
Abstract
Background
FDG-PET/CT is increasingly being used for breast cancer staging. Its diagnostic accuracy in comparison to ultrasound as the standard non-invasive imaging modality for the evaluation of axillary lymph nodes has yet not been evaluated.
Purpose
To retrospectively compare the diagnostic value of full-dose, intravenously contrast-enhanced FDG-PET/CT and ultrasound for the detection of lymph node metastases in breast cancer patients.
Material and Methods
Ninety patients (one patient with a bilateral carcinoma) (89 women, one man; mean age, 55.5 +/− 16.6 years) suffering from primary breast cancer underwent whole-body FDG-PET/CT and axillary ultrasound. The ipsilateral axillary fossa (n = 91) was evaluated for metastatic spread. The sensitivity, specificity, the positive predictive value (PPV), negative predictive value (NPV), and accuracy of both methods were calculated. The sensitivity and accuracy were statistically compared using the McNemar Test (P <0.05). Analyses were made on a patient basis. The number of patients with extra-axillary locoregional lymph node metastases exclusively detected by FDG-PET/CT was evaluated. For axillary lymph node metastases histopathology served as the reference standard.
Results
The sensitivity, specificity, PPV, NPV, and accuracy of FDG-PET/CT for the detection of axillary lymph node metastases were 54%, 89%, 77%, 74%, and 75%, respectively. For ultrasound it was 38%, 78%, 54%, 65%, and 62%, respectively. FDG-PET/CT was significantly more accurate than ultrasound for the detection of axillary lymph node metastases (P = 0.019). There was no statistically significant difference between the sensitivity of both modalities (P = 0.0578). FDG-PET/CT detected extra-axillary locoregional lymph node metastases in seven patients (8%) that had not been detected by another imaging modality.
Conclusion
Though more accurate compared to ultrasound for evaluating the axillary lymph node status FDG-PET/CT is only as sensitive as ultrasound when it comes to the detection of axillary lymph node metastases. Due to the low sensitivity FDG-PET/CT cannot act as a substitute for Sentinel lymph node biopsy. FDG-PET/CT is able to detect previously unknown locoregional extra-axillary lymph node metastases.
Breast cancer is the most common newly diagnosed cancer type and the second most common cause of cancer-related death among women in the USA (1). It is expected to account for approximately one-third of all new cancer cases among US female patients (1). For estimating the duration of survival the axillary lymph node status is the most important prognostic factor (2). The 10-year survival rate in patients with axillary lymph node metastases depends on the number of involved nodes and ranges from 30% (>10 nodes) to 90% in those women without axillary lymph node metastases (3). The axillary lymph status is not only important for estimating the prognosis of patients with breast cancer but also for the decision on the individual treatment regimen (3). Today a surgical staging approach, using either Sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND) is the most accurate approach to stage the axilla (4). To plan the therapeutic strategy, however, it is desired to determine the axillary lymph node status preoperatively (5).
For non-invasive detection of axillary lymph node metastases manual palpation has a well-known low sensitivity and specificity (6), not valid to predict the accurate axillary lymph node status (7). Today ultrasound is the most commonly used imaging procedure to investigate the axilla, but also yields only a moderate diagnostic accuracy (8–10). A lot of non-invasive – either solely morphologic or functional – techniques such as scintimammography, high-resolution computed tomography (CT), contrast-enhanced magnetic resonance imaging (MRI), and positron emission tomography (PET) have been tested, but also have only limited use (11–15). Nowadays the staging of the axillary lymph node is done invasively by identifying the sentinel lymph node(s) by lymphatic mapping with a following SLNB (4,16). If the Sentinel lymph node harbors metastases in most cases an ALND follows (4).
In the last decade positron emission tomography/ computed tomography (PET/CT) has become an established imaging modality for different cancer types (17). The addition of morphologic CT data to metabolic [18F]-fluoro-deoxyglucose (FDG) PET data to combined anato-metabolic imaging increased the diagnostic accuracy over CT and PET alone (18). Recently, whole-body FDG-PET/CT is also increasingly used for breast cancer staging and treatment monitoring, revealing its diagnostic potential by detecting previously unknown metastases (19–23). However, there is little evidence concerning the diagnostic accuracy for axillary lymph node staging (10). Furthermore there is only one study using a full-dose, contrast-enhanced FDG-PET/CT protocol for the evaluation of the axilla, however not comparing the results with those of ultrasound (8).
