
Abstract
Background
Idiopathic intracranial hypertension (IIH) is a clinical disorder of unknown etiology manifesting with increased intracranial pressure in the absence of hydrocephalus, an underlying mass lesion, and demonstrating normal cerebrospinal fluid composition. IIH may exhibit several non-specific imaging findings including: an empty sella, posterior globe flattening, tortuosity of the optic nerve, and optic nerve sheath distention.
Purpose
To introduce widening of the foramen ovale as a new imaging marker for IIH.
Material and Methods
IIH is a syndrome which may exhibit several previously described non-specific imaging findings including: an empty sella, posterior globe flattening, tortuosity of the optic nerve, and optic nerve sheath distention. We hypothesize that chronically elevated cerebrospinal fluid pressure can lead to osseous erosions and we propose widening of the foramen ovale as a new imaging marker for IIH.
Results
Average foramen ovale sizes were increased in patients with IIH compared to controls (30.03 ± 7.00 mm2 vs. 24.21 ± 5.97 mm2, P < 0.001). For a cut-off value of 30 mm2, the sensitivity of FO area to detect IIH was 50%, with 81% specificity. Classic findings were significantly more common in patients with IIH compared to controls including: empty sella (65.9% vs. 0%), posterior globe flattening (65.9% vs. 4.5%), vertical tortuosity of the optic nerve (54.5% vs. 9.1%), and optic nerve sheath distention (52.3% vs. 11.4%, all P values < 0.001).
Conclusion
Our study confirms the association of several classic imaging findings with IIH and supports widening of the foramen ovale as an additional imaging marker which may be incorporated into the evaluation of patients suspected to have this condition.
Idiopathic intracranial hypertension (IIH), previously referred to as pseudotumor cerebri or benign intracranial hypertension, is a syndrome of unknown etiology best described as increased intracranial pressure (ICP) in the absence of an identifiable cause (1, 2). It predominantly affects overweight women of childbearing age (3, 4). Patients usually present with headaches, nausea, vomiting, visual field disturbances, tinnitus, and physical examinations frequently and classically reveal papilledema (2, 3). Proposed mechanisms of pathogenesis for IIH revolve around altered cerebrospinal fluid (CSF) physiology, either through resistance to absorption and/or abnormal CSF pressure and pulsatility (5–9). Recently, vascular causes have also been proposed to contribute to the underlying pathology, with emphasis on arterial inflow and venous outflow abnormalities (10–13).
Traditionally, the role of imaging in the evaluation of IIH has been to exclude secondary causes of increased ICP and papilledema (1, 2) including but not limited to: hydrocephalus, intracranial masses, chronic meningitis and dural venous sinus thrombosis. Several radiological findings have been described in the literature that may aid in establishing the diagnosis such as: flattening of the posterior aspect of the globe; increased perioptic nerve sheath dimensions; vertically increased tortuosity of the optic nerve (ON); and the presence of an empty sella, described as an enlarged, CSF-filled sella with or without the presence of an identifiable pituitary gland (14–22). Previous reports suggest that most of these findings aid in the diagnosis of IIH but lack sufficient specificity.
The relationship of an empty sella with IIH is not fully understood and its pathogenesis is still debated; however, it is thought that the exertion of chronically elevated CSF pressure or pulsatility on the diaphragma sellae causes this finding (23). CSF herniates into the sella through an opening in the diaphragma sellae and over time causes widening and enlargement of the sella turcica and effacement of the pituitary gland leading to the typical appearance of an empty sella. Our hypothesis is that IIH causes osseous erosions by a similar mechanism, eventually leading to CSF leak as a consequence of osseous dehiscences and arachnoid herniation. Osseous dehiscences in the skull base occur mainly in the cribriform plate, the sphenoid sinus, and the tegmen tympani, among other locations. In clinical practice we have also noted a tendency for the foramen ovale (FO) to appear widened in patients with IIH. Meckel's cave is a dura/arachnoid-lined extension of the prepontine cistern which contains the fifth cranial nerve ganglion. The mandibular nerve (V3) passes through the FO in the middle cranial fossa, at the skull base, before the other trigeminal nerve branches (V1 and V2) enter the cavernous sinus. Arachnoid spaces that herniate towards the sella secondary to chronically increased ICP may also herniate through the FO, leading to widening over time. We think that FO widening may be detected by imaging before other osseous erosions and CSF leaks become apparent. This finding has not been reported and is unique in that it could serve as an objective evaluation method that could potentially be used in clinical practice.
