
Abstract
In the last decade contrast-enhanced magnetic resonance angiography (CE-MRA) has gained wide acceptance as a valuable tool in the diagnostic work-up of patients with peripheral arterial disease.
This review presents current concepts in peripheral CE-MRA with emphasis on MRI technique and contrast agents.
Peripheral CE-MRA is defined as an MR angiogram of the arteries from the aortic bifurcation to the feet. Advantages of CE-MRA include minimal invasiveness and lack of ionizing radiation. The basic technique employed for peripheral CE-MRA is the bolus-chase method. With this method a paramagnetic MRI contrast agent is injected intravenously and T1-weighted images are acquired in the subsequent arterial first-pass phase. In order to achieve high quality MR angiograms without interfering venous contamination or artifacts, a number of factors need to be taken into account. This includes magnetic field strength of the MRI system, receiver coil configuration, use of parallel imaging, contrast bolus timing technique, and k-space filling strategies. Furthermore, it is possible to optimize peripheral CE-MRA using venous compression techniques, hybrid scan protocols, time-resolved imaging, and steady-state MRA.
Gadolinium(Gd)-based contrast agents are used for CE-MRA of the peripheral arteries. Extracellular Gd agents have a pharmacokinetic profile similar to iodinated contrast media. Accordingly, these agents are employed for first-pass MRA. Blood-pool Gd-based agents are characterized by prolonged intravascular stay, due to macromolecular structure or protein binding. These agents can be used for first-pass, as well as steady-state MRA. Some Gd-based contrast agents with low thermodynamic stability have been linked to development of nephrogenic systemic fibrosis in patients with severe renal insufficiency.
Using optimized technique and a stable MRI contrast agent, peripheral CE-MRA is a safe procedure with diagnostic accuracy close to that of conventional catheter X-ray angiography.
Imaging of the peripheral arteries (aortic bifurcation to the feet) is important in treatment planning of patients with peripheral arterial disease (PAD). For this purpose different imaging modalities are in use. This includes conventional X-ray angiography (digital subtraction angiography [DSA]), computed tomography angiography (CTA), duplex Doppler ultrasound (dd-US), and magnetic resonance angiography (MRA). Each modality has both advantages and limitations.
DSA is regarded as the gold standard method for peripheral arterial imaging. The main advantage of DSA is high spatial and temporal resolution; furthermore diagnostic DSA can be combined with endovascular interventions. Drawbacks are radiation exposure, use of nephrotoxic iodinated contrast agents, and risk of procedure-related complications. The rate of clinically significant complications (hemorrhage, embolism) following peripheral DSA is approximately 2% (1). Technological advances in multidetector CT systems have made peripheral CTA feasible. Advantages of CTA are minimal invasiveness, short examination times, and high diagnostic accuracy (2, 3). Limitations are use of nephrotoxic contrast agents, decreased diagnostic confidence in heavily calcified vessels (blooming effect), and use of ionizing radiation. Advantages of dd-US include non-invasive procedure, wide availability, and no harmful side-effects; functional assessments are possible with acquisition of real-time images. Considerable operator dependency is the main drawback of dd-US (4, 5). Furthermore, dd-US does not provide a roadmap of the peripheral arteries for use in treatment planning.
MRA applications include both unenhanced and contrast-enhanced techniques. Although unenhanced time-of-flight and phase-contrast MRA techniques have proven feasible for accurate detection of PAD (6–11), the methods have never gained widespread clinical use, primarily because of long acquisition times and flow-related artifacts. However, interest in unenhanced peripheral MRA using balanced steady-state free precession (b-SSFP) and ECG-gated subtraction techniques is growing (12–14). Two factors have contributed to this interest. First, developments in MRI technology have lead to reduced acquisition times, making some newer MRA methods clinically practical. Secondly, some MRI contrast agents have been associated with the devastating disease nephrogenic systemic fibrosis (NSF).
Contrast-enhanced (CE) MRA is widely used for detection of PAD (15). Advantages of CE-MRA are minimal invasiveness, no utilization of ionizing radiation, high diagnostic accuracy (16, 17), and cost-effectiveness (18). Limitations are problems related to metal implants, pacemakers, claustrophobic patients, and gadolinium-based contrast agents.