The aim of this retrospective study was: (a) to compare the diagnostic value of full-dose, intravenously contrast-enhanced FDG-PET/CT and ultrasound for the detection of axillary lymph node metastases; and (b) to define the number of patients with previously unknown locoregional lymph node metastases.
Material and Methods
Patients
Between February 2007 and December 2010 90 breast cancer patients (mean age, 55.7 years; range, 25.4–84.3 years; standard deviation [SD], 8.1 years; 89 women, 1 man) underwent contrast-enhanced, full-dose FDG-PET/CT and axillary ultrasound for staging purposes. One patient suffered from a bilateral carcinoma, so the number of patients is 90 and the number of the axillary fossae used is 91. Sixty-nine patients suffered from histopathologically proven ductal carcinoma, 13 from lobular carcinoma, three from micropapillary carcinoma, and one each from a tubular, mucinous, apocrine, medullary, and neuroendocrine carcinoma; one patient had a ductal carcinoma in situ. (y)pT stage was as follows: pTx, three patients; ypT0, 10 patients; pTis, three patients; pT1, 38 patients; pT2, 29 patients; pT3, six patients; pT4, two patients. The pN stage was as follows: pN0, 54 patients; pN1, 24 patients; pN2, seven patients; pN3, six patients. The grading was as follows: GX, six patients; G1, 11 patients; G2, 45 patients; G3, 29 patients. No patient had undergone any kind of local or systemic treatment prior to imaging. All patients were consecutive examined concerning these inclusion criteria. One patient suffered from bilateral breast cancer. The study was performed in accordance with the regulations of the local ethics committee and federal laws.
Whole-body FDG PET/CT
All investigations were performed as full-dose, contrast-enhanced PET/CT scans. The patients had been instructed to fast for a minimum of 6 h before FDG injection. All patients had blood glucose levels below 150 mg/dL at the time of FDG injection. They received an intravenous application of 270±40 MBq of FDG (210–360 MBq). After FDG application, 1.000 mL of a water-based oral contrast agent was applied for bowel marking (24). Sixty minutes after intravenous application of FDG imaging was started (beginning with the CT scan) covering an area from the skull base to the upper thighs. Patients were either scanned on a biographTM PET/CT (Siemens Molecular Imaging, Hoffmann Estates, IL, USA) (n = 57) or a mCTTM PET/CT system (Siemens Molecular Imaging, Hoffman Estates, IL, USA) (n = 33) after application of intravenous contrast material.
Procedural and technical data for both scanners were: (a) biographTM PET/CT: CT, 100 mA/s; 130 kV; 140 mL iodinated intravenous contrast material (Xenetrix 300TM, Guerbet, Sulzbach, Germany); contrast material injection by an automated injector (XD 5500TM; Ulrich Medical Systems, Ulm, Germany); biphasic injection technique (flow rate of 3 mL/s for the first 90 mL and 1.5 mL/s for the following 50 mL); start delay, 50 s; slice thickness, 5 mm; increment, 2.4 mm. PET: mode, 3D; emission time, 3.5 min per bed position; image reconstruction, iterative algorithms (FORE and AWOSEM, non-linear); two iterations; eight subsets; filter, FWHM 5.0 mm; scatter correction; and (b) mCTTM: 210 mA/s; 120 kV; automatic dose modulation (CareDoseTM); 100 mL iodinated intravenous contrast material (Xenetrix 300TM, Guerbet, Sulzbach, Germany); contrast material injection by an automated injector (StellantTM DCT Injection System, Medrad, Duesseldorf, Germany); monophasic injection technique (flow rate of 2 mL/s); start delay, 70 s; slice thickness, 5 mm; increment, 5.0 mm. PET: mode, 3D; emission time, 2.0 min per bed position; image reconstruction, iterative algorithms (FORE and AWOSEM, non-linear); four iterations; eight subsets; filter, FWHM 4.0 mm; scatter correction.