The objectives of this study were: (a) to investigate the relationship of IIH with FO widening, osseous erosions and low lying tonsils demonstrated by CT and MRI; and (b) to analyze the frequency of traditionally reported radiological manifestations of IIH (i.e. empty sella, ON sheath distention, ON vertical tortuosity, posterior globe flattening, and slit-like ventricles) in our patient population.
Material and Methods
Study subjects
An institutional review board (IRB) approved retrospective study of 48 patients with clinically confirmed IIH was conducted. All the patients with IIH who were seen in our neurology clinic between January of 2005 to April of 2010, and who had both MRI and CT studies of the head were selected and their past medical histories were reviewed in detail. The provided reason for the exams was headache. The diagnosis of IIH was established by the Modified Dandy Criteria, which takes into account a combination of clinical signs, and CSF studies revealing normal composition and pressure greater than 250 mm H2O on lumbar puncture (2). Patients with a history of trauma, congenital cranial malformation, subarachnoid hemorrhage and intracranial surgery unrelated to IIH, as well as patients who were found to have secondary causes of increased ICP on imaging, such as hydrocephalus, intracranial mass, cerebral venous thrombosisor chronic meningitis, were excluded. Diseases such as Addison's disease, hypoparathyroidsm, pulmonary hypertension, renal failure and medications such as vitamin A, tetracycline, lithium, and anabolic steroids are known to cause elevations in ICP. Patients' past medical histories were screened to confirm the absence of these factors.
The patient group who had MRI scans included 47 female patients and one male patient. Four of the patients only had a CT scan without a corresponding MRI scan. A matched control group of 44 patients by age and sex for the patient group with MRI scans, and a control group of 48 patients for the patient group with CT scans was selected from the PACS station. The control group consisted of patients with completely normal imaging findings. The symptoms prompting the study in the control group were either headaches, dizziness, or weakness. Those who had headaches were either due to migraines or were of an acute nature. None had papilledema on exam. Upon detailed review of the medical records of the control group, there were no clinical findings to suggest the possibility of IIH.
Image analysis
The CT and MRI images of the patients were analyzed by two neuroradiologists in a blinded fashion. In case of multiple studies, the most recent study was used for evaluation. All CT and MR studies of the head were performed within 1 year of one another. Four of the 48 patients included in the CT scan group did not have MRI scans. Measurements of the FO were taken from CT images. All cases were de-identified and the reviewers were asked to note the presence or absence of classically reported imaging findings of IIH on MRI and presence of bony erosion on CT exams. A final decision regarding the findings was reached by common consensus.
CT images on eight out of 48 of our patients were obtained on a 2-slice CT scanner (Siemens Volume Access, Siemens Medical Solutions; Erlangen, Germany), all performed before the year of 2007 and CT images on the rest of the patients were obtained on a 64 MDCT scanner (Siemens Somatom Sensation, Siemens Medical Solutions; Erlangen, Germany) and analyzed for the presence of and location of osseous erosions. Area measurements of both FO were obtained on an axial plane through the supraorbitomeatal line (section thickness = 3mm, field of view = 230mm, matrix = 512 × 512, bone window). Measurements were performed with a hand-drawn circle, using a PACS workstation (Cerner Works 2006, Cerner Corporation; Kansas City, MO, USA). The most cephalad slice showing the FO was chosen. An average of left and right FO measurements was obtained.
Repeatability and reproducibility analyses were conducted and analyzed separately with repeat of FO measurements at a later time. The FO measurements from the patient group were repeated 3 weeks later by the same observer (SB) for repeatability analysis. The average of the left and right FO area was used for each patient. The measurements were also obtained by a different observer (DT) for inter-rater reproducibility analysis.
MR images were obtained on either a 1.5 Tesla (Siemens Sonata, Siemens Medical Solutions; Erlangen, Germany) or a 3.0 Tesla (Siemens Magnetom Trio, Siemens Medical Solutions; Erlangen, Germany) scanner using a standard head coil and examined for low-lying cerebellar tonsils, the presence or absence of a partially or completely empty sella, vertical ON tortuosity, ON sheath distention, and posterior globe flattening. Arachnoid space herniations were also evaluated, defined as extensions of arachnoid spaces beyond the expected margin of dural reflections predominantly occurring at the skull base. Vertical ON tortuosity was evaluated on the sagittal plane. Cerebellar tonsils were considered low-lying if they abutted the foramen magnum or extended below it by no more than 5 mm. Partially empty sella was considered present when the majority of the sella turcica was filled with CSF with the presence of a thinned pituitary gland at the base of the sella. A completely empty sella was diagnosed if the pituitary fossa was completely filled by CSF with no visible pituitary gland. All subjects were scanned using standard protocol for headaches with a section thickness 4.0 mm and a gap of 30%, including axial T1, T2 fat-saturated, axial FLAIR, diffusion-weighted, and sagittal T1 sequences.
