
Abstract
The objective of this review is to highlight the pertinent imaging features and potential pitfalls in the diagnosis and staging of gall bladder carcinoma. This condition is notoriously non-specific on imaging on many occasions, particularly in its early stages; gall bladder carcinoma shows numerous features that overlap with a large number of benign conditions, leading to delayed diagnosis and incurable disease. Radiologists should be familiar with its typical and atypical imaging features.
Despite being the commonest biliary tract cancer, gall bladder carcinoma (GBCA) is a relatively rare cancer, accounting for 1–2% of all alimentary tract malignancies (1). Its importance lies in its overall poor outlook. GBCA usually presents at an advanced and inoperable stage, with an overall 5-year survival rate of 15–20% at the very best (2). Sixty percent of GBCA occurs in the fundus, 30% in the body, and 10% in the neck. Early diagnosis remains the only hope of cure, achieved primarily through surgery. Early GBCA, i.e. those confined to the gall bladder wall, may be treated with extended cholecystectomy with a reported 5-year survival rate of 90% (3).
Although the absence of a protective submucosal layer in the gall bladder wall may contribute to early local spread, the main reason behind delayed diagnosis of GBCA lies with its relatively vague early clinical presentation. Affected patients usually present with non-specific complaints similar to those of benign gall bladder diseases (such as indigestion and jaundice). Hence, early disease is rarely clinically suspected. The disease is often recognized by radiologists first – as an unexpected finding – when the patient is being investigated for suspected benign gall bladder disease. However, as with its clinical presentation, the radiological features of early GBCA are often non-specific and easily mistaken for those of benign diseases. Shukla et al. reported that 50% of incidental GBCA found on routine cholecystectomy specimens showed radiological features suggestive of cancer on preoperative imaging (4).
It is therefore important for radiologists to be familiar with its imaging features in order not to miss curable GBCA. In this article, we shall illustrate the various radiological appearances and stages of this disease by the use of case examples, while highlighting the main diagnostic features and potential pitfalls, and by incorporating the recent evidence available in the literature.
