results
Perfusion classification in abdominal aortic branches
The perfusion condition of the abdominal aortic branches is shown in Fig. 2. Of the three types, type 1 was the most common (LRA in Figs. 2a, 4a and c, 5b and c). Type 3 was observed most frequently in the left renal artery (Figs. 4d and 5d). Only one patient had concomitant type 3 perfusion in the celiac trunk, SMA, and IMA.

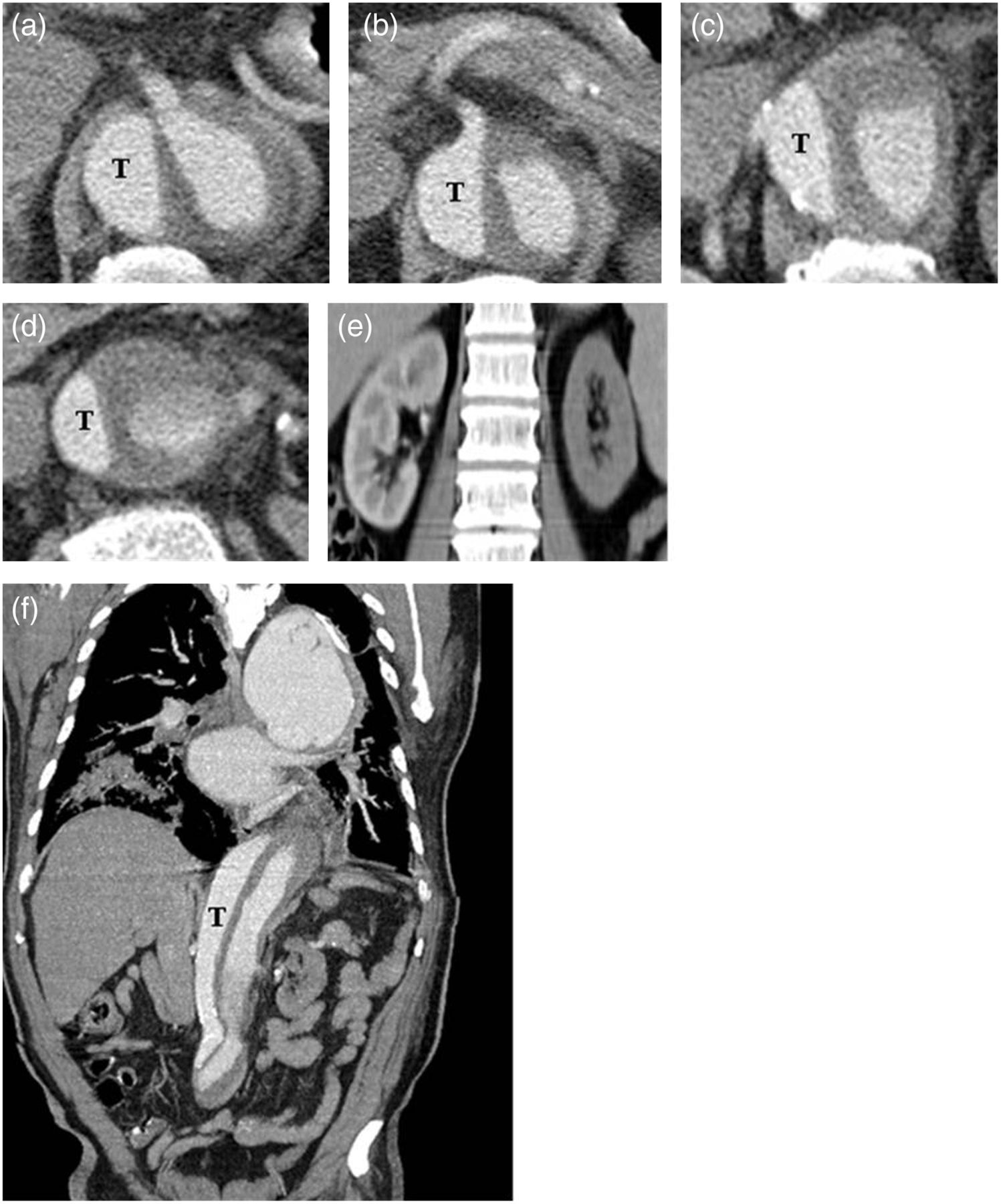
A 53-year-old man had aortic dissection and received open surgery with graft replacement. There was false lumen with partial thrombi proximal to the level of renal arteries. CT images show type 1 perfusion in (a) celiac trunk, (b) superior mesenteric artery, (c) right renal artery and type 3 perfusion in (d) left renal artery. (e) An axial CT image reveals focal atrophy of the left kidney. (f) Coronal CT shows partial thrombi in the false lumen above renal arteries. T, true lumen
A 56-year-old man had type B aortic dissection in 2001 and received intra-aortic graft. Enhanced CT images show different types of perfusion in abdominal branch vessels, including type 3 for celiac trunk (a), type 1 in superior mesenteric artery (b) and right renal artery (c), and type 3 in left renal artery (d). Reconstructed coronal-enhanced CT image shows global atrophy of left kidney (e) and thrombi in false lumen above renal arteries (f). T, true lumen
Of 176 patients with aortic dissection involving the celiac trunk, SMA, renal arteries, and IMA, 35 (19.9%) patients (25 men) had global or focal unilateral renal atrophy (Table 1). Twelve patients (34.3%) had focal renal atrophy (Figs. 3a and 4e) and 23 patients (65.7%) had global renal atrophy (Figs. 3b and 5e) (Table 2). Of the 35 patients with unilateral renal atrophy, 80% of the RRA arose from the true lumen (type 1) and 57.1% of the LRA arose from the false lumen (type 3).
Correlation among the renal atrophy, perfusion type of renal arteries and other variables (n = 176)
95% CI, 95% confidence intervals; LRA, left renal artery; OR, odds ratio; RRA, right renal artery
Correlation among the extent (focal or global) of renal atrophy, perfusion type of renal arteries, and other variables (n = 35)
95% CI, 95% confidence intervals; LRA = left renal artery; OR, odds ratio; RRA, right renal artery
