
Abstract
We report a case of a 63-year-old man with a complicated postsurgical bronchopleural fistula (BPF), which was treated with a minimally-invasive hybrid procedure using fluoroscopy, bronchoscopy, and thoracoscopy. A previous surgical attempt had failed to seal the pathologic tract. An Amplazter II vascular plug was successfully deployed into the BPF, followed by autologous blood and glue injection. An adjunctive endoscopically-guided glue embolization was deemed necessary. The 14-month clinical and imaging follow-up confirmed the successful exclusion of the BPF. No migration of the device was noted and the patient remained asymptomatic. The combined endoscopic and fluoroscopic guided management of a BPF using the Amplatzer II vascular plug and glue was proven safe and effective after mid-term follow-up.
Bronchopleural fistulas (BPFs) constitute a serious complication of pneumonectomy, and are associated with high perioperative morbidity and mortality rates (1). Due to the direct communication with the pleural space, the fistula may be further complicated leading to an empyema, aspiration pneumonia, adult respiratory distress syndrome, and even death (2). Despite advanced surgical techniques that are currently employed to minimize postoperative BPFs, an incidence rate between 3% and 28% is reported (3–5). BPF treatment may require a new surgical intervention with high periprocedural mortality and morbidity rate. The mortality rate associated with BPFs ranges from 16% to 72% (4, 5). We herein report the first mid-term outcomes following the minimally-invasive, hybrid management of a complicated postoperative BPF, using an Amplatzer II vascular plug, and glue embolization under bronchoscopic, thoracoscopic, and fluoroscopic guidance.
Case report
A 63-year-old male ex-smoker was referred from his general practitioner to our tertiary level hospital due to persisting cough. A computed tomography (CT) scan revealed a 3-cm lesion in the left upper lobe of the lung with imaging characteristics of malignancy. The lesion appeared with a high fludeoxyglucose (FDG) uptake on positron emission tomography (PET)-CT scan (GE Discovery ST PET-CT scanners, GE Healthcare, Waukesha, WI, USA). Percutaneous biopsy followed and the histology confirmed a bronchogenic non-small-cell lung carcinoma (NSCLC) that was staged as T1bN1M0. The patient was considered fit for surgery and a left-sided total pneumonectomy was performed. The procedure was uneventful, but on the first evening post surgery the patient had to be returned to the operating theater for a re-exploration and bleeding control. However, the patient had a rapid recovery without any further complications and was dismissed after 6 days. A week later the patient developed clinical symptoms of postoperative infection (pain, raised white blood cells, difficulty breathing) with purulent discharge. Air was emerging from the surgical wound on coughing. Chest X-ray revealed a large left hemithorax collection with multiple air fluid levels. The diagnosis was early bronchial breakdown complicated by infection of the pneumonectomy space. Left video-assisted thoracoscopic surgery (VATS) was performed the following day. The pleural flap was raised, the bronchial stump edges were trimmed, and surgical adhesive glue was applied in order to obtain sealing of the fistula, while in order to treat the empyema thoracic wash-out was performed and a thoracic window was created anterior to the thoracotomy. Nevertheless, the fistula persisted and was evident by CT (Fig. 1), while the patient suffered from dyspnea and dysphonia over the next few weeks. A multidisciplinary meeting decision was made to attempt treating the fistula using fluoroscopically-guided, transbronchial embolization of the communication site. The procedure was performed under general anesthesia in the operating theater. A mobile digital fluoroscopic C-arm was used for fluoroscopic guidance. A thoracic surgeon and two interventional radiologists were involved in the procedure. The access to the bronchial tree was obtained with the use of a rigid bronchoscope that was initially advanced into the left main bronchus, followed by a thoracoscope, which was positioned via the left chest wall defect and was used to view the pleural aspect of the fistula. A fixed core, polytetrafluoroethylene (PTFE) coated, 150 cm, 0.035”, 10 cm floppy guide-wire (Bentson Straight, COOK, Bloomington, IN, USA) and two 4Fr Multipurpose catheters (Abbott Vascular, Abbott Park, IL, USA) were subsequently advanced in a parallel fashion through the fistula into the pleural space. One of the two catheters was exchanged to a 45 cm 7Fr sheath (COOK, Bloomington, IN, USA) through which the vascular plug was to be advanced whereas the other 4Fr catheter was left in the pleural space in order to maintain access for the subsequent glue injection (Fig. 2). The guide-wire was retracted from the 8Fr sheath and an 18 × 22 mm vascular occlusion device (Amplatzer vascular plug II, AGA Medical Corporation, Plymouth, MN, USA) was advanced through the sheath across the fistula under both fluoroscopic and bronchoscopic monitoring. The sheath was retracted and the device was deployed with the lateral disc orientated against the pleura just beyond the pneumonectomy stump, and the medial disc in the proximal left main bronchus (Fig. 2). Once the patency of the right main bronchus was secured, the 4F catheter was used to inject 3 mL of surgical glue, composed by purified bovine serum albumin (BSA) and glutaraldehyde (BioGlue® Surgical Adhesive, San Mateo, CA, USA) in order to obtain complete sealing of the fistulous tract (Fig. 2). Few mL of additional autologous blood clot were also used to block the proximal part of the plug. No immediate adverse events were noted. However, 3 days after the procedure clinical examination revealed a small amount of air leak on cough. Subsequently left VATS was performed and in total 10 mL of BioGlue were additionally applied into the fistula. This procedure was not performed under fluoroscopic guidance. CT scan before discharge confirmed the correct position of the vascular plug into the stump of the left main bronchus and the satisfactory expansion of the right lung. No inflammatory pleural collections were noted (Fig. 3). The patient was discharged 2 days later, free of symptoms.