Image analysis
For image evaluation an AW SuiteTM 5.5.3e Volume viewer plusTM Workstation (GE Healthcare, Munich, Germany) was used. This workstation was connected to a picture archiving and communication system (PACS) workstation (GE Healthcare, Munich, Germany). A radiologist and a nuclear medicine physician (each with >5 years of experience in reading PET/CT scans) analyzed the FDG-PET/CT data unaware of the histopathological gold standard. Diagnoses were made in consensus. All scans were evaluated in three orthogonal planes (axial, coronal, and sagittal). The ipsilateral axillary fossa was evaluated for the presence of metastatic spread using the proceeding of Heusner et al., with the exception that lymph nodes of every size were evaluated (8). Image analysis was done as follows: first all lymph nodes were noted on CT, followed by FDG-PET evaluation for any focally increased PET signal. Any focus which could be mapped to a lymph node and was considered elevated above normal was rated as positive for metastasis. Non-elevated PET signal or such considered compatible with physiologic lymphatic uptake was rated negative. The lymph nodes’ sizes themselves did not directly enter the final PET/CT finding but were indirectly considered with respect to the intensity of the PET signal. In short, a given PET focus was rated positive in a small lymph node rather than in a large lymph node – accounting for partial volume effects. According to this approach a PET focus being rated positive or negative with respect to a given lymph node constituted the final PET/CT finding. The decision was an empiric one being based on the long-term imaging experience of the two readers. Quantitative measurements such as standardized uptake values on PET were not used for decisionmaking. Furthermore the maximal standardized uptake value (SUV max) of the ipsi-lateral axillary lymph nodes was determined. From these results averages, ranges and standard deviations of the true-negative, true-positive, false-negative, and false-positive axillary lymph nodes were defined. Following the staging system of the American Joint Committee on Cancer (AJCC) other locoregional lymph nodes were additionally evaluated for metastatic spread (25) and the number of patients with locoregional, extra-axillary lymph node metastases not detected by the conventional staging algorithm was determined. This conventional staging algorithm includes: clinical examination of breast and local lymph nodes, X-ray mammography, ultrasound of breast and axilla, ultrasound of the liver, bone scintigraphy, and MR mammography in several cases (26).
Axillary ultrasound examination
Axillary ultrasound examinations (AUS) were performed by or under supervision of a consultant gynecologist specialized in senology using an Siemens Acuson AntaresTM (Siemens Medical Solutions, Erlangen, Germany) ultrasound system equipped with a linear array transducer at a frequency of 11.4 MHz. AUS criteria positive for axillary lymph node metastases were: enlargement of lymph nodes with short axis diameters of 10 mm or more, oval (not bean-shaped without typical fatty hilus) or even, round shape, homogeneously hypoechoic and thickening of cortex, cortical thickness of more than 3 mm in the short axis diameter (diffuse or focal), infiltration of surrounding tissue, a distortion of the lymph nodes architecture, or a dislocation of the hilum. Axillary fossae were imaged by ultrasound in the transverse as well as the sagittal plane. Additional ultrasound-guided biopsies of axillary lymph nodes were not performed.
Gold standard
Histopathological findings of ALND (n = 15), SLNB (n = 70), or both (SLNB and subsequent ALND, n = 6) served as the gold standard. The decision whether to perform SLNB or ALND was based on the synopsis of ultrasound and FDG-PET/CT findings; at least two surgeons specialized in senology made the decision whether to perform an ALND or SLNB in consensus. Histological work-up of all lymph node specimens was performed according to the guidelines of the German Society of Senology (26). For the sentinel node procedure, each lymph node was cut into 2 mm slices. After complete embedding 3 to 7 stepwise H&E stained sections were cut from each paraffin block in levels of 500 μm distance. In ALND specimen all lymph nodes were carefully removed from the adipose tissue and sorted by size. Lymph nodes up to 4 mm in minimum diameter were embedded in total, larger lymph nodes were cut into 3 mm slices and completely embedded, allowing the histological count of the nodes. One H&E stained slide was cut from each paraffin block in ALND specimens. Immunohistochemistry for the detection of isolated tumor cells was not routinely performed.