Important technical aspects of peripheral CE-MRA are presented in this review. Furthermore, use of different types of MRI contrast agents for peripheral CE-MRA is described. Unenhanced MRA techniques are described elsewhere (12, 19, 20). This article focus on peripheral CE-MRA in the adult patient population.
Peripheral MRA technique
Single- vs. multi-station contrast-enhanced MRA
CE-MRA was introduced in the early 1990s (21, 22). In CE-MRA, a paramagnetic gadolinium-based contrast agent is injected intravenously, and images are acquired in the subsequent arterial first-pass phase. As the contrast agent has T1 shortening effect, arteries appear bright on T1-weighted MRI images. Three-dimensional (3D) spoiled gradient echo sequences are usually employed for CE-MRA studies, as this allows fast data acquisition. Furthermore, the volumetric 3D data-sets make it possible to perform multiplanar reformations (MPRs) and maximum intensity projections (MIPs) rendering DSA-like angiograms (23).
Early CE-MRA studies were limited to a single field of view (FOV), so-called single-station CE-MRA (21–23). The single-station technique is useful for MRA of arteries in a limited anatomical area, for example the abdominal aorta, renal arteries, or the carotids. To perform peripheral CE-MRA from the aortic bifurcation to the feet, multiple overlapping FOVs need to be imaged (multi-station boluschase CE-MRA). Improvements in MRI hardware with faster gradients and automatic table translation over multiple FOVs made peripheral multi-station CE-MRA feasible in the late 1990s (24–26). The technique has been improved ever since, both regarding temporal and spatial resolution. In most cases peripheral CE-MRA consists of imaging in three stations: (a) aortic bifurcation and iliac arteries; (b) femoral arteries; and (c) run-off vessels. An example is shown in Fig. 1, and typical imaging parameters are shown in Table 1. Systematic reviews report CE-MRA sensitivity and specificity for detection of significant arterial stenosis (≥50% luminal narrowing) above 0.90 (16, 27–29). With the multi-station technique image acquisition needs to be fast enough to keep up with the arterial bolus, as it propagates distally. If this is not the case, venous contamination will be present and degrade the quality of the MR angiograms (Fig. 2). Opposed to the stepwise patient table movement in peripheral multi-station CE-MRA, continuous table MRA has been developed (30–33). Using this newer approach the peripheral arteries are imaged in one continuous acquisition, without breaks for table translation.

Peripheral CE-MRA in a patient with peripheral arterial disease. T1-weighted MIP shows bright arteries due to the T1-shortening effect of the MRI contrast agent (0.2 mmol/kg body weight gadoterate). Note, occlusion of the left superficial femoral artery (arrow). In this patient, bolus-acquisition timing was successful with resulting good arterial contrast and no venous overlay

MIP showing venous contamination. In this patient, acquisition was performed too late, i.e. after the arterial first-pass phase. The result is reduced diagnostic quality due to servere venous overlay
Example of scan parameters in peripheral CE-MRA @ 1.5T
The diagnostic quality in peripheral MR angiograms depends upon a large number of factors, each of which will be discussed below. In general, it is desirable to reduce scan time (increase temporal resolution) to ensure imaging in the arterial first-pass. Furthermore, the aim is to obtain images with high spatial resolution to maximize anatomical detail and improve diagnostic accuracy in stenosis detection. Unfortunately, improvements in temporal resolution decrease spatial resolution and vice versa.
Magnetic field strength
As with other MRI applications, the magnetic field strength (B0) of the MRI system is a significant factor influencing image quality. Increasing the B0 leads to an increase in the achievable MRI signal. The signal-to-noise ratio (SNR), a measurement of the MRI signal, scales linearly with the B0. Thus, an increase from 1.5 to 3T doubles the SNR. With large SNR voxel size may be decreased. Widespread use of 3T MRI systems for peripheral CE-MRA in the recent years has influenced the size of acquisition voxels (34, 35). Commonly, submillimeter voxels are acquired; something that has not been possible in 1.5T systems. However, image quality can also be degraded at higher field strengths. Artifacts relating to magnetic field inhomogeneities/susceptibility are extensive at 3T compared with lower field strengths (36). These are general limitations in MRI and not specific for peripheral CE-MRA.