Statistical analysis
Categorical variables were compared using the chi-square test and continuous variables (i.e. FO measurements) were compared using the Student-t test (SPSS software 2007; Chicago, IL, USA). Accuracy of FO size to diagnose IIH was evaluated by ROC curve (GraphPad Prism 5, GraphPad Software; La Jolla, CA, USA). Agreements of average FO area measurements were analyzed with Bland-Altman plots using absolute differences between the measurements (XLSTAT for Mac; Addinsoft, Montreal, Canada).
Results
CT findings
Foramen ovale area measurements were significantly larger in the patients (30.03 ± 7 mm2) with IIH compared to the control group (24.21 ± 5.97 mm2) with a P value of <0.001 (Fig. 1, Table 1). When the ROC curve was plotted for FO measurements for the detection of IIH, an area under the curve of 0.74 was found (95% CI 0.65–0.84). For an arbitrary cut-off of 29.9 mm2, the sensitivity of FO area to detect IIH was 50% with 81% specificity (Table 2, Fig. 2).

Axial (a) non-contrast CT image shows bilaterally widened FO in a patient with IIH with an area of 47.7mm2, and axial (b) image shows FO in a normal patient with an area of 26 mm2, for comparison

FO areas plotted on a ROC curve. Area under the curve: 0.74 (95% CI 0.65–0.84)
Foramen ovale (FO) area measurements of the patients (n = 48) and the control group (n = 48) with statistical comparisons
All measurements are mean ± SD
Sample FO area measurements with corresponding sensitivity, specificity, and positive predictive values to detect IIH
The FO average measurements were repeatable and reproducible with good agreement for both intra-observer and inter-observer measurements. The repeated measurements by the same rater had a mean FO area of 28.55 mm2 and a standard deviation (SD) of 7.1 for the first set of measurements. A mean of 28.89 mm2 and a SD of ±7.16 were calculated for the second set of measurements. Intra-rater analysis demonstrated a bias of –1.026 mm2 (95% CI –1.661 to –0.391 mm2). Most measurements fell within 95% limits of agreement for average measurements plotted against the difference between measurements. The 95% CI for difference between measurements ranged from –5.313 to 3.261 mm2. The second rater had a mean of 28.55 mm2 and a SD of ± 7.1. Inter-rater analysis demonstrated a bias of 0.679 mm2 (95% CI 0.024–1.335 mm2) and a 95% CI for the difference in absolute measurements ranging from –6.699 to 6.428 mm2. Bland-Altman plots for intra-rater and inter-rater absolute differences of the measurements are provided in Figs. 3 and 4.

