
Abstract
Background
Totally implantable venous access devices (TIVAD) may be associated with different complications. Certain mechanical port disorders can easily be diagnosed on chest radiographs if the implanted systems are radiopaque and well visible. There are no reports regarding the visibility of TIVAD on chest X-rays.
Purpose
To assess the radio opacity of TIVAD implanted in the chest as well as type and frequency of mechanical complications of ports on chest X-ray images.
Material and Methods
Chest X-rays of 985 patients from the time period 2007-2009 were analyzed retrospectively. In these patients 1190 TIVAD were inserted. All parts of the TIVAD, i.e. port chamber, connection, and port catheter, were checked for their visibility on chest radiographs. An opacity score was used here as follows: ++ well visible; + visible; - partly or completely invisible. Mechanical complications of TIVAD incidentally detected on chest X-ray were also analyzed retrospectively.
Results
Nineteen TIVAD models with diverse configuration and visibility of port chambers, connections, and catheters were identified in our study. Eighty-eight percent of the analyzed port systems were well visible or visible on chest radiographs. Twelve percent of the port chambers and catheters were partly visible or completely invisible. In 9% of the TIVAD, different mechanical complications were diagnosed on chest X-ray images.
Conclusion
TIVADs should be evaluated carefully on every chest X-ray. Ideally, they should be radio-opaque and well visible on thoracic X-ray images. Unfortunately, this is not always the case. Therefore, manufacturers of TIVAD should take into consideration to use exclusively radio-opaque materials that allow sufficient visibility of each port component on chest radiographs.
Totally implantable venous access devices (TIVAD) or ports are valuable and efficient instruments for long-term intravenous treatment of patients with malignant diseases, frequent blood sampling, stem cell transplantation, parenteral nutrition, and for injections of contrast media during radiological investigations, such as computed tomography (CT) (1–6). However, their use may be associated with different complications (7–16) like catheter-related infections, venous thrombosis, extremity swelling, catheter tip migration, venous perforation, cardiac perforation, cardiac arrhythmia, inadvertent device removal, catheter-port/hub connection failure, catheter fracture, catheter occlusion/fibrin sheath formation, catheter erosion through vessel wall, erosion of port/catheter through the skin, infusate infiltration around access device, and inability to access the device (1, 2, 5, 10–18). Certain mechanical port problems occur clinically silent and can cause secondary hazardous sequelae such as cardiac arrhythmia or pulmonary embolism (7,11,13). Some mechanical complications of chest ports, such as chamber rotation, catheter tip migration, port disconnection, and complete catheter fracture can be diagnosed on thoracic radiographs if the implanted systems are radio-opaque and well visible (19).
Nowadays, multiple diverse models of TIVAD are used. However, to the best of our knowledge, there are no reports regarding the visibility of TIVAD on chest radiographs. Therefore, the purpose of this study was to assess the radio opacity of implanted ports and the prevalence and location of mechanical complications of TIVAD incidentally identified on chest X-ray images.
Material and Methods
The study was approved by our institutional ethic commission.
Chest X-rays of 985 patients during the time period from 2007 to 2009 were analyzed by two radiologists (AS and CR with 9 and 3 years of experience in thoracic imaging, respectively) on PACS (Picture Archiving and Communication System) retrospectively. There were 504 women and 481 men with a median age of 59 years (range, 17–87 years), mean age 57 ± 14 years. The chest X-ray images were performed for restaging or follow-up investigations and for diagnosis of several cardiopulmonary disorders, such as pneumonia, stasis, pleural, or pericardial effusion. X-ray images were obtained by radiographic equipment Bucky Diagnost (Philips Medical Systems, Amsterdam, The Netherlands). Typical imaging parameters were 125 kV and mAs of 07–1.2. In these patients 1190 TIVAD were inserted during this time. A total of 963 (97.8%) patients had one port, and 22 (2.2%) patients had two ports during this time.