Imaging features
Typically, GBCA assumes one of three common configurations: mass-forming, wall thickening, and polypoid. On an unenhanced CT, it is usually hypodense. On MRI, it usually shows hypo- to iso-intense signal on T1-weighted images, and moderately hyper-intense signal on T2-weighted images (5). The tumor classically shows strong contrast enhancement on CT and MRI equal to or greater than that of the liver, which persists into the delayed phases (Figs. 1 and 2) (1, 6).

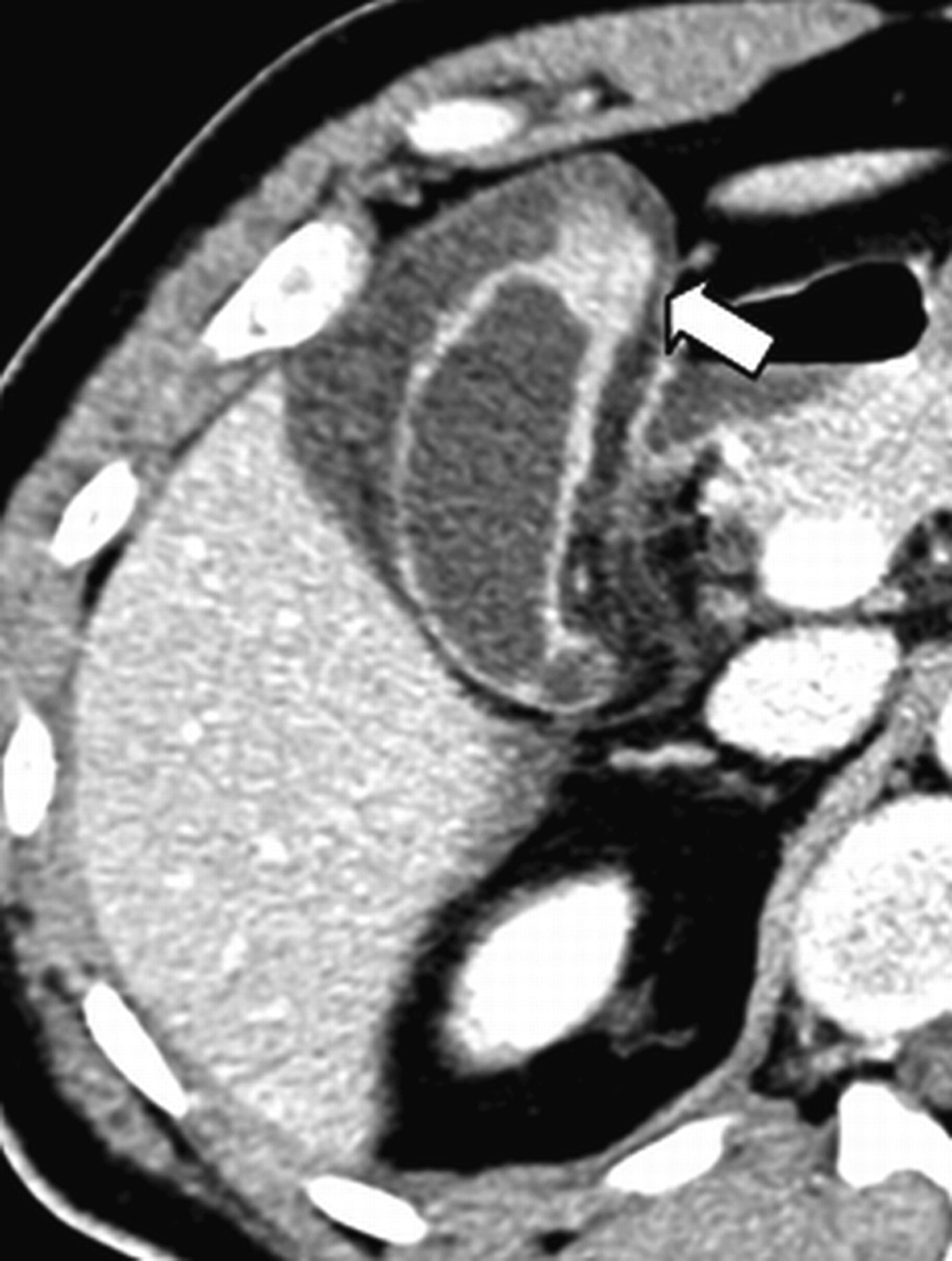
A 55-year-old woman with weight loss and upper abdominal pain. Contrast-enhanced CT (CECT) shows polypoid mass (arrow) within gall bladder lumen. The lesion shows avid contrast enhancement suspicious for malignancy. Note apparent extra-serosal nodules (arrowhead), which represent engorged veins. Postsurgical histology confirmed GBCA

A 70-year-old woman with weight loss. (a) Axial T1-weighted gradient echo (GRE) MR image shows hypointense lobulated mass (arrow) replacing GB and involving adjacent liver (>2 cm). (b, c) Fat-suppressed T1-weighted spoiled GRE image (portal venous and equilibrium phase, respectively) at levels corresponding to (a) show avid and persistent enhancement of solid components of mass (arrows); the pattern is typical for GBCA. Biopsy of the gall bladder confirmed it as a carcinoma
Mass-forming
In 40–65% of patients, GBCA appears mass-like, and either partially or completely fills up the gall bladder (GB) lumen (5). Radiological diagnosis in this subgroup of GBCA is usually straightforward. However, once the tumor invades into an adjacent organ – most commonly the liver – its distinction from other malignancies that have invaded the gall bladder may be difficult. In such cases, the presence of centrally located calculi or curvilinear calcification (from porcelain gall bladder) may provide vital clues to its cholecystic origin (Fig. 3). Those GBCA arising from the body or fundal regions have a propensity to invade the liver (Fig. 2), and those arising from the neck region, the extrahepatic biliary tree. The latter is often confused with extrahepatic cholangiocarcinoma (Fig. 4).