Intra-rater agreement analysis demonstrated in Bland-Altman plots for absolute differences of the measurements between the two measurements
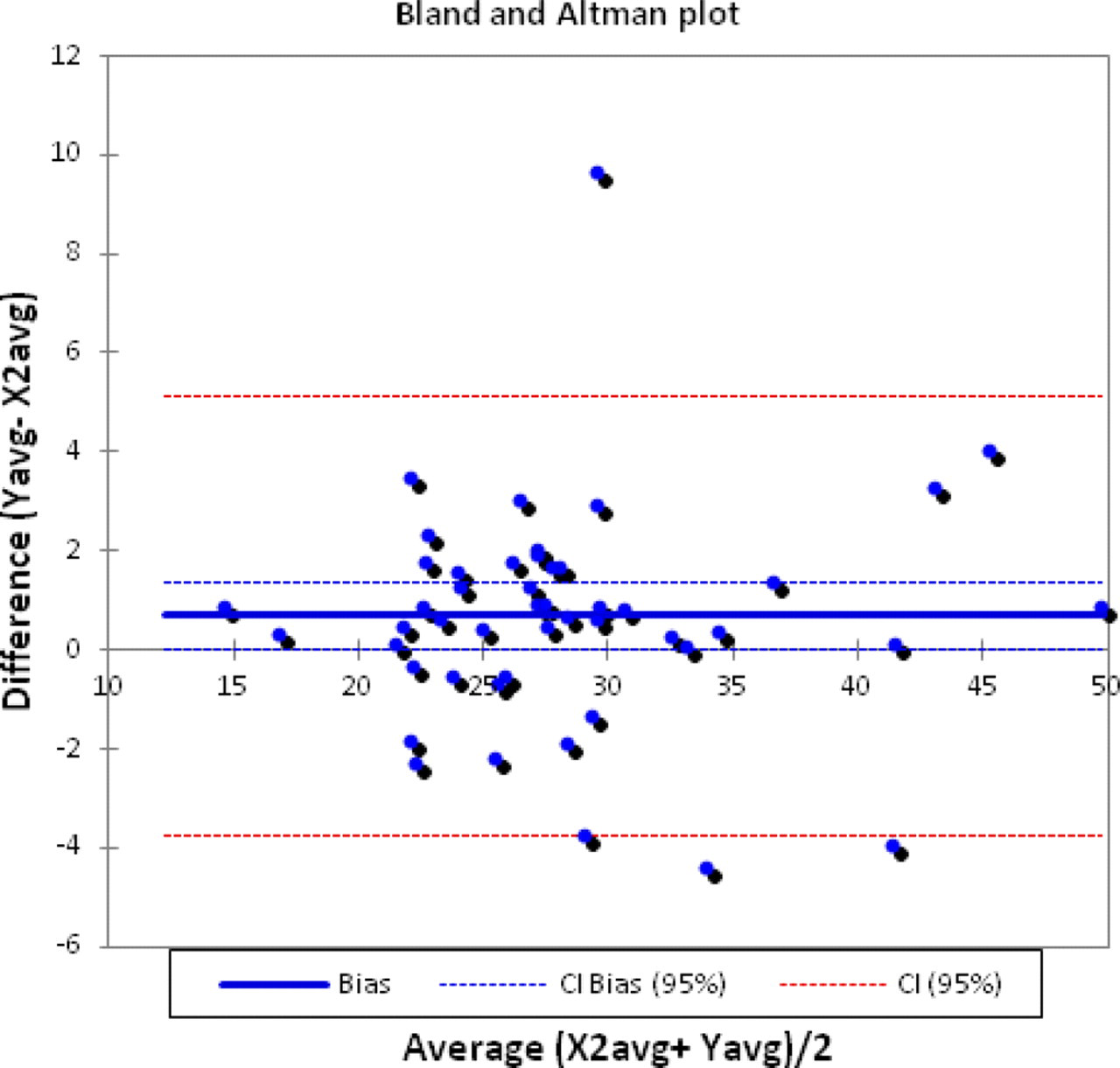
Inter-rater agreement analysis demonstrated in Bland-Altman plots for absolute differences of the measurements between the two raters
Two of our patients demonstrated arachnoid space herniation through osseous defects or, in other words, osteodural defects, secondary to osseous erosion progression. One patient had herniation through the greater wing of the sphenoid bone as well as an empty sella, ON sheath distention, and posterior globe flattening (Fig. 5). This patient had an average FO measurement of 46 mm2. The other patient had arachnoid space herniation through the petrous apex, extending from bilaterally prominent Meckel's caves. The extra-axial space anterior to the middle cranial fossa was also prominent. This patient also had a constellation of findings, including an empty sella, ON sheath widening, and FO widening (Fig. 6). The average FO area measurement was 66 mm2.