Receiver coils
Different coil configurations can be used for reception of the MRI signal in peripheral CE-MRA. In the simplest form, images are acquired using the MRI system's built-in body body coil (24–26). Alternatively, dedicated vascular surface coils can be used (37). As the received MRI signal is dependent upon the distance to the imaged anatomy, the MRI signal favours from application of surface coils. Thus, higher SNR is achieved with surface coils as compared with acquisition performed with the built-in body coil. Consequently, surface coils are used to improve spatial resolution in peripheral CE-MRA. Another advantage with surface coils is the possibility of applying parallel imaging (discussed below). Currently, almost all clinical peripheral MRA examinations are performed using dedicated vascular coils (37, 38).
Parallel imaging
In recent years, parallel imaging has been established as a powerful method to improve spatial and temporal resolution in both peripheral CE-MRA and MRI in general. In peripheral MRA, the main advantage of parallel imaging is that data acquisition times can be reduced by a factor of 2 or more (the acceleration factor, AF). Alternatively, spatial resolution can be increased with unaltered acquisition time. In parallel imaging, data are acquired simultaneously using multiple surface coils with different spatial sensitivities (39, 40). Not all lines of k-space are filled, but the missing data are calculated from the spatial sensitivities of the surface coils. Importantly, parallel imaging implies a SNR penalty that scales with √2 × AF. This is due to the incomplete k-space filling. Hence, the AF is limited by the SNR reduction. Due to the intrinsic higher SNR in 3T MRI systems, as compared with 1.5T, higher AFs may be used at the higher field strength. Typical AFs in peripheral CE-MRA are 2 (1.5T) and 3–4 (3T).
Bolus timing
The technical quality of peripheral CE-MRA is heavily dependent on images being acquired in the arterial first-pass phase. Hence, contrast injection must be performed in a reproducible manner, and the time point for starting image acquisition must be adjusted in each patient. Today, most centers use automatic power injectors for contrast injection in peripheral CE-MRA. Both mono- and bi-phasic injection protocols have been advocated for. The benefit of bi-phasic injection is an elongation of the contrast bolus, potentially extending the arterial first-pass phase (41). Importantly, a saline chaser, to propagate all the contrast medium out of the connecting lines and into the circulation, should follow the contrast injection. Manual contrast injection is also possible, with inherent operator-related limitations regarding accuracy of injection rates and volumes (42). The intravenous cannula used for contrast injection is typically a size 20G placed in the antecubital fossa.
Different bolus-timing strategies are useful to adjust image acquisition to the arterial first-pass phase (43). It is necessary to use such strategies as the hemodynamics differ in each patient, due to, for instance, ischemic heart disease and extent of atherosclerosis in the peripheral arteries. The most simple bolus-timing strategy is the so called ”best guess” strategy, in which time from contrast injection to acquisition start is predefined after taking into account different factors (cardiac output, age, PAD stage, etc.). It is obviously not a very robust strategy, and is therefore rarely used. On the contrary, test bolus and real-time bolus detection strategies are commonly used in peripheral CE-MRA. With the test bolus technique a small volume of contrast agent is injected (for instance 2 mL) followed by a fast repetitive imaging sequence over the abdominal aorta. The resulting images are used to identify the time point at which contrast enhancement peaks, i.e. it defines the time of the arterial first-pass phase. With this information delay between injection start and image acquisition in the following peripheral CE-MRA can be accurately set. Importantly, the same injection rate should be used for the test bolus and contrast bolus. Using the real-time bolus detection strategy, images of the abdominal aorta are acquired in a rapid pace after injection of the contrast bolus. When the operator detects aortic peak enhancement, the peripheral bolus-chase MRA is started.
k-space filling
Another important technical factor in CE-MRA is the method of k-space filling. To achieve MR angiograms with good arterial contrast and minimal venous contamination, the central part of k-space must be acquired during peak of the contrast bolus, while the peripheral part may be acquired later. This is because the central part of k-space determines image contrast, while the peripheral parts determine image detail. In peripheral CE-MRA it is common to employ linear k-space filling for the proximal station(s), while centric k-space filling is used for the distal stations. The use of linear k-space filling proximally ensures that peripheral k-space lines are acquired during rise of the arterial bolus, while the contrast-deciding central lines are acquired during peak of contrast bolus. Distally, contrast bolus is typically peaking when image acquisition commences. Accordingly, central part of the k-space must be acquired first (centric k-space filling) and the peripheral parts last.