A 64-year-old man investigated for weight loss and abdominal pain. Grey-scale ultrasound demonstrates ill-defined hypoechoic mass surrounding a peripherally calcified gallbladder (arrow). Appearances are suggestive of an aggressive mass arising from a porcelain gall bladder. GBCA was confirmed on histology

A 72-year-old man presenting with obstructive jaundice. (a) Axial CECT shows calcified calculi in the gall bladder and a polypoid mass (open arrow) at the neck region. (b) Axial CECT at a level cranial to (a) shows concentric mural thickening of the common hepatic duct (arrow). Preservation of enhancing mucosa suggests submucosal infiltration. Postsurgical histology showed GBCA with infiltration of common hepatic and bile ducts
Wall thickening
Twenty to thirty percent of GBCA present as focal (Fig. 5) or diffuse wall thickening (Fig. 6) (1). Irregular and asymmetrical thickening is typical for GBCA, but in mild disease, it may be easily overlooked (Figs. 7 and 8). In the early stage of disease, wall thickening is often smooth and indistinguishable from that seen in benign diseases such as cholecystitis and adenomyomatosis (ADM), and systemic diseases such as renal or liver failure. On CT, a single wall layer with avid and heterogeneous portal venous enhancement favours carcinoma (Figs. 7 and 8) (7). In a double-layered wall pattern which is seen in early GBCA, cholecystitis, and systemic disease, an avidly enhancing and thick (>2.6 mm) inner layer with a thin, less enhancing outer layer, are more suggestive of carcinoma (Figs. 9 and 10) (7). During dual-phased (arterial and portal venous phases) CT, the inner layer of a double-layered GBCA typically shows avid enhancement