Statistical analysis
The following parameters for the detection of ipsilateral axillary lymph nodes both with FDG-PET/CT and ultrasound were analyzed compartment-based: sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy. The diagnostic sensitivity and accuracy of both methods was compared using the McNemar test. A P value <0.05 was considered to be statistically significant.
The number of patients with locoregional, extra-axillary lymph node metastases not detected by the conventional staging algorithm (26) was determined.
Results
According to the reference standard 54 axillary fossae did not harbor ipsilateral axillary lymph node metastases, whereas 37 did. According to histopathology the mean number of axillary lymph node metastases was 5 (range, 1–30; SD, 7).
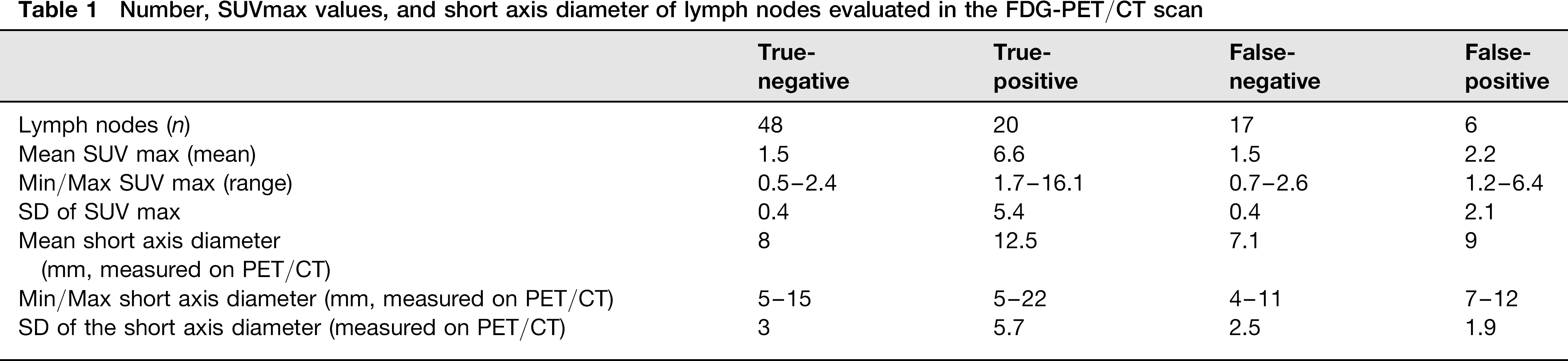
FDG-PET/CT was true-negative (TN) in 48 axillary fossae with a mean SUVmax of 1.5 (range, 0.5–2.4; SD, 0.4) and a mean short axis diameter of the lymph nodes of 8 mm (range, 5–15 mm; SD, 3 mm, measured in the CT part of FDG-PET/CT). FDG-PET/CT was true-positive (TP) in 20 axillary fossae with a mean SUVmax of 6.6 (range, 1.7–16.1; SD, 5.4) and a mean short axis diameter of 12.5 mm (range, 5–22 mm; SD, 5.7 mm). FDG-PET/CT was false-negative (FN) in 17 axillary fossae with a mean SUVmax of 1.5 (range, 0.7–2.6; SD, 0.4) and a mean short axis diameter of 7.1 mm (range, 4–11 mm; SD, 2.5 mm). FDG-PET/CT was false-positive (FP) in six axillary fossae with a mean SUVmax of 2.2 (range, 1.2–6.4; SD, 2.1) and a mean short axis diameter of 9 mm (range, 7–12 mm; SD, 1.9 mm) (Table 1, Fig. 1). For ultrasound the results were as follows: 42 TN, 14 TP, 23 FN, and 12 FP.