Modified bolus-chase peripheral CE-MRA
Conventional peripheral CE-MRA is based on sequential bolus-chase acquisition over three stations from the aortic bifurcation to the feet (Fig. 3a). As the lower leg region is imaged last, this station is most likely to suffer from venous contamination (44). Thus, interest in techniques to optimize peripheral image quality/decrease venous contamination has been growing. Important optimization techniques are hybrid scan protocols and use of venous compression.

Schematic layout of peripheral MRA protocols: (a) Consecutive MRA acquiring data from stations 1 to 3 using a single contrast injection. (b) Hybrid MRA using two contrast injections. Acquisition of data from stations 1 and 2 is performed after first contrast injection, while station 3 is imaged following second injection. The syringe icons mark the contrast injections
Hybrid scan protocols are based on dividing the contrast injection into two separate injections (45–47). Following first injection, acquisition of the proximal stations, i.e. pelvic and thigh regions are performed in the arterial first-pass phase. After the second injection, acquisition of the lower leg region is performed in the new arterial first-pass phase (Fig. 3b). Such split-bolus technique is feasible due to the pharmacokinetic profile of MRI contrast agents (excluding blood-pool agents) with rapid distribution to the extracellular compartment following the arterial phase. It seems advantageous to use slightly larger contrast volume for the second injection, as residual contrast from first injection in the stationary tissues can decrease image contrast. For example 40% of the contrast dose can be injected as the first bolus, and the remaining 60% as the second bolus. However, if subtraction techniques are applied, it is not necessary to adjust contrast bolus volume between injections.
Venous compression techniques, using sub-systolic compression of either the thigh or calf, have proven effective in reducing peripheral venous contamination in CE-MRA (48–53). The compression technique is easy to implement, as the only requirement is placement of blood-pressure cuffs around the thigh or calf. Cuffs are inflated to sub-systolic pressures in the range of 50–60 mm Hg. The exact mechanism behind the hemodynamic changes induced by the compression technique remains unknown. A number of hypotheses have been formulated: one hypothesis is that increased venous pressures in the calves prolong the arterial transit time through a backpressure mechanism in the capillary bed (49). Another hypothesis is that venous stasis leads to dilution of the contrast agent in the veins (53). Also local arteriolar vasoconstriction as a response to increased capillary pressure, has been proposed as the mechanism behind reduced venous contamination with cuff compression (54). Cuff compression should not be used in patients with superficial vascular bypass grafts due to the risk of thrombosis.
Time-resolved MRA
Another important technique to improve performance of CE-MRA is time-resolved MRA. This technique employs fast imaging, with multiple acquisitions of the imaged arteries. The technique is most often used in the calf region, as the multiple acquisitions provide a near optimal solution to arterial phase imaging without venous overlay (55). However, a drawback of the technique is that a separate contrast injection must be performed for both the multi-station bolus-chase MRA of the entire peripheral arterial tree, as well as for the selective time-resolved calf MRA. Technically, time-resolved MRA is characterized by k-space segmentation from the center and out. k-space is filled in an elliptic centric order. Furthermore, the center of k-space is sampled at higher frequency than the peripheral segments, a technique often referred to as Time-Resolved Imaging of Contrast Kinetics (TRICKS). In diabetics with small vessel disease, time-resolved MRA has proven effective to image the calf arteries, a challenging task with conventional multi-station peripheral MRA techniques (56, 57).
Steady-state MRA
A newer concept in CE-MRA is steady-state imaging using blood-pool contrast agents, characterized by prolonged intravascular stay compared to conventional extracellular agents (see below). When using blood-pool agents the imaging period can be extended far beyond the short arterial first-pass phase (58, 59). In this steady-state phase, MR angiograms with largely improved spatial resolution may be acquired, as there is no significant time constraint (60). Steady-state MRA provide images of both arteries and veins. However, the excellent spatial resolution facilitates artery-vein separation (Fig. 4). In our experience, it is rarely a problem to differentiate arteries from veins in steady-state MR angiograms. When difficulties occur, it is most common in the lower leg region, due to the small vessel diameters below the knee. Blood-pool agents may also be used for first-pass imaging, and a combined first-pass/steady-state MRA approach of the peripheral arteries has proven to improve results compared to first-pass imaging alone (61).