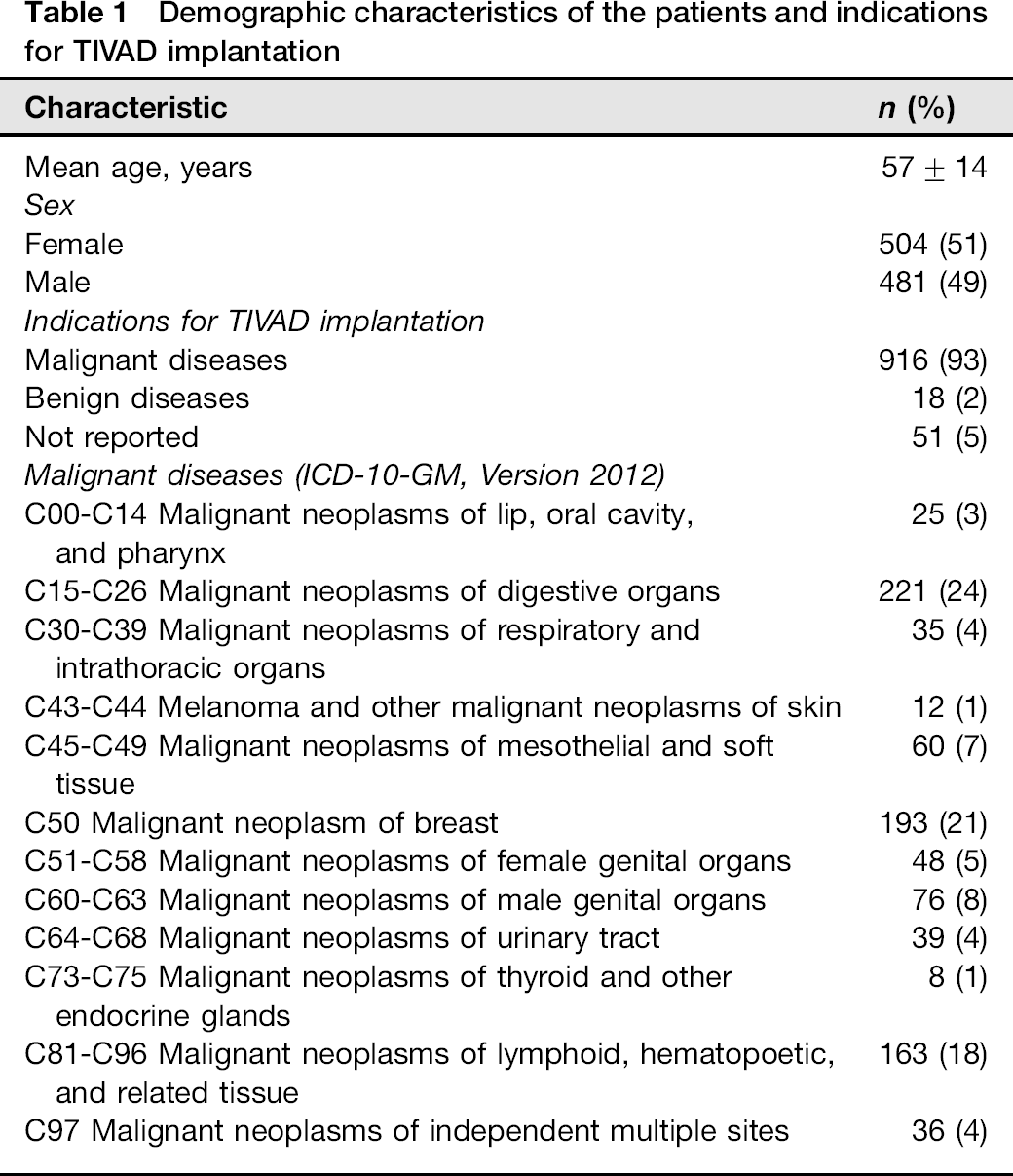
Indications for TIVAD implantation are listed in Table 1. Ninety-three percent of the ports were implanted for chemotherapy and 2% for parenteral nutrition, intravenous infusions, and/or application of antibiotic and other drugs. In 5% of the cases the cause of port implantation was not known. Most of the ports were inserted via subclavian veins (n = 1174, 99%). Sixteen devices (1%) were implanted via jugular veins.
Demographic characteristics of the patients and indications for TIVAD implantation
All parts of the TIVAD, i.e. port chamber, connection, and port catheter, were checked retrospectively for their visibility on chest radiographs. An opacity score was used here as follows: ++ well visible; + visible; – partly or completely invisible (Figs. 1–4).