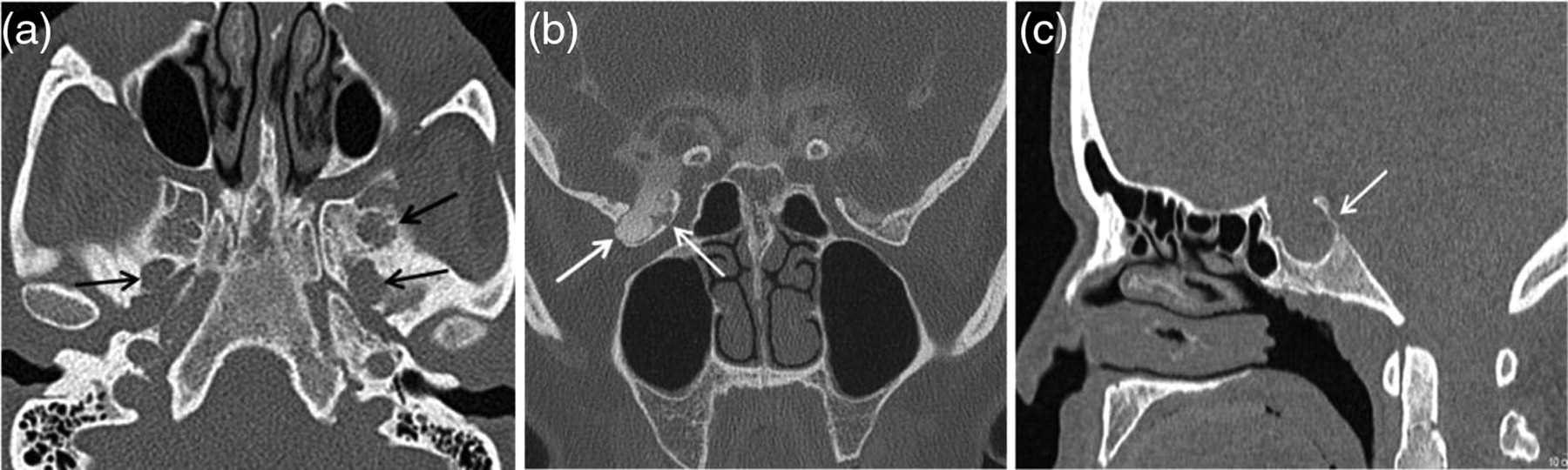
Axial (a) non-contrast CT image shows osseous erosion through the greater wing of the sphenoid bone with widening of both FO. Coronal (b) image from CT cisternography confirms the osteodural defect. This patient demonstrated ON sheath distention, posterior globe flattening, and an empty sella as seen on the sagittal (c) CT image
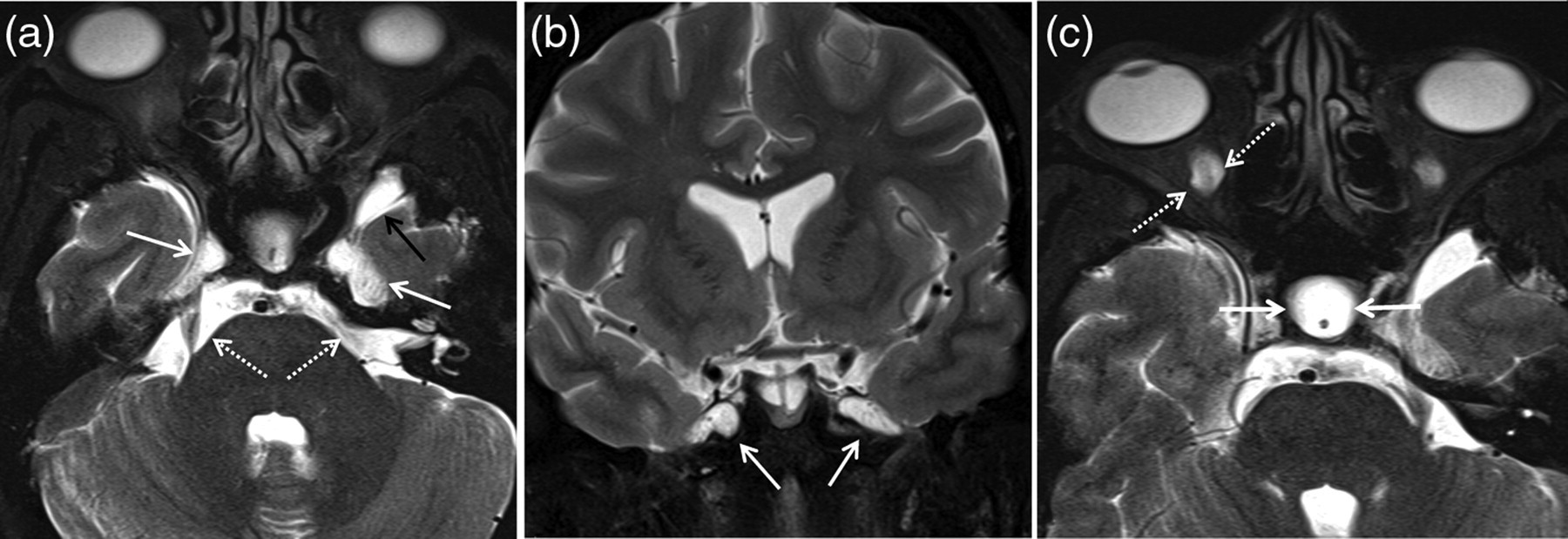
Axial (a) and coronal (b) T2-weighted images demonstrate arachnoid space herniation through the petrous apex (solid white arrows in a and b), extending from bilaterally prominent Meckel's caves (dashed white arrows). The extra-axial space anterior to the middle cranial fossa is also very prominent (solid black arrow). This patient also had a constellation of findings, an empty sella (solid white arrows) and ON sheath widening (dashed white arrows) as seen on the axial (c) T2-weighted MR image, and FO widening
MRI findings
The MRI findings of patients with confirmed IIH and controls are detailed in Table 3. Empty sella (P < 0.001), posterior globe flattening (P < 0.001), ON tortuosity (P < 0.001), and ON sheath distension (P < 0.001) were significantly associated with IIH. No significant association between slit ventricles (P = 0.229) and IIH was found. Sixty-six percent (29/44) of our patients had partially or completely empty sella compared to none in the control group. In addition, 66% (29/44) of our patients had posterior globe flattening. Vertical tortuosity of the ON and ON sheath distention was present in 55% (24/44) and 52% (23/44) of the cases, respectively. Twelve cases (27%) had all four imaging findings commonly described in IIH, including a partially or completely empty sella, posterior globe flattening, ON tortuosity, and ON sheath distention, whereas 12 others (27%) had three of four findings.