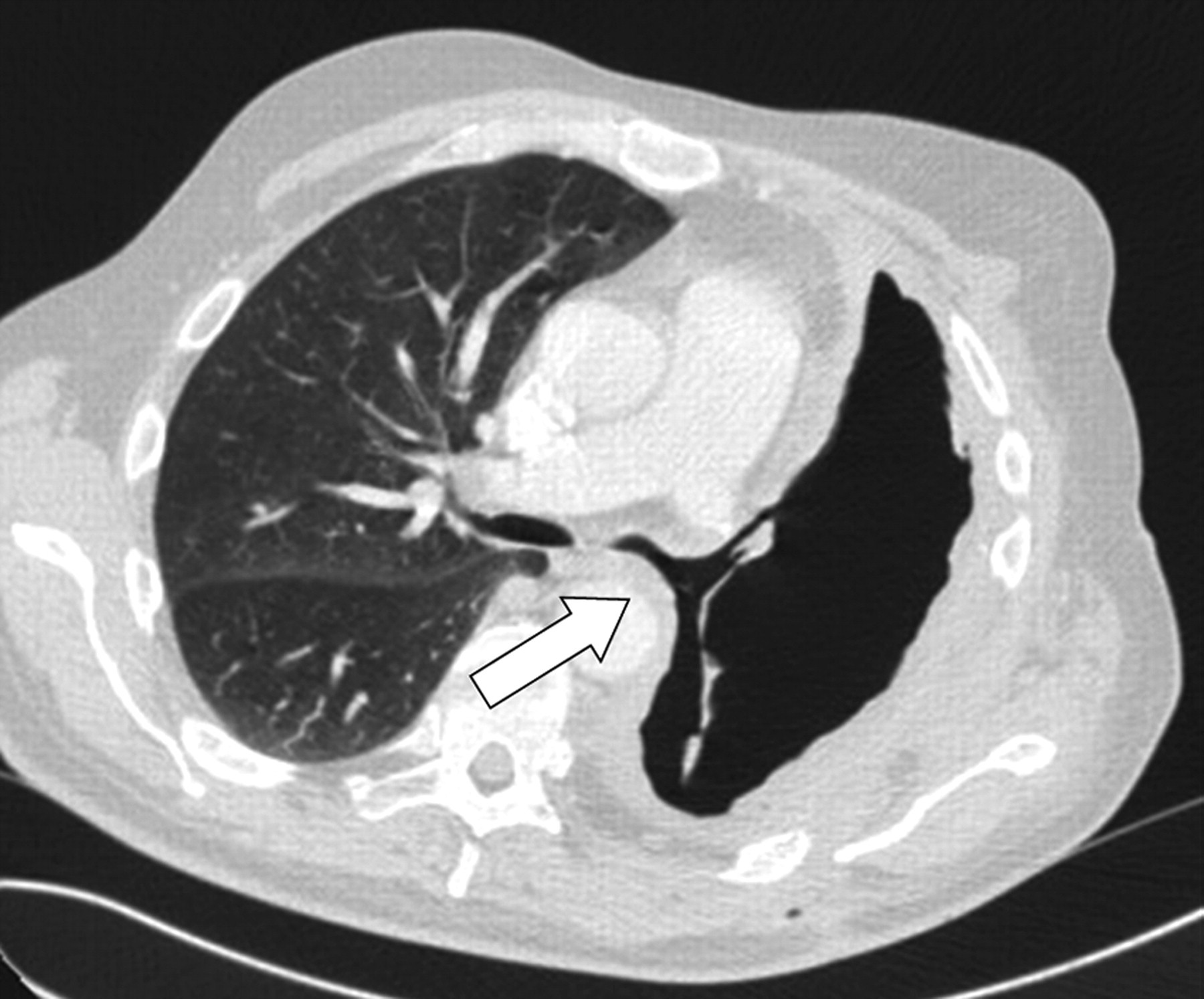
CT scan demonstrating the left bronchopleural fistula (arrow)

Fluoroscopic images demonstrating a 7Fr sheath advanced into the fistula through which the vascular plug is about to be deployed, while the 4Fr catheter (arrow) is situated in the pleural space (a) and the deployed device (b, c). The 4Fr catheter is retracted (arrow) as to allow the glue injection in the proximal end of the device. Note that the distal disc is orientated against the mediastinal pleura, and the medial disc towards the proximal left main bronchus

Postprocedural, pre-discharge chest CT confirming the appropriate positioning of the vascular plug within the left main bronchus. Note that the device completely traverses the stump of the left main bronchus with its proximal end sitting against the tracheal wall at the origin of the left main bronchus and the distal end adjacent to the pneumonectomy cavity (arrow). The right bronchus remains patent
After a 14-month clinical and imaging follow-up (regular clinical examination and chest X-rays every 3 months), the patient was in good condition, with satisfactory breathing capacity and no signs of ongoing infection. The thoracic window had diminished to 2 cm and was producing only a small amount of clear fluids. Although there was still a small amount of residual air in the left hemi thorax, visible at plain chest X-ray, the fistula was not evident during auscultation and the patient remained asymptomatic.