Model 1 of the analyzed TIVAD (Baxter Health port, Baxter Healthcare SA, Zurich, Switzerland). Visibility on thoracic X-ray: chamber ++, connection ++, catheter ++
Model 2 of the analyzed TIVAD (Braun Celsite®, B. Braun Medical, Boulogne Cedex, France). Visibility on thoracic X-ray: chamber +, connection +, catheter +
Model 3 of the analyzed TIVAD (Bard Port® with Groshong® catheter, C.R. Bard Access Systems, Inc., Salt Lake City, USA). Visibility on thoracic X-ray: chamber –, connection –, catheter –
Model 4 of the analyzed TIVAD (
Consensus of the investigators was obtained for the grading of each port.
In addition, mechanical complications of TIVAD incidentally detected on chest X-ray were also analyzed retrospectively.
Results
Nineteen TIVAD models with diverse configuration and visibility of port chambers, connections, and catheters were identified in our study (Table 2).
Distribution of radio-opacity of the identified TIVADs in our study

There were 19 different port systems regarding their configuration and visibility of port chambers, connections and catheters. In our hospital, four models were used (Table 3).
Implanted TIVAD models, their frequency, and radio-opacity
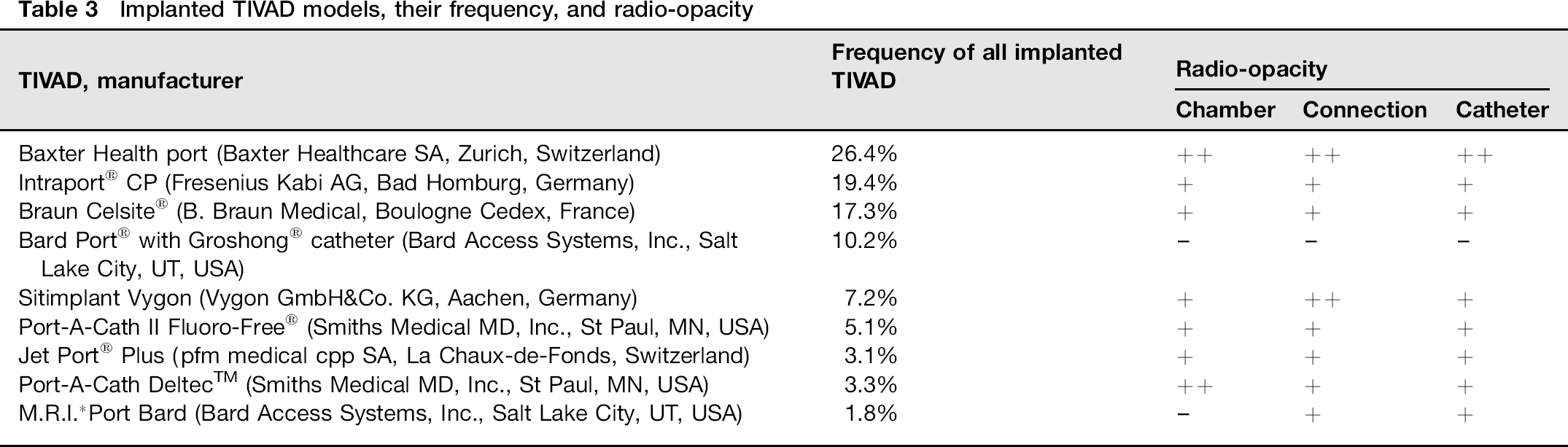
Baxter Health port (Baxter Healthcare SA, Zurich, Switzerland), Braun Celsite® (B. Braun Medical, Boulogne Cedex, France), Intraport® CP (Fresenius Kabi AG, Bad Homburg, Germany), and Bard Port® with Groshong® catheter (C.R. Bard Inc., Salt Lake City, UT, USA). The four port models used in our institution were implanted in 873 cases (73.3%). Five TIVAD models (20.5% of all identified ports) were inserted in neighboring hospitals: Sitimplant Vygon (Vygon GmbH&Co. KG, Aachen, Germany), Port-A-Cath II Fluoro-Free® and Port-A-Cath DeltecTM (Smiths Medical MD, Inc., St Paul, MN USA), Jet Port® Plus (pfm medical cpp SA, La Chaux-de-Fonds, Switzerland), and M.R.I.*Port Bard (Bard Access Systems, Inc., Salt Lake City, UT, USA). The frequency and visibility of the implanted TIVAD are shown in Table 3.
Type and manufacturer of 6.5% of devices implanted at other institutions were not known.