Frequency of classic MR findings of IIH in the patient group and the control group with statistical comparisons
ON, optic nerve
On an incidental note, 20% (9/44) of patients were observed to have low-lying cerebellar tonsils (Fig. 7). However, no statistically significant association between this finding and IIH was found (P = 0.133). The tonsils were not more than 5 mm below the foramen magnum to be considered a Chiari I malformation.
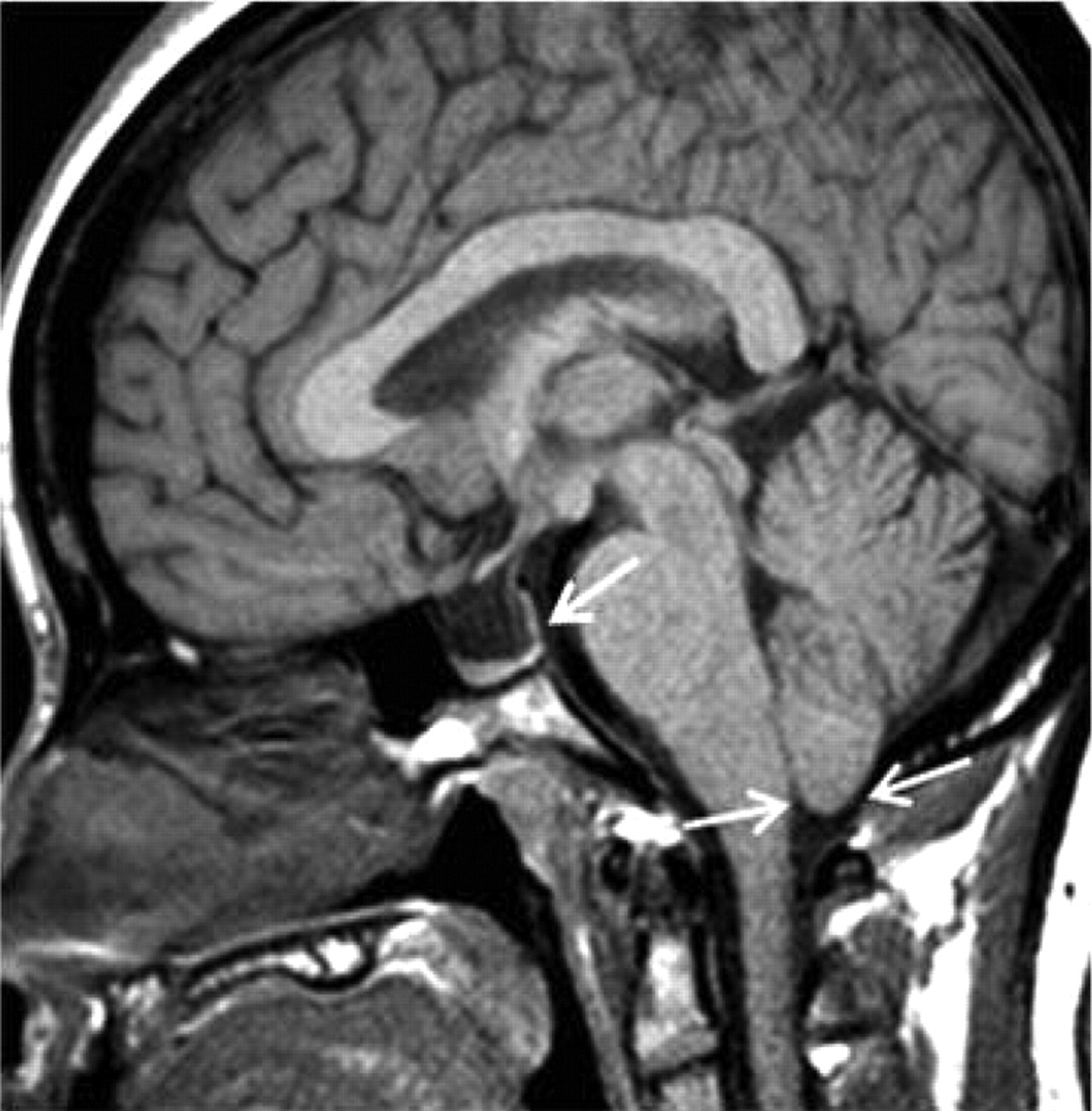
Sagittal T1-weighted MR image demonstrates low lying cerebellar tonsils. Also, note the partially empty sella
Discussion
The presence of elevated ICP in patients with CSF leaks is supported by multiple studies. Spontaneous CSF leaks presenting as otorrhea or rhinorrhea have been postulated to be manifestations of IIH (24, 25). Chronically elevated and pulsatile CSF could cause osseous erosions over an extended period of time leading to CSF leaks by means of herniation of the arachnoid spaces through osteodural defects (26, 27). Furthermore, many of the patients with spontaneous, atraumatic CSF leaks have demonstrated empty sellas on imaging, and were found to have similar demographic features as those seen in IIH, i.e. middle-aged, obese females (28–31). Schlosser et al. investigated 16 patients with spontaneous CSF leaks and found 10 of them to have elevated ICP with similar radiological and physical features to IIH (28). In another study by Schuknecht et al. investigating CSF rhinorrhea, several osteodural defects were identified within the ethmoid and the sphenoid sinuses. Although CSF pressure measurements were not made, 63% of their patients were found to have empty sellas (26).