Steady-state MRA of the calf arteries. The image was acquired 10 min after injection of the blood-pool contrast agent gadofosveset trisodium at a dose of 0.03 mmol/kg body weight. The high-spatial-resolution MR angiogram (0.6 mm isotropic) allows artery-vein separation. Arrows point to calf arteries
Image postprocessing
Computer work stations are used for image postprocessing and viewing of the 3D data-sets produced in peripheral CE-MRA. The most important postprocessing techniques are multiplanar reformations (MPR), maximum intensity projection (MIP), and volume rendering (VR). MPR allows imaging of the anatomy in all planes. Image quality of MPRs are improved if the acquisition voxels are isotropic. Of special interest in CE-MRA is curved MPR, that allows reformation along tortious vessels. MIPs produce images similar to conventional DSA. The method is excellent to present a quick overview of the entire peripheral arterial tree. By combining multiple MIPs, 3D rotational MIPs can be made. Commonly the MRI system is set up to produce standard MIPs. VR is another method to produce 3D images of the imaged anatomy. The technical foundation of VR is different than MIP. Although postprocessing may produce impressive MIPs or volume rendered images, diagnosis of arterial stenosis should always be confirmed using source images.
Arterial stenosis grading
In PAD patients arterial segments are usually classified as either insignificantly diseased (≤49% diameter reducition/stenosis) or significantly diseased (≥50% diameter reducition/stenosis and occlusions). To be used in the clinical setting, imaging methods should be both sensitive as well as specific for detection of significantly stenosed arteries. An important factor to achieve high diagnostic accuracy in peripheral CE-MRA is the spatial resolution. This has been investigated by Hoogeveen et al., who showed that reliable diagnosis of arterial stenoses in MRA requires at least three pixels to be present across the arterial lumen (62). In the the lower leg this may be challenging due to the small vessel diameters of 2–3 mm in this area.
Another important consideration is that CE-MRA only depicts the arterial lumen (luminography). As the earliest stages of atherosclerosis are contained in the arterial walls due to expansive remodelling, CE-MRA may fail in detecting these lesions. However, this limitation is not specific for CE-MRA, other imaging modalities like CT angiography and DSA are also luminographic and have similar limitations.
Patient-related factors
Before referring patients to peripheral CE-MRA a number of patient-related factors must be considered. In generel, pacemakers, neurostimulating devices, otological implants, and metallic foreign bodies in the eyes are contraindications for MRI. Claustrophobia may also be a problem. As peripheral CE-MRA requires imaging in high field MRI systems, use of open bore magnets are not an option. Orthopedic implants (for example hip/knee prosthesis) and arterial stents are not contraindications for MRA. However, severe susceptibility artifacts from such implants may interfere with diagnostic assessment of nearby arterial segments.
MRI contrast agents
An overview gadolinium-based contrast agents is presented in this section. A more comprehensive review of MRI contrast agents can be found elsewhere (63, 64).
Classification and pharmacokinetics
Gadolinium-based contrast agents (Gd-CA) contain the paramagnetic Gd3 + ion. As free Gd is highly toxic, all Gd-CA consist of Gd chelated to a ligand that should prevent cellular uptake of free gadolinium. Depending on the chemical structure of the ligand, Gd-CA are classified as linear or macrocyclic, as well as ionic or non-ionic (Table 2, Fig. 5). Furthermore, Gd-CA are divided into extracellular, hepatobiliary, and blood-pool agents according to their pharmacokinetic profile.