during the arterial phase, which either remains hyperdense or becomes isodense with the surrounding liver during the portovenous phase. In contrast, the inner layer of a double-layered cholecystitis is typically isodense with the surrounding liver on both phases (8). On T2-weighted MRI, diffuse or focal nodular thickening with no layering is typically seen in GBCA (Fig. 6), and a double-layered pattern is seen in inflammatory diseases (9).
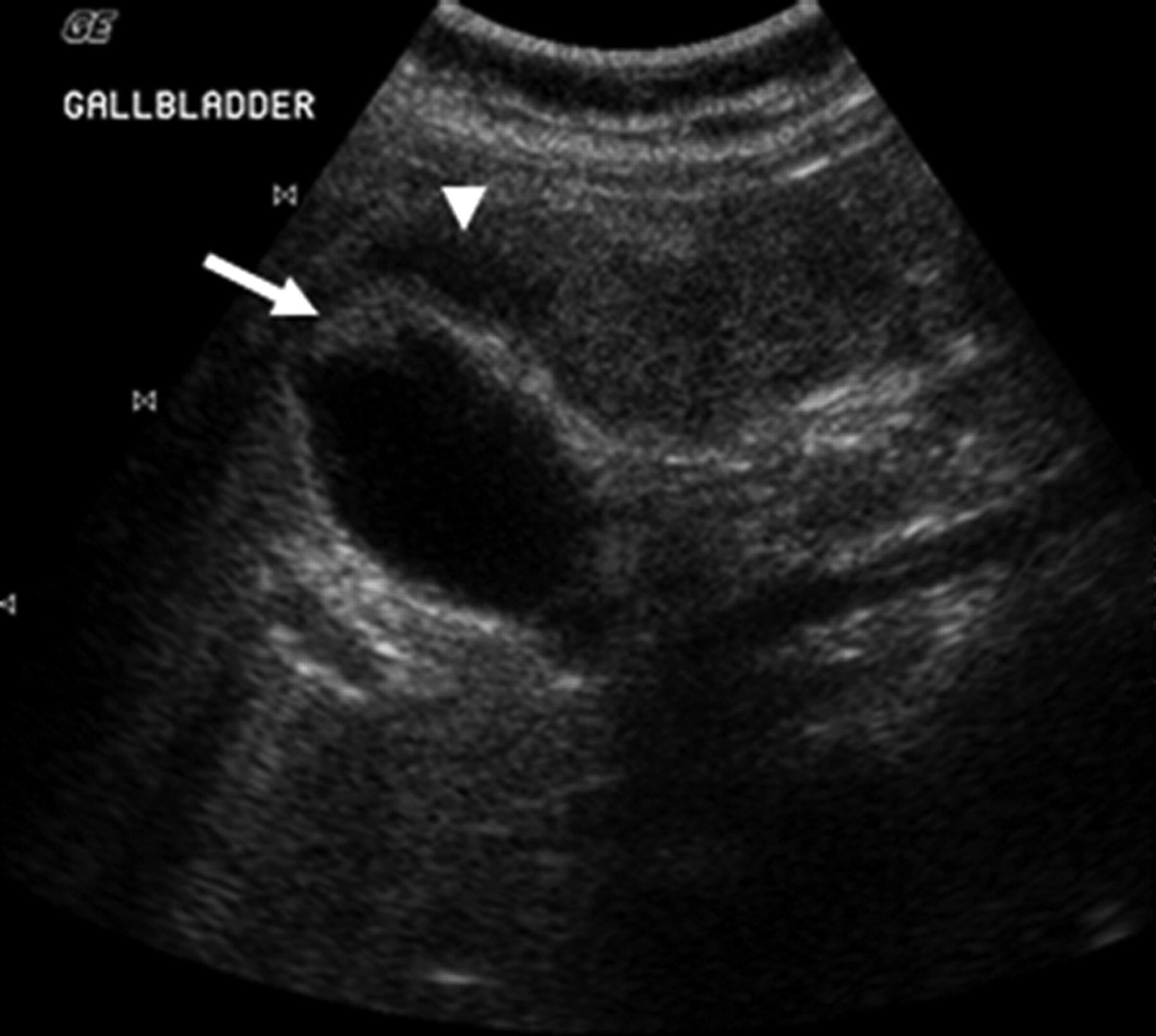
A 63-year-old male patient with epigastric discomfort. Grey-scale ultrasound shows irregular fundal thickening of GB (arrow). Adjacent liver is heterogeneous and shows areas of abnormal hypoechogenicity (arrowhead). GBCA with adjacent hepatic invasion was confirmed on surgery
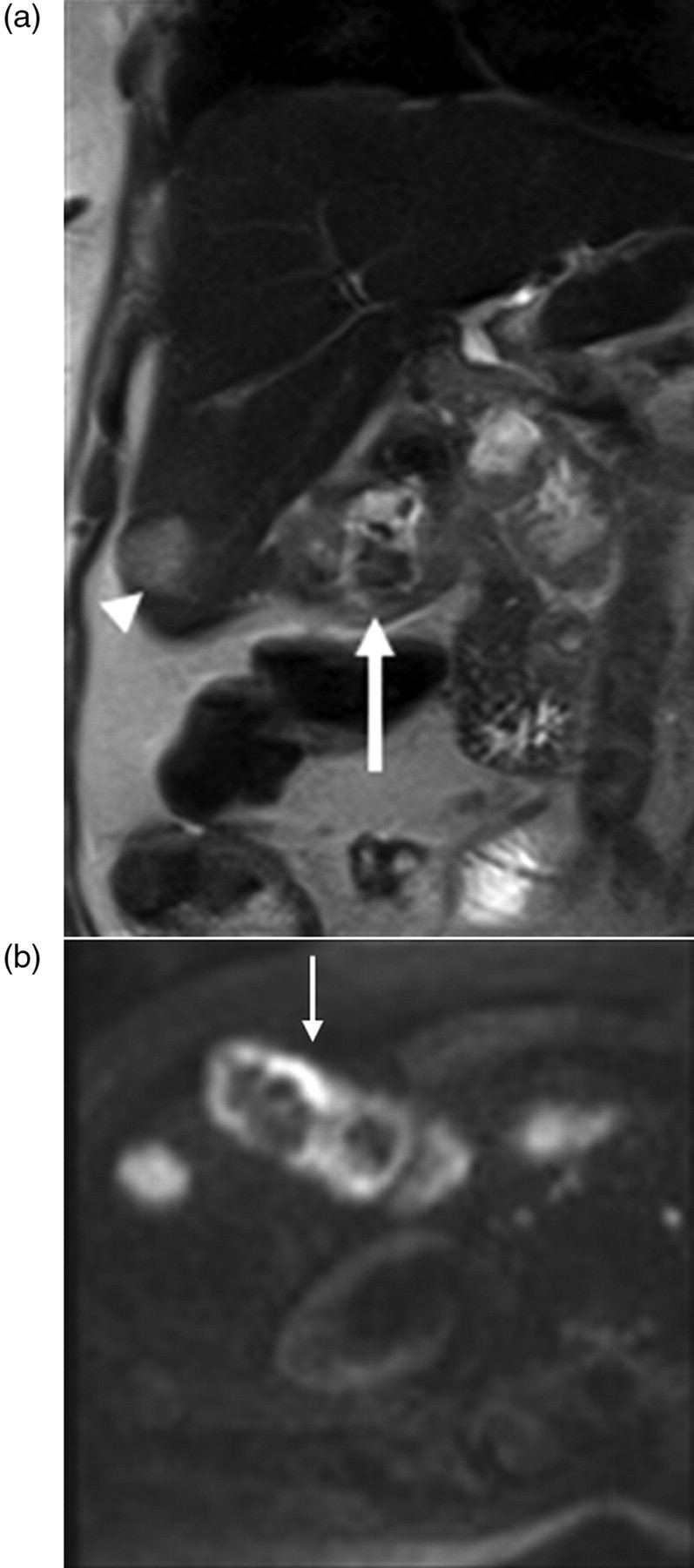
A 64-year-old woman with weight loss and abdominal pain. (a) Coronal single-shot fast-spin echo (SSFSE) image shows irregular gall bladder wall thickening (arrow) with intermediate intensity and no layering. Note T2-hyperintense focus in the liver, consistent with metastasis (arrowhead). (b) Axial high b value (1000) diffusion-weighted image through the gall bladder shows hyperintensity in the thickened wall (arrow), in keeping with malignancy. Biopsy of gall bladder confirmed carcinoma

A 66-year-old woman on follow-up for hepatocellular carcinoma. Axial CECT through the gall bladder shows mild but irregular wall thickening. A calculus is also noted (arrow). This was initially interpreted as inflammatory calculous disease. Histology confirmed GBCA