Number, SUVmax values, and short axis diameter of lymph nodes evaluated in the FDG-PET/CT scan
Axial CT (A), FDG-PET (B), and fused FDG-PET/CT (C) show a histopathologically proven lymph node metastasis in the left axilla missed by ultrasound (small axis diameter of the lymph node metastasis: 5 mm (measured on PET/CT, SUVmax: 9.2)
The sensitivity, specificity, PPV, NPV, and accuracy of FDG-PET/CT for the detection of ipsilateral axillary lymph node metastases was 54%, 89%, 77%, 74%, and 75%. The corresponding values for ultrasound were 38%, 78%, 54%, 65%, and 62%, respectively. The diagnostic accuracy of FDG-PET/CT was significantly higher than that of ultrasound for the evaluation of the axillary lymph node status (P = 0.0190). However, FDG-PET/CT was as sensitive as ultrasound for the detection of axillary lymph node metastases (P = 0.0578).
FDG-PET/CT was TP but ultrasound FN for the detection of axillary lymph node metastases in eight axillary fossae. The mean small axis diameter of axillary lymph nodes was 11 mm (5–22 mm; SD, 6 mm). Ultrasound was TP but FDG-PET/CT FN in two axillary fossae. The mean small axis diameter of axillary lymph nodes was 8 mm (4–11 mm; SD, 5 mm). On the other hand, FDG-PET/CT was TN but ultrasound FP in nine axillary fossae. The mean small axis diameter was 8 mm (5–12 mm; SD, 2 mm). Ultrasound was TN but FDG-PET/CT FP in three axillary fossae. The mean small axis diameter was 12 mm (7–15 mm; SD, 4 mm). In seven patients (8%) 13 extra axillary, locoregional lymph node metastases were present. These lymph node metastases were detected only by FDG-PET/CT: nine lymph node metastases were localized at the internal mammarian artery (stage N2b in one patient, stage N3b in three patients, stage N3c in one patient); one lymph node was localized supraclavicularly (same patient as mentioned before [stage N3c]); one lymph node was localized infraclavicularly (N3a in one patient), two lymph nodes were localized beside the ipsilateral internal jugular vein (N3c in one patient) (Fig. 2a–c) (23).