Eighty-eight percent of the analyzed port systems were well visible or visible on chest radiographs while 12% of the port chambers and catheters and 10% of the port connections were partly visible or completely invisible.
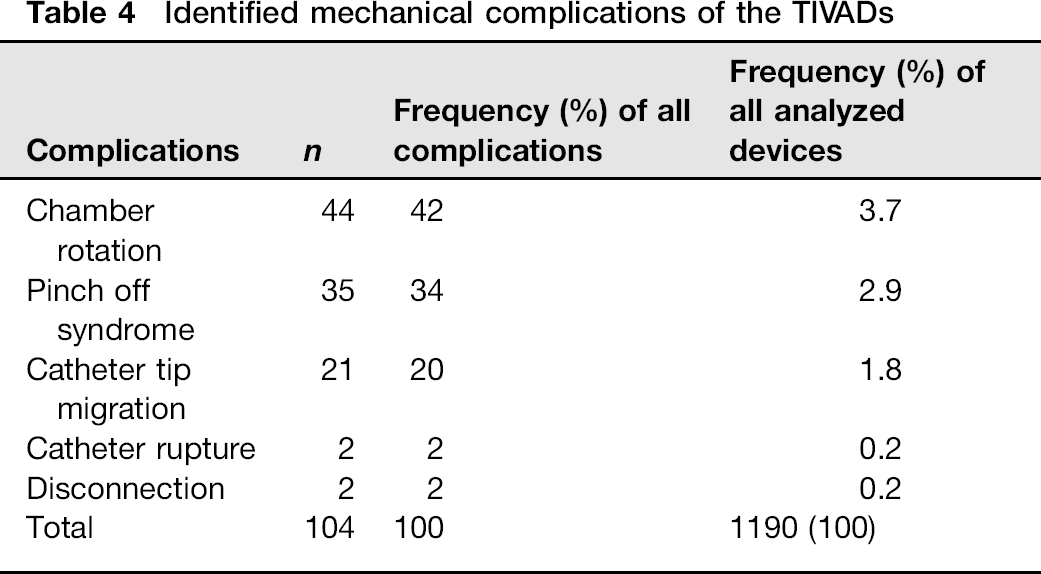
In 104 (9%) of the TIVAD, different mechanical complications (Figs. 5–7) were incidentally diagnosed on thoracic X-ray images (Table 4).
Partly rotated port chamber (twisted port chamber, arrow). Visibility of the TIVAD on thoracic X-ray: chamber ++, connection ++, catheter ++ (Baxter Health port)
Port catheter disconnection (white arrow) with catheter embolization in the superior cava vein and right atrium (black arrows). Port system visibility: chamber +, connection +, catheter + (Intraport® CP)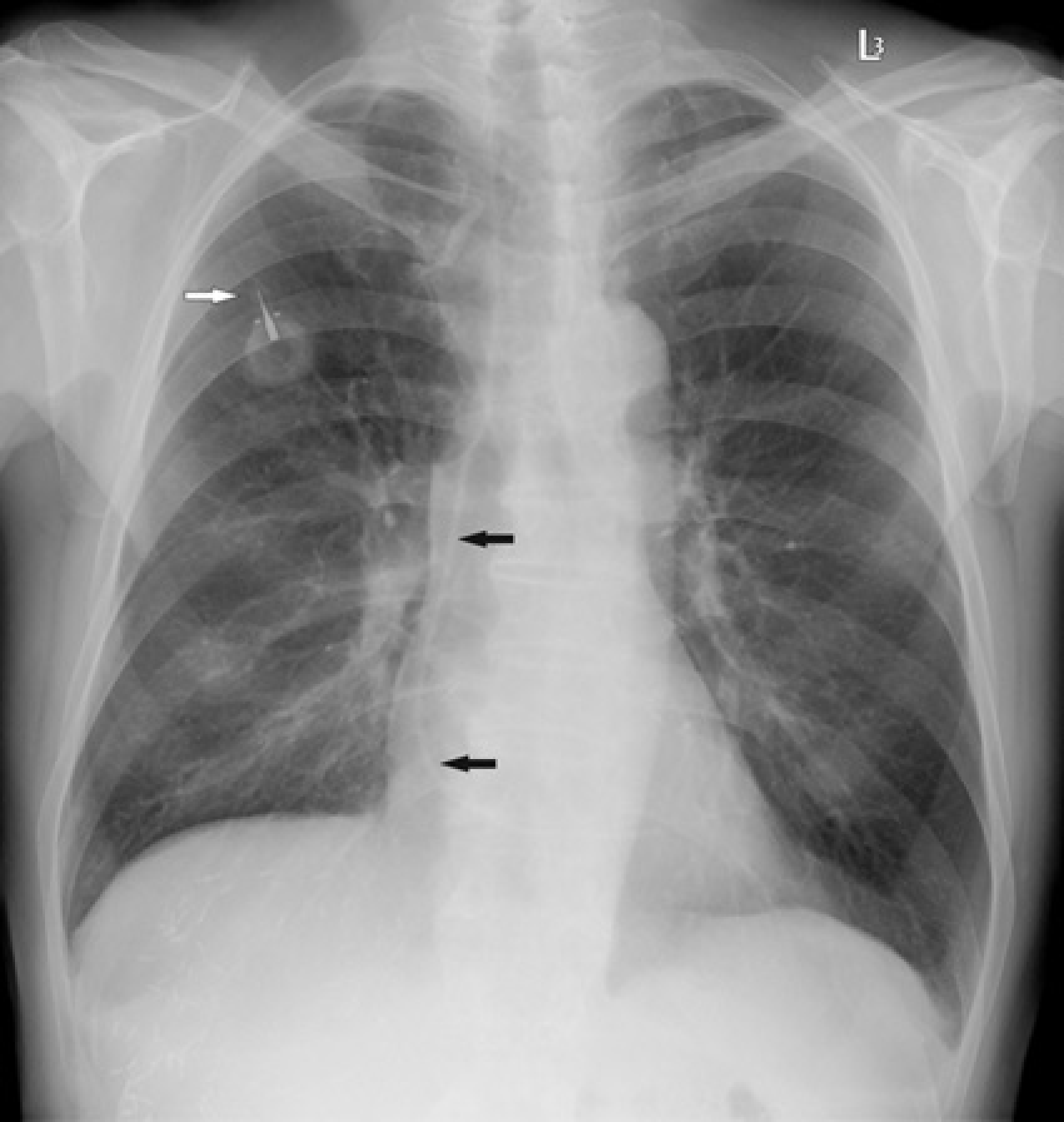
(a) Port catheter rupture (white arrow) with embolized catheter in the right atrium/right ventricle (black arrow). (b) Magnification view of the embolized catheter (black arrow). Port system visibility: chamber –, connection –, catheter – (Bard Port® with Groshong® catheter)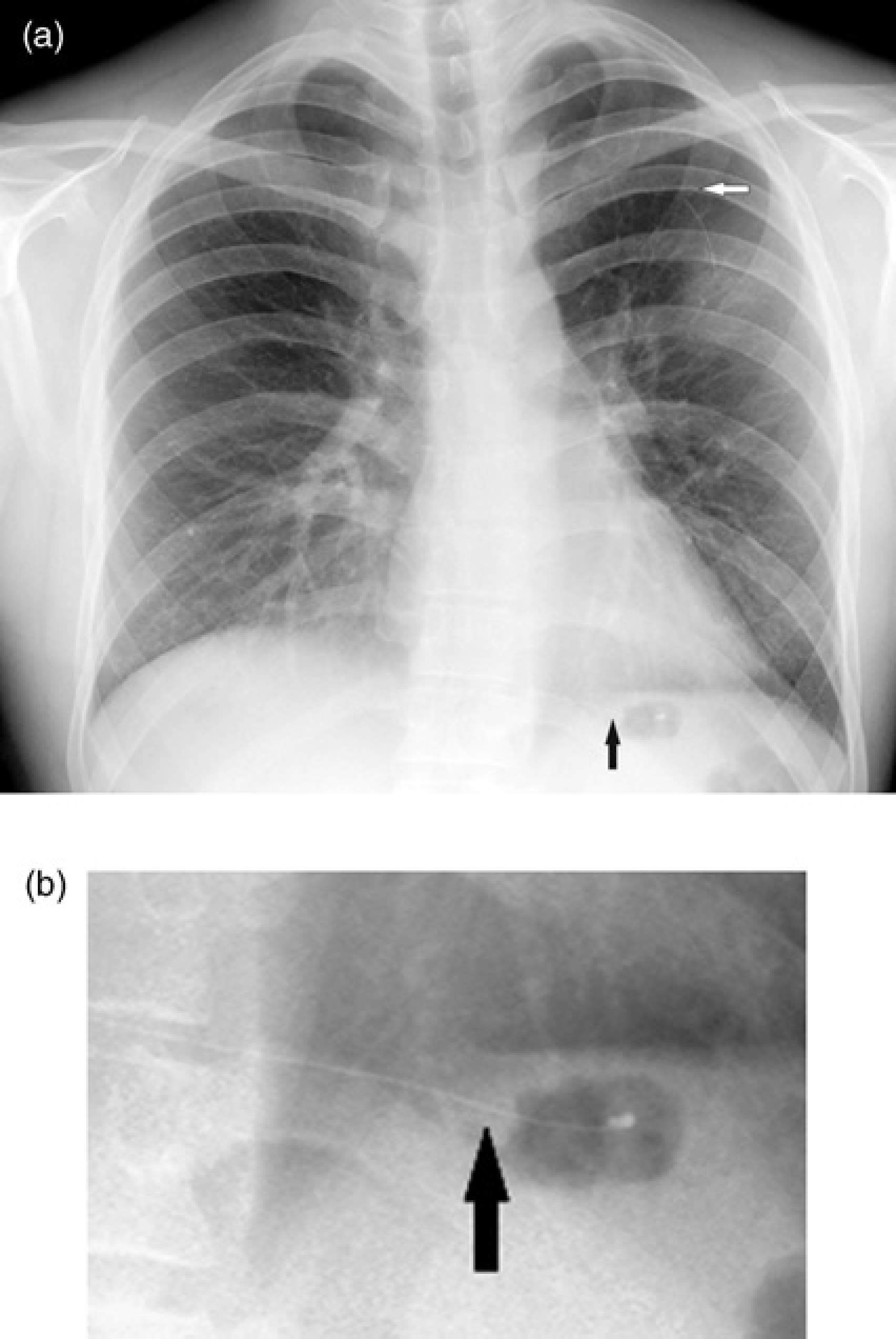
Identified mechanical complications of the TIVADs
Discussion