One hundred and twenty-one patients (68.8%) had partial thrombi in the false lumen proximal to the level of the renal arteries (Table 1). Among patients without renal atrophy, 92 patients (65%) had partial thrombi in the false lumen above the renal arteries and 49 patients (35%) had patent false lumen. On the other hand, among 35 patients with renal atrophy, 29 patients (82%) had partial thrombosis in the false lumen and six patients (18%) had patent false lumen. None had complete thrombosis of the false lumen. There was a significant correlation between renal atrophy and partial thrombi in the false lumen proximal to the renal arteries (Table 1). There was also a significant correlation between renal atrophy and type 3 perfusion of the LRA (Table 1). Both simple and multiple logistic regression analysis revealed no significant correlation between the variables and extent (focal or global) of renal atrophy (Table 2).
The laterality of renal atrophy was analyzed to determine its relation (if any) with age, gender, type of aortic dissection, type of renal artery perfusion, or partial thrombi in the false lumen proximal to the renal arteries (Table 3). In univariate analysis, there was a significant correlation between the laterality of renal atrophy and type 3 perfusion of the renal arteries and partial thrombi in the false lumen. However, multiple logistic regression analysis failed to reveal any significant variables.
Correlation among the laterality (right or left) of renal atrophy, perfusion type of renal arteries, and other variables (n = 35)
95% CI, 95% confidence intervals; LRA, left renal artery; OR, odds ratio; RRA, right renal artery
Among the 35 patients who later developed renal atrophy, a unilateral delayed or absent cortical nephrogram was identified on initial CT images in 13 (37%) at the time of dissection (Fig. 6). On the other hand, 21 (60%) patients had normal renal perfusion on the initial CT scan (Fig. 7). One patient had bilateral diminished renal parenchymal enhancement, as well as global decreased enhancement of liver and spleen, presumably due to circulatory failure. This patient had a type 3 perfusion in left renal artery, type 1 perfusion in right renal artery and partial thrombi in false lumen. She developed left renal atrophy in follow-up CT scan.