(a) Axial CT (A), FDG-PET (B), and fused FDG-PET/CT (C) of patient with extra-axillary locoregional lymph node metastases. These lymph node metastases were solely detected by FDG-PET/CT: ipsilateral (left) internal mammary lymph node metastasis with a small axis diameter of 6 mm (measured on PET/CT) and a SUVmax 6.1. (b) Axial CT (A), FDG-PET (B), and fused FDG-PET/CT (C) of patient with extra-axillary locoregional lymph node metastases. These lymph node metastases were solely detected by FDG-PET/CT: ipsilateral supraclavicular lymph node metastasis in a lymph node besides the internal jugular vein with a small axis diameter of 7 mm (measured on PET/CT) and a SUV max of 2.9. (c) Axial CT (A), FDG-PET (B), and fused FDG-PET/CT (C) of patient with extra-axillary locoregional lymph node metastases. These lymph node metastases were solely detected by FDG-PET/CT: ipsilateral infraclavicular lymph node metastasis in a lymph node with a small axis diameter of 6 mm (measured on PET/CT) and a SUV max of 3.7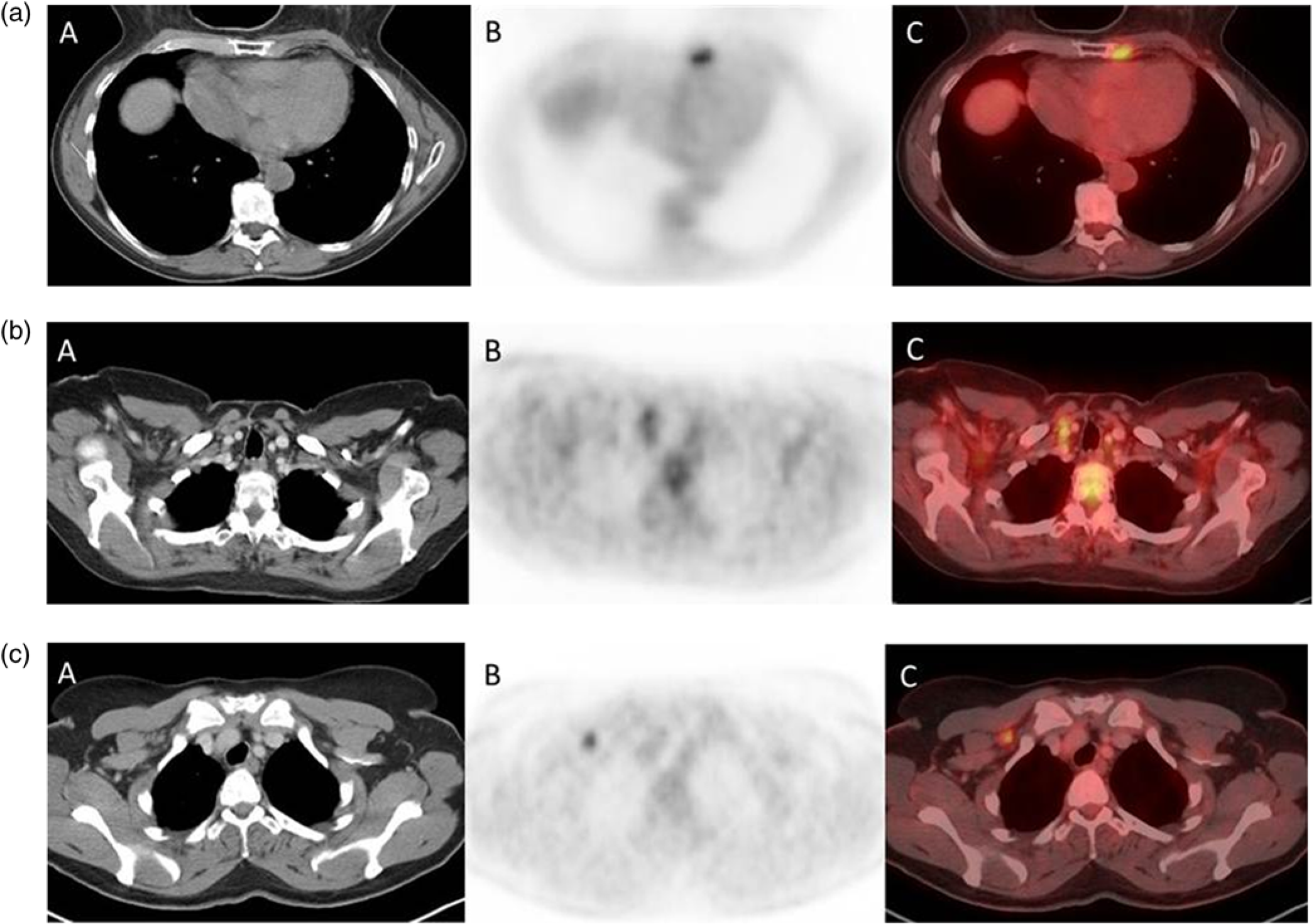
Discussion
Although more accurate than ultrasound for the evaluation of the axillary lymph node status FDG-PET/CT showed an only moderate sensitivity – not higher than that of ultrasound – for the detection of axillary lymph node metastases (P = 0.0578). Due to the higher diagnostic accuracy of FDG-PET/CT compared to ultrasound a standardized axillary sonography may be dispensable in patients undergoing FDG-PET/CT for whole-body staging purposes. However, due to the low sensitivity invasive axillary staging procedures have still to be carried out. One advantage of FDG-PET/CT is that it detects previously unknown locoregional extra-axillary lymph node metastases, which are not captured by the conventional staging algorithm (26).
The significant higher accuracy of FDG-PET/CT compared to ultrasound may be explained by its combination of morphological and functional criteria, as well as by the FDG avidity of most breast cancer lesions (27). However, a sensitivity of 54% and an accuracy of 75% are clearly far away from highly sensitive and accurate. This limitation may be explained by the incapability of FDG-PET/CT for detecting micrometastases with a diameter of 0.2–2 mm within lymph nodes (28); based on the limited spatial resolution of PET micrometastases cannot be detected. The consequence is that invasive staging procedures (SLNB and ALND) are still mandatory to avoid missing small axillary metastases.