A 55-year-old man being investigated for cystic lesions in the liver with incidental abnormality in the gall bladder. Axial CECT through the gall bladder shows nodular wall thickening at fundus with avid contrast enhancement (arrow). Mild wall thickening and enhancement are also seen in the adjacent mucosa (arrowheads). Post-cholecystectomy histology confirmed GBCA
A 62-year-old female patient with diffuse thickening of GB wall on ultrasound. Axial CECT shows diffuse double-layered wall thickening. The inner layer shows mild thickening (arrow) and enhancement with a focal nodule at the fundus. Post-cholecystectomy histology confirmed pT1 disease

A 70-year-old woman who presented with right upper quadrant abdominal pain and local peritonism. Axial CECT shows diffuse double-layered gall bladder wall thickening, with hyper-enhancing irregular inner layer (arrow). Abundant pericholecystic free fluid and fat stranding are also present (arrowhead). Post-cholecystectomy histology showed pT1 carcinoma with secondary inflammation
To make radiologists' job even harder, GBCA and cholecystitis can also co-exist due to their common association with gallstone disease (Fig. 7). Furthermore, GBCA that involves the gall bladder neck can lead to outflow obstruction and biliary stasis, becoming a nidus for cholecystitis (Fig. 11).

A 58-year-old man with right upper quadrant pain and pyrexia. Axial CECT axial image shows intramural collection at GB fundus (open arrow) and concentric wall thickening at the neck region (arrowhead). Postsurgical histology showed GBCA at neck region (arrowhead) with secondary inflammation, perforation, and abscess formation at the fundus
Wall thickening secondary to systemic diseases is less confusing due to the presence of associated findings elsewhere (such as ascites and effusion).