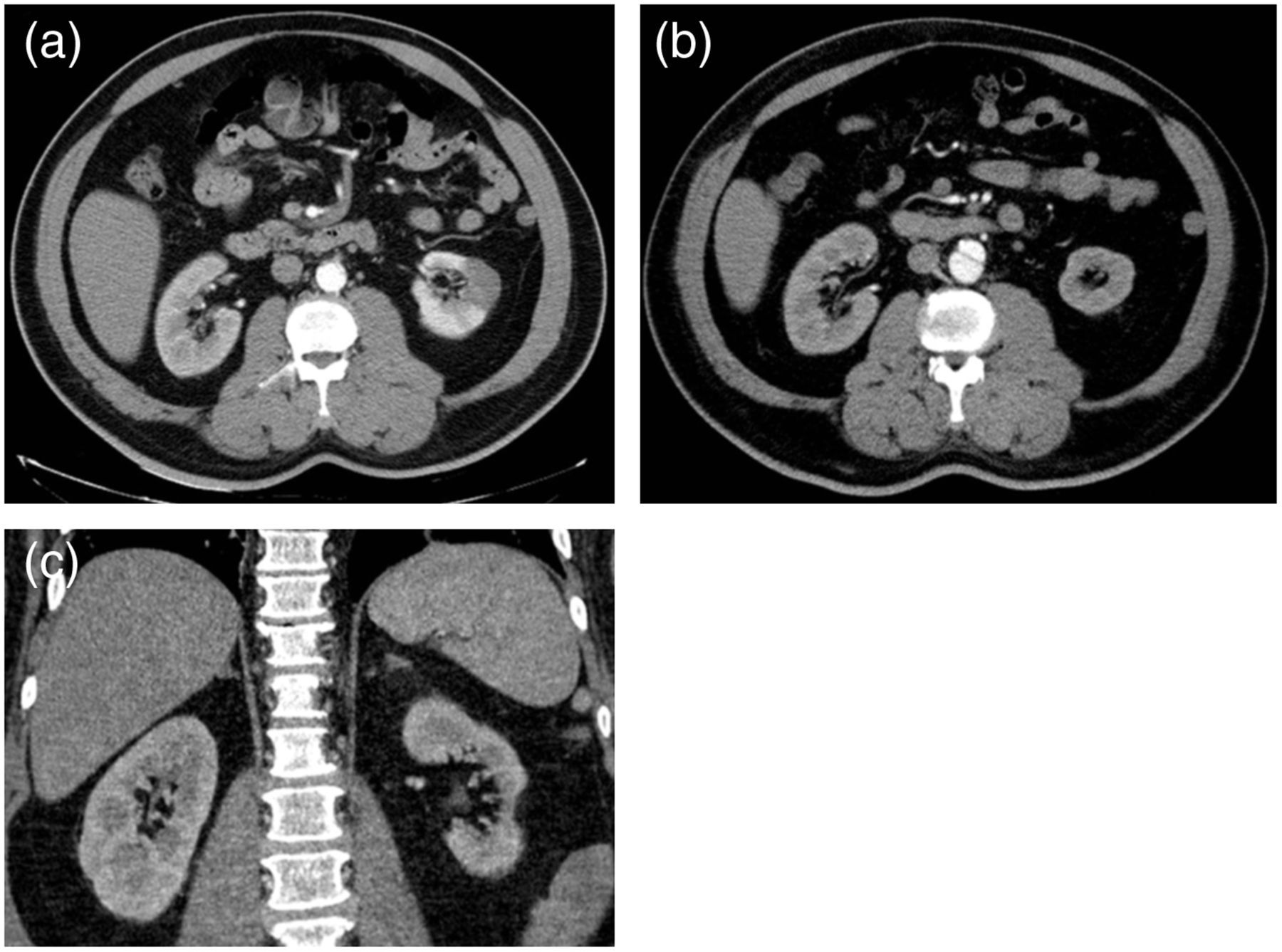
A 54-year-old man had type B aortic dissection. (a) Initial CT image in 2005 shows wedge-shaped left renal infarct. There is type 3 perfusion for left renal artery and type 1 perfusion for right renal artery (not shown). (b) Follow-up CT image and (C) reconstructed coronal CT image in 2008 reveals focal left renal atrophy

A 52-year-old woman with type A aortic dissection. (a) The initial CT shows normal left renal enhancement. The patient had a type 3 perfusion in left renal artery. (b) CT 1 year later shows partial thrombosis of the false lumen. The patient developed global left renal atrophy. (c) Reconstructed coronal image shows decreased left renal length and cortical atrophy. T, true lumen
CT angiography depicted 352 main renal arteries and 13 accessory renal arteries in 176 patients. All accessory renal arteries arose from the abdominal aorta. Eight accessory arteries were found on the left side and five on the right side. Eight accessory renal arteries arose from the true lumen and five arose from the false lumen. Among the patients without renal atrophy, eight patients (5%) had accessory renal arteries. In 35 patients with renal atrophy, five (14%) accessory renal arteries were recognized on CT. In 12 patients with focal renal atrophy, only one patient had an accessory renal artery, which arose from the partially thrombosed false lumen.