An anatomical relationship to pneumatized spaces such as the sphenoid sinus, ethmoid sinus, or the mastoid air cells is needed with progression of osseous erosions at adjacent locations, such as the cribriform plate or the tegmen tympani (26, 32, 33) for osteodural defects to manifest as CSF leaks. Osseous erosions in areas adjacent to non-pneumatized spaces would not be expected to cause CSF leaks, such as in the cases we demonstrated in Figs. 1 and 2. These patients did not have CSF leaks, however, both demonstrated bilateral FO widening. Further evaluation of these patients with CT cisternography confirmed arachnoid space herniations but did not reveal CSF leaks. This could either be explained by the pressure effect of CSF, not through arachnoid herniation but by a direct effect, as dura covers the FO through which V3 passes or by the limitations of cisternography. In fact, MR cisternography often fails to demonstrate contrast accumulation in the distended perioptic nerve sheath. The underlying pathophysiology that leads to osteodural defects could cause FO widening with the same mechanism of chronically increased CSF pressure. Other foraminal widenings could potentially be observed in cases of IIH as well; however this would require a dural reflection overlying the foramina, for chronic CSF pressure to exert its effect. We did not include foramen lacerum to our evaluation due to the lack of an overlying dural reflection, its highly variable shape, its difficulty in measurement, and the fact that pressure effects from the internal carotid artery cannot be isolated. Foramen spinosum was not considered for evaluation due to its small size.