The presence of the intramural cystic spaces, due to dilated Rokitansky-Aschoff sinuses, is considered to be a highly specific feature of ADM. Appreciated as a “comet-tail” shadowing on sonography, these spaces are best seen on T2-weighted MR images, where they give rise to the famous “pearl necklace” appearances (10). However, isolated cases of GBCA with similar findings, due to intramural mucin pools, have been reported (11). Moreover, calculi may be formed within these cystic spaces, making the ADM difficult to be distinguished from calculi containing (engulfing) GBCA (Fig. 12). In less certain cases, follow-up to ensure stability is recommended.

A 58-year-old woman investigated for weight loss. Reconstructed sagittal CECT shows a cluster of calculi localised to in the GB fundus (arrow). Preoperative differentials included cholelithiasis and fundal adenomyomatosis with intramural calculi. GBCA engulfing calculi was confirmed by histology on surgical specimen
Xanthogranulomatous cholecystitis (XGC) is frequently associated with irregular wall thickening, visceral invasion and regional adenopathy. The well-described intramural xanthomas and abscesses seen as intramural hypodense lesions on CT favour the diagnosis of XGC, even though there is a significant overlap in appearance with GBCA (12). At present, the preoperative distinction between the two diseases by imaging is not reliable, and surgical excision is recommended.
Polypoid
In the remainder of patients with GBCA, the disease manifests as an intraluminal polypoid lesion (Fig. 1). Benign gall bladder polyps are common incidental lesions on sonography, and they are mostly cholesterol pseudopolyps. Cholesterol pseudopolyps are typically pedunculated in configuration, multiple, and less than 1 cm in diameter. On ultrasound, they are typically echogenic without posterior acoustic shadowing. The larger lesions are seen as aggregates of echogenic specks (13). On unenhanced CT, they are often invisible or appear smaller than on ultrasound or contrast-enhanced images. With contrast, they show avid contrast enhancement. Malignant polyps are typically sessile in configuration, solitary, and more than 1 cm in diameter (Fig. 13). On CT, they are typically visible without intravenous contrast, and show avid and prolonged contrast enhancement (Fig. 1) (14, 15). The other independent predictors of malignancy are the patient's age (>57 years) and the presence of gall bladder calculi (16, 17). Preoperative distinction between the two entities is unreliable, and lesions more than 1 cm – particularly those with broad base and sessile configuration – should be surgically removed (18). Those between 5 and 10 mm should be regularly followed up for progression in size; only a small percentage of benign polyps demonstrate increases in size over time (19). Tumefactive sludge should be recognized from its mobility and avascularity on sonography.