Discussion
Aortic dissection is one of the most catastrophic acute aortic events and results in high levels of mortality. Prompt diagnosis and treatment are essential to improve the prognosis. The outcome depends on the type and involvement of dissection, and other vascular complications such as stroke, visceral malperfusion, coronary branch involvement, and cardiac tamponade.
As illustrated in our study, multidetector CTA with enhanced CT axial images and three-dimensional reformatted images is the optimal imaging modality for comprehensive evaluation of aortic dissections. The benefits include a shorter scanning time, better spatial and contrast resolution, minimal invasiveness, fewer complications, and lower costs (14–16). Although non-invasive magnetic resonance angiography (MRA) is comparable to CTA in sensitivity and specificity, it is time-consuming and more susceptible to motion artifacts. Thus, it is more suitable in medically stable patients or patients with chronic dissections (17–19).
Branch vessel malperfusion may be the result of static extension of the dissection flap into a visceral branch, or prolapse of the intimal flap across the branch with dissection sparing the vessel origin, which is termed static and dynamic obstruction respectively (9). Williams et al. reported that intravascular ultrasonography and manometric findings clarify the mechanisms of branch-vessel compromise after aortic dissection and provide a rational guide for percutaneous treatment (9). Gaxotte et al. proposed a classification system based on the position and extent of the intimal flap with reference to the axis of the collateral branches; type 1 means the flap is parallel or perpendicular to the major aortic branch, type 2 means that the dissection extends into the major branch, and type 3 means the presence of ostial avulsion of the visceral artery (10). On reviewing the CT images, however, some ambiguity was encountered. Intimal flaps may be oblique to the branch vessels in type 1, and the intimal flaps that extend to the branch vessels may be parallel to their long axis in type 2. In addition, the Gaxotte classification was less frequently used as a guide in endovascular treatment. We used a classification that focuses on the perfusion of branch vessels based on CTA findings. In our classification, type 1 is equivalent to dynamic obstruction based on Williams' classification, type 2 refers to static obstruction, and type 3 is actually a subset of static obstruction with a circumferential re-entry tear in the dissected vessel, in which the vessel originates from the false lumen (9).
About 30% of patients with aortic dissection develop peripheral vascular ischemia and visceral malperfusion, which may increase the risk of morbidity and mortality (8, 12, 13, 20–23). Among the common features of visceral malperfusion syndromes, renal malperfusion has been recognized as the most important risk factor for increased mortality (11–13). Its incidence ranged from 8% to almost 50% in previous series (12, 24). In the current study, almost one-fifth of patients with aortic dissection involving the abdominal branch vessels had renal atrophy. Our findings revealed that the left renal artery was more prone to having type 3 perfusion, which may have led to a higher percentage of renal atrophy. In a study by Barnes et al., the left renal artery was more prone to arise from the false lumen (equivalent to type 3 perfusion) than the right renal artery (20% vs. 7%), which is consistent with our findings (24). This phenomenon may be explained by the pathophysiology of aortic dissection. As the dissection flap propagates in the descending thoracic aorta, it tends to lie posterolaterally and to the left of the true channel down to the diaphragm (15). As a result, the LRA has the highest frequency of type 3 perfusion.