Port system insufficiency may manifest with several clinical signs, such as inability of blood aspiration, port occlusion, or soft tissue swelling (5, 6, 12–19). However, implanted ports are not always permanently used, for example in patients, in whom the port is kept implanted after the end of therapy or in therapy-free intervals. Chest X-ray images are often performed in patients for several reasons: to rule out a pneumonia or pleural effusion or to control the cardiac function (pulmonary edema). Although CT, positron emission tomography, and magnetic resonance imaging are often used for restaging and follow-up in oncologic patients, chest X-ray is also often performed to determine progression of the underlying disease (20,21). Several mechanical complications of pectorally placed implanted port systems, such as chamber dislocation, intravenous catheter migration, catheter retraction, disconnection, and catheter fracture can be identified on chest X-ray (5, 6, 11, 14–19, 22, 23). Our analysis showed that in 9% of the implanted ports complications were identified incidentally on thoracic X-ray. Many complications, especially intravascular catheter embolization are potentially hazardous and can result in severe cardiac arrhythmia or even death (7,11,17). Therefore, for any chest radiograph performed on patients with a pectorally placed port the position and integrity of the implanted TIVAD should be analyzed carefully. Furthermore, if a mechanical complication is suspected, the implanted TIVAD should be investigated clinically and by fluoroscopy because of its better resolution to diagnose leakage, fibrin sheath, or thrombus formation. Our study shows, however, that several port systems are totally or partially radiolucent and may therefore evade detection and evaluation on thoracic X-ray images. For this reason, several port complications may go undiagnosed for a prolonged time period.
The present study has several limitations. First, this was a retrospective analysis. Second, not every mechanical complication of implanted chest ports could be identified incidentally on chest X-ray images. Third, not every port type and manufacturer could be identified and therefore analyzed.
In conclusion, TIVADs should be evaluated carefully on every chest X-ray. Ideally, they should be radio-opaque and well visible on thoracic X-ray images. Unfortunately, this is not always the case. Due to this deficit, potentially severe complications may not be identified – a problem that could easily result in forensic consequences. Therefore, manufacturers of TIVAD should take into consideration to use exclusively radio-opaque materials that allow sufficient visibility on chest radiographs of each port component. The frequency of mechanical complications of TIVAD incidentally detected on chest X-ray is 9%.