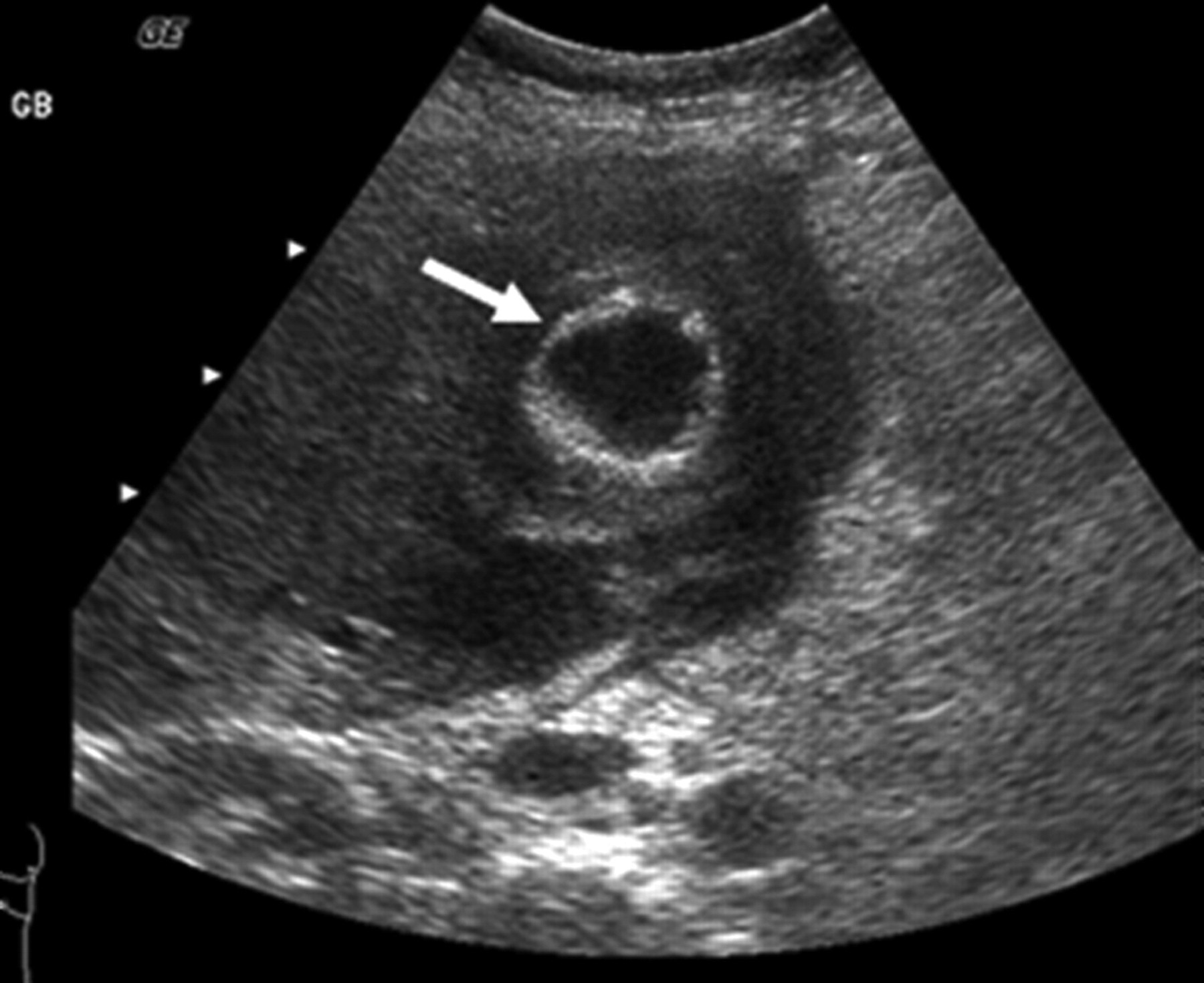
A 65-year-old man with epigastric discomfort. (a) Grey-scale ultrasound image of the gall bladder showed 1.4 cm solitary sessile polyp (arrow) of intermediate echogenicity. These features collectively were highly suggestive of malignancy. Surgery was advised. Patient was lost to follow-up. (b) Patient re-presented for follow-up 2 years later. The grey-scale ultrasound image of gall bladder now showed mass filling up the lumen (arrow). GBCA was confirmed on surgical specimen
Contrast-enhanced ultrasound (CEUS) and diffusion-weighted MR (DW-MR) are two relatively new imaging techniques that have been extensively studied for their roles in investigating abdominal malignancies. Their roles, specifically in distinguishing benign from malignant gall bladder disease, have also been studied. On CEUS, Xie et al. reported that both benign and malignant polyps show early contrast hyper-enhancement, as both receive pure arterial supply (20). However, a tortuous (as opposed to a normal dotted) vessel enhancing pattern, delayed contrast washout that is manifested as hypoechogenicity at 30–60 s, and interruption of mucosal integrity, are typical features seen in GBCA, whereas benign lesions typically showed delayed contrast retention and mucosal integrity (20). Sugita et al. and Irie et al. reported that GBCA typically appeared hyper-intense on high b value DW images more often than benign gall bladder lesions. GBCA also showed significantly lower apparent diffusion coefficient (ADC) values compared with benign gall bladder lesions (Fig. 6b) (21, 22).
Assessment of spread
After the diagnosis is made, accurate evaluation of the local and distant extent of GBCA is pivotal in prognostication and therapeutic planning. The operability of the tumor and the surgical approach is determined by the extent of the primary tumor, and the prognosis of gall bladder cancer differs according to the TNM staging (19–21). Moreover, accurate assessment of the segmental anatomy and generation of an accurate vascular map of the relevant arterial and venous anatomy are both crucial prerequisites to planning radical surgery. An accuracy of about 85% was reported in the staging of GBCA by multidetector row computed tomography (MDCT) (23, 24).