The kidneys can sustain an ischemic insult early in the course of dissection. In the setting of aortic dissection, an absent or delayed nephrogram on CT may be suggestive, but not conclusive, of ischemia (9). This is because difference in the transit time between the true lumen and false lumen can also result in delayed contrast enhancement in kidneys supplied by separate lumina (9). In our series, nearly 40% of patients with late renal atrophy had a delayed or absent nephrogram on initial CT. It is possible that in these patients, renal atrophy stemmed from both the initial ischemic event caused by aortic dissection and repeated thrombosis of the false lumen. On the other hand, 60% of patients with late renal atrophy had normal renal enhancement on initial CT. Therefore, the initial ischemic insult may play a role in the development of late renal atrophy, but the ongoing hazard of postoperative false lumen thrombosis may be a more important risk factor. The patient with bilateral diminished renal parenchymal enhancement and global decreased visceral enhancement on initial CT because of circulatory shock demonstrated a good example. Instead of bilateral renal atrophy, the patient developed left renal atrophy, probably contributed to a type 3 perfusion in left renal artery and partial thrombi of the false lumen.
The incidence of accessory or supernumerary renal arteries may vary according to race. In a previous study, accessory renal arteries were identified in one-third of patients (25). A cadaveric report from a South-east Asian population showed a relatively lower incidence of 4% (26). In our cohort, accessory renal arteries were observed in 7% of patients, predominantly on the left side. It is possible that thrombosis of the accessory renal artery could be a cause of focal renal atrophy. However, the small number of patients with focal renal atrophy and accessory renal artery in our cohort precludes strong validation of this correlation.
Turbulent flow may lead to thrombi in the false lumen. Complete thrombosis of the false lumen with a subsequent reduction in flow may decrease the risk of progressive aortic dissection or rupture. Tsai et al. analyzed the outcomes of patients with type B acute aortic dissection who survived during initial hospitalization. In patients with partial thrombosis of the false lumen, the risk of death increased by a factor of 2.7 compared with patients with a completely patent false lumen (6). The factors explaining the poor prognosis of this patient group have not yet been validated. Our study found that postoperative partial thrombi in the false lumen above the renal arteries were significantly related to the development of renal atrophy. In this series, 68.8% of patients had partial thrombi in the false lumen, which may dislodge and result in repeated renal infarction and atrophy. It is assumed that perfusion may be disturbed in organs with combined true and false lumen perfusion as well as those with only false lumen perfusion. However, this assumption was not supported by our statistical analysis. We speculate that the dual blood supply from both true and false lumens may compensate for the disturbance of perfusion following thrombosis of the false lumen.
Predicting renal atrophy based on dissection flap anatomy may play a role in clinical practice. Studies have established that renal failure in the setting of acute aortic dissection is associated with lethal multiple organ failure (21–23). Moreover, long-term renal malperfusion can lead to atrophy and renal dysfunction. Although in most cases one kidney will suffice in maintaining renal function, predictions regarding future renal atrophy can alert the clinician about the importance of further renal protection strategies, since most patients with aortic dissection have comorbidities such as hypertension or atherosclerosis and are at high risk for chronic renal insufficiency (5).
There were several limitations in our study. First, this study did not quantify or correlate the severity of renal atrophy with laboratory data such as blood urea nitrogen, serum creatinine levels, or the glomerular filtration rate. Serum creatinine levels may be normal in cases of renal atrophy, which was unilateral in all our patients. Second, arterial pressure measurements, arteriography, and intravascular ultrasonography were not performed. Third, due to limitations in the technique and the availability of devices, endovascular interventions such as stenting or fenestration were not performed in order to reduce complications from renal malperfusion syndrome, which was fortunately unilateral in all cases. Fourth, the majority of patients in our cohort received an aortic interposition graft without fenestration at the distal anastomosis, and consequently false lumen flow stasis ensued. The results of our survey also reflect renal atrophy due to reduced false lumen flow. This atrophy would be expected to reach a maximum in those organs with only false lumen perfusion.
In conclusion, this is the largest series describing the correlation of aortic dissection with late renal atrophy to date. Our study found that perfusion of the left renal artery exclusively from the false lumen in association with partial thrombi proximal to the bilateral renal arteries is significantly associated with the development of renal atrophy. It is noteworthy that false lumen stasis following surgical repair of the proximal descending aorta may also have contributed to this renal artery compromise.