In this study we concentrated on means to measure the effect of increased CSF pressure and/or pulsatility on bone causing osseous erosions by widening of the FO and to demonstrate any related osseous changes in the skull base. To our knowledge FO widening in IIH has not been described in the literature, and we believe that it presents a manifestation of osseous erosion. With a cut-off value of 30 mm2 we had a sensitivity and specificity of 50% and 81%, respectively, with a positive predictive value of 73%. With this arbitrary cut-off, we failed to diagnose 24 patients (24/48) and misdiagnosed nine patients (9/48). While we were able to demonstrate FO widening in patients with IIH with significant increase in area measurements, whether this will be of clinical utility and aid in accurate diagnosis in day-to-day practice remains to be determined. Although there was some overlap in the measurements, the value of an objective measurement method is unarguably valuable. We believe that this finding could be utilized as an adjunct feature especially in cases of longstanding IIH demonstrating noticeable FO enlargement. It could also be argued that the small areas of the FO could prove to be a challenge in practicality of obtaining measurements; however we had good intra- and inter-rater agreement indicating repeatability and reproducibility. For practical purposes, the accuracy of subjective evaluation of FO enlargement based on pure observation of CT scans could be made in future studies.
Multiple studies have revealed the presence of structural changes in patients with IIH. We confirm several previously described imaging findings on MRI scans associated with IIH. The incidence of empty sella in cases of IIH varies widely (10–94%), probably related to discrepancies in definition (19). Although empty sella is highly associated with IIH, the underlying suggested pathogenesis of altered CSF dynamics on the diaphragma sellae and the pituitary gland only applies to a number of patients. This finding should probably be considered a normal variant in the vast majority of asymptomatic patients, which is estimated to be present in 5–6% of normal individuals (19, 28). Sixty-four percent of our patients were found to have a partially or completely empty sella compared to none in our control group.
The ON and globe findings are significant in that they probably better predict papilledema (34). In a review of the MRI findings of 30 patients, Agid et al. (35) found that four of the traditional imaging findings were significantly associated with IIH (empty sella, posterior globe flattening, ON sheath distention, ON tortuosity); however, they concluded that only posterior globe flattening had high enough specificity to be of clinical use. Lim et al. studied similar MRI findings in 23 children and found that a combination of three or more findings of globe flattening, empty sella, protrusion of the ON head, and tortuosity of the ON would increase specificity to 95% for the diagnosis of IIH (36). Although there are many initial studies as early as Dandy's report in 1937 that suggest the association of slit-like ventricles and enlarged extra-axial CSF spaces with IIH (1, 14, 37), we believe that this finding is a normal variant for young patients. This is supported by multiple other studies and our results (16, 35).
There are multiple recent reports that propose the association of dural venous sinus stenosis or thrombosis in patients with IIH. We do not routinely obtain MR venograms in patients with typical presentations of IIH; therefore, we did not investigate for the presence of these findings. Further studies evaluating dural venous sinus stenosis may shed light on the underlying pathogenesis of at least a subgroup of patients with IIH, and better define the role of sinus stenosis stenting as a treatment option (13, 38–40).
Our study has weaknesses in that it was not prospective and therefore did not allow us to follow patients over a period of time to monitor the progression of findings and osseous erosions. We also did not correlate the findings with the duration of symptoms. Given the nature of the disease, a predominant portion of our patient population was indeed obese, consistent with the overwhelming data showing a relationship between IIH and obesity. We did not examine an independent relationship between obesity and foramen ovale sizes. Neither did we select our control population from obese patients. We believe that if we had strictly included obese patients in the control group, there may have very well been undiagnosed or subclinical patients having increased CSF pressures complicating our results. This could represent another potential weakness of our study. Our CT head protocol for headaches does not include routine coronal plane reconstructions. Given the retrospective nature of our study, the source data were no longer available to allow for full resolution reformats and we could not obtain transverse measurement of the FO in the coronal plane that could prove to be more accurate than axial measurements. Further studies are needed to demonstrate FO widening in IIH patients as a manifestation of osseous erosion.
Patients with IIH have a typical clinical presentation; however, imaging findings associated with IIH lack adequate sensitivity or specificity for a confident diagnosis. The utility of imaging has been to exclude other causes that lead to increased ICP rather than confirming or diagnosing IIH. The initial study ordered in line of investigation during the work-up of patients with headache is usually a CT scan of the head. In the appropriate clinical setting, the finding of bilaterally widened FO could be used to raise the possibility of IIH and prompt further work-up which may include an MRI or lumbar puncture to evaluate for CSF pressure.
In conclusion, our study supports widening of the FO as an additional imaging marker for IIH, which may be incorporated into the evaluation of patients suspected to have this condition.
Footnotes
Acknowledgements
Part of this manuscript was presented at the 2010 RSNA scientific meeting as an educational exhibit and received a “Certificate of Merit” award.