According to the sixth edition of American Joint Committee on Cancer staging manual (25), GBCA can be classified as:
T1: Confined to the lamina propria or the muscle layer of the gall bladder (T1A and T1B, respectively); T2: Extending to, but not through, the serosa; the preservation of the pericholecystic fat plane denotes T1 or T2 disease. The radiological distinction between T1 and T2 disease carries poor accuracy (23); T3: Perforating the serosa or directly invading the liver of less than 2 cm margin, and/or one other adjacent structure (stomach, duodenum, colon, pancreas, omentum, or extrahepatic bile ducts) (Figs. 5 and 14). Radiologically, this is manifested as the loss of an intervening fat plane between the tumor and an adjacent organ, and presence of serosal nodules. The loss of an intervening fat plane leads to false-positives due to partial-volume averaging and pericholecystic adhesion, and the serosal nodules may be mimicked by engorged cholecystic venous branches due to tumoral neovascularity (Fig 1) (23). High resolution studies with multiplanar reconstruction are key to avoiding these pitfalls. Intrahepatic extension may sometimes be mimicked by peritumoral hyperaemia in adjacent liver parenchyma. If in doubt, an MRI evaluation should be carried out, as reactive hyperaemia is not visible on unenhanced images with no restricted diffusion on DWI; T4: Invading the liver of more than 2 cm (Figs. 2 and 3), main portal vein, the hepatic artery, or multiple extrahepatic organs. Vascular involvement is radiologically determined by the irregularity of the vessel wall adjacent to the tumor, and the presence of tumor on both sides of the vessel on at least one plane (26). T4 disease is not amenable to curative surgery.
A 70-year-old diabetic woman presented with pyrexia and right upper quadrant abdominal pain. Axial CECT shows extensive gall bladder wall thickening with intraluminal gas. The intervening fat plane with liver (open arrow) and duodenum (arrowhead) are lost. The liver and duodenal biopsy confirmed GBCA. Cholecystoduodenal fistula was noted on endoscopy

Nodal involvement is present in more than 50% of patients at initial diagnosis. Regional stations, considered N1, constitute cystic, pericholedochal, hilar, periduodenal, peripancreatic, and superior mesenteric nodes. Extraregional stations are those centered around the para-aortic region, and considered as M1 disease. As with other malignancies, nodal involvement is radiologically determined based on the size criteria of 1 cm in the widest short-axis diameter. Regional adenopathy does not preclude curative surgery.
The direct venous drainage of the gall bladder into the liver means distant metastases are common in the liver, and, thereafter, lungs. Peritoneal deposits are likely due to direct spread. Metastatic disease precludes curative surgery.
The other criteria for non-resectability include: involvement of main portal vein or hepatic artery; involvement of the portal vein or hepatic artery branches of both lobes of the liver; simultaneous involvement of the ipsilateral hepatic artery and contralateral portal vein; simultaneous invasion in both lobes of the liver at the level of confluence of segmental bile ducts to form the hepatic ducts; contiguous involvement of more than two segments each in both lobes of the liver (27). By using the multislice CT dual-phased technique with 3D reconstruction, Kalra et al. reported an accuracy of 85% for determining the resectability of GBCA (26).
As for any hepatic surgery, anatomical variants in hepatic artery (e.g. replaced right hepatic artery), portal vein (e.g. trifurcation), and hepatic veins (accessory veins) should also be conveyed to the surgeon by generating a high resolution vascular map.
Conclusion
While its diagnosis at the advanced stage is relatively straightforward but less rewarding, diagnosis of early GBCA is potentially life-saving but riddled with non-specific imaging features. We hope to have highlighted the main imaging features and potential pitfalls in the diagnosis and staging of this deadly disease. Suspicious findings should at least lead to a diagnosis of “potential GBCA” in the report, which should prompt intraoperative histological confirmation to ensure adequate surgery and potential cure.
Footnotes
ACKNOWLEDGEMENTS
The authors would like to acknowledge Ms Shuyu Tan from the Publications Support Unit, Yong Loo Lin School of Medicine, National University of Singapore.