Discussion
A bronchopleural fistula is a pathologic condition characterized by the direct communication of the pleural space and the bronchial tree. It is usually iatrogenic (i.e. postsurgical) and is associated with increased morbidity and mortality (2). The incidence of BPFs after pneumonectomy varies and is appears to be more frequent when resection occurs in the ambit of an underlying malignancy or after right total pneumonectomy (6). Potential treatment options mainly include surgical and bronchoscopic techniques. Surgery is usually indicated for the large BPFs but usually results in disappointedly high peri-procedural morbidity and mortality rates, whereas bronchoscopy may offer a less invasive solution with the use of sealing materials (i.e. glue, coils, and/or stents) but is associated with higher recurrence rates (7–12).
We report a case of a left-side large postsurgical BPF complicated by infection and treated with a minimally-invasive hybrid procedure. An initial VATS attempt to treat the fistula was unsuccessful, and the lesion was finally sealed with a large diameter endovascular closure device and glue application, under bronchoscopic, fluoroscopic, and thoracoscopic guidance, followed by a second consecutive glue embolization under endoscopic guidance. The specific embolic device was chosen because of its large diameter, particular design, and deploying mechanism which allows a very precise positioning at the site of the pathologic communication. The Amplatzer vascular plug II provides the choice to deploy, recapture, and redeploy ensuring accurate placement. The extravascular use of this specific device has been reported to be safe and feasible (10, 11). A bare nitinol plug was chosen because its dimensions were more suitable for the large fistula length. A very similar covered device, the Amplatzer Atrial Septal Occluder with a polyester fabric inside the metallic mesh, has been previously utilized but only in shorter lesions (11). Moreover, the uncovered device has the benefit of immediate endothelial response and quick integration to the surrounding tissue, which usually reduces migration rates, particularly in non-vascular applications. On the other hand the covered device offers better sealing of the fistula. We decided to inject glue in order to obtain a better sealing effect and autologous blood injection was used proximally in order to avoid glue contamination of the remaining lung. Furthermore, blood accelerates the polymerization of the surgical glue. The use of the Amplatzer device for the management of a BPF has been also described by Fruchter et al. in a recent publication including 10 patients, three of which underwent a previous unsuccessful surgical treatment attempt (11). However, the authors used only bronchoscopic guidance for the deployment of the device and median follow-up period was nine months, while the successful exclusion of the fistula was obtained in all but one patient (90%). The sole failure was attributed to the large size of the BPF and therefore a subsequent surgical treatment was endeavored. The type of the device used (covered or uncovered) in this study was not stated. In this particular case where the length of the tract necessitated the use of an uncovered device, the adjunctive application of BioGlue was proven effective. The dual material technique was also described by Gulkarov et al. (10) but both positioning of the covered Amplatzer plug and the glue injection were performed solely under bronchoscopic guidance. Moreover, the procedure was used as a bridge to surgery and the follow-up was limited to one month.
Whereas in the above-mentioned publications only bronchoscopy was employed and follow-up was available up to 9 months, in the herein reported hybrid procedure bronchoscopy was used to gain access to the left main bronchus, while fluoroscopy was the main imaging guidance modality during device deployment and 14-month clinical and imaging follow-up is presented. The authors believe that the specific radiopaque device is better visualized under fluoroscopic guidance and that fluoroscopy was essential for the real-time monitoring of the precise and uncomplicated plug deployment.
In conclusion, the occlusion of a complicated post-surgical BPF with the Amplatzer vascular plug II and glue in a minimally-invasive, hybrid procedure setting, using bronchoscopy, thoracoscopy, and fluoroscopy was proven to be safe and feasible in this patient. The 14-month clinical and imaging follow-up supports the mid-term efficacy of the method.