Using FDG-PET/CT as a preinvasive axillary staging modality offers another interesting option: As discussed in the literature it can be used as a pre-test before surgery especially in patients with large primary breast cancer lesions and thus can extend the indication for SLNB instead of ALND (8). In patients with large tumors with a high probability for harboring axillary lymph node metastases the NPV of SLNB falls below acceptable levels, so SLNB runs the risk to be falsely negative (8). Using FDG-PET/CT as a pre-test before invasive staging procedures, SLNBs can be used instead of ALNDs in the case of unremarkable FDG-PET/CT scans even in patients with large tumors to avoid unnecessary ALNDs and associated morbidity. SLNB can be performed in these patients without falling below a NPV level of 95% and as a consequence patients with tumor sizes up to 5 cm can be triaged to SLNB (8).
FDG-PET/CT is mainly performed for purposes of whole-body staging with the advantage to include all locoregional lymph nodes as well as distant sites of potential metastases. Whole-body staging may, thus, be performed in a single session reducing the time to definite therapy decision. This is important because the aim of every breast cancer therapy is to eliminate or at least reduce metastatic lesions at the best (29). Due to costs, availability, and radiation exposure FDG-PET/CT will not replace axillary ultrasound; however, if a FDG-PET/CT scan is performed for staging purposes anyway a subsequent ultrasound may be dispensable.
There are several publications in the recent literature dealing with the diagnostic value of FDG-PET and not intravenously contrast-enhanced, low-dose FDG-PET/CT for the detection of axillary lymph node metastases (10); these studies were performed with different protocols compared to our study (PET-only, non-contrast-enhanced FDG-PET/ CT). To our knowledge our study is the first one that compares the diagnostic accuracy of a “fully-diagnostic” full-dose, intravenously contrast-enhanced FDG-PET/CT protocol with axillary ultrasound, enabling to evaluate morphological features of axillary lymph nodes additionally to the FDG-PET signal.
This study has limitations: Apart from the retrospective study design we did not allocate findings on ultrasound and FDG-PET/CT to specific histopathological specimen. This was the reason why we decided to abandon a lesion-based analysis. However, we rate the decision how to deal with the axilla is dichotomic: If the axillary fossa harbors metastases the patient has to undergo ALND with resection of all detectable lymph nodes. In cases of negative imaging findings SLNB has to prove the histopathological absence of metastases. The sensitivity of only 38% for the detection of axillary lymph node metastases with ultrasound is lower compared to some sensitivities reported in the literature: Ueda et al., for example, reported a sensitivity of 54% (10); Ahn et al. even reported a sensitivity of 79.5% (30). Monzawa et al., however, reported a sensitivity of only 33% (31); the difference between our sensitivity and the high sensitivities reported in the literature be a result of the course of action with axillary ultrasound: although a senior senologist supervised all ultrasound investigations performed not by himself some lymph node metastases may be missed as it is a known limitation of ultrasound's accuracy to be strongly investigator dependent. This might have artificially deteriorated the sensitivity of ultrasound. Another reason may be different criteria used in different studies for the definition of an axillary lymph node to be malignant (9). Another limitation might be the fact that a PET focus being rated positive or negative with respect to a given lymph node constituted the final PET/CT finding. The decision was an empiric one being based on the long-term imaging experience of the two readers. While this is a subjective evaluation mode we decided to use this algorithm due to the well-known fact that many breast cancer lesions show only a mild FDG uptake.
In conclusion, full-dose, i.v. contrast-enhanced FDG-PET/ CT may be more accurate than ultrasound for the detection of ipsilateral axillary lymph node metastases in breast cancer patients. An axillary ultrasound investigation may, therefore, be dispensable in patients undergoing “fully-diagnostic” FDG-PET/CT for staging purposes. By detecting locoregional extra-axillary lymph node metastases FDG-PET/CT contributes to a correct locoregional staging in a relevant number of patients. However, based on its overall moderate sensitivity for the detection of axillary lymph node metastases (that is not higher than the sensitivity of ultrasound) it clearly cannot replace invasive axillary staging approaches.