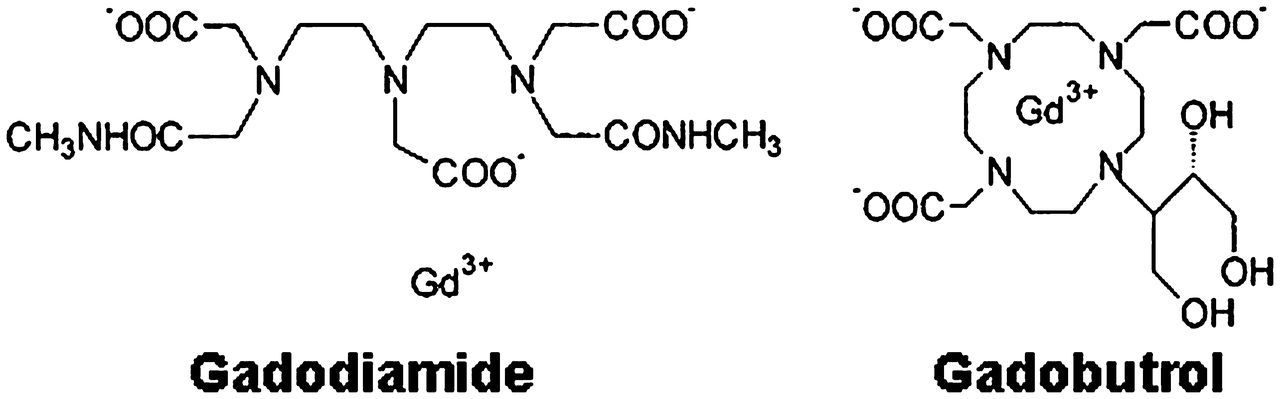
Molecular structure of the non-ionic extracellular agents gadodiamide and gadobutrol, with linear and macrocyclic structure, respectively
Approved gadolinium-based MRI contrast agents
Extracellular Gd-CA are the most commonly used MRI contrast agents. After intravenous administration, the pharmacokinetic profile is similar to that of iodinated contrast agents. Following the arterial first-pass phase the agents are distributed to the extracellular compartment. Elimination is exclusively by passive glomerular filtration in the kidneys. In patients without renal insufficiency, 98% of the administered Gd-CA is excreted within 24 h (65).
The hepatobiliary Gd-CA (liver specific agents) consist of gadobenate dimeglumine and gadoxetate disodium. The former behaves mainly like an extracellular agent after intravenous administration. However, it has greater relaxivity because of weak protein binding in plasma (66). Gadobenate is suitable for CE-MRA due to the high relaxivity and initial distribution like extracellular agents. Occasionally, gadobenate is referred to as a blood-pool agent because of its protein binding. However, the binding is weak and transient, and gadobenate is therefore not a true blood-pool agent. Gadobenate is predominantly eliminated by renal glomerular filtration, with a smaller percentage of the administered dose (4%) is eliminated by the biliary route. Selective liver imaging is therefore possible with late phase acquisitions.
Gd-based blood-pool contrast agents are characterized by prolonged intravascular stay (67). Accordingly, MR angiographic applications using these agents encompass both first-pass and steady-state MRA. Due to the long plasma half-life of blood-pool agents, they are often referred to as intravascular contrast agents. Gd-based blood-pool agents are classified according to size into macro- and low-molecular agents. The former consist of macromolecules with multiple gadolinium ions bound to the surface. The blood-pool effect of these agents is due to the large size of the macromolecules, ensuring low or absent leakage to the extracellular compartment. The Gd-based macromolecules are high relaxivity agents because their large size leads to slow rotational dynamics (63). Elimination is by glomerular filtration in the kidneys. Macromolecular agents (Gd-DTPA-17 and gadomelitol) are undergoing trials (68, 69). Gadofosveset trisodium is the most important agent in the low-molecular group of Gd-based blood-pool agents. This agent is a monomer, which blood-pool property is due to non-covalent binding to protein (albumin) in human plasma (70). Gadofosveset is a high-relaxivity agent due to slow molecular rotational speed when bound to albumin (66). In human plasma, 4–20% of gadofosveset follows the same distribution as extracellular Gd-CA. Elimination of gadofosveset is predominantly renal filtration, and to a lesser extent hepato-biliary excretion (9%) (65, 70). Gadofosveset has been the first blood-pool MRI contrast agent to become commercially available, however other agents are under development (71).
MRI contrast agents in peripheral CE-MRA
When performing peripheral CE-MRA the simplest approach is to use an extracellular agent. In the literature, the majority of lower extremity MRA studies have been performed using extracellular agents. Most commonly, contrast dose is adjusted according to the patients' weight, with single, double, and triple doses referring to 0.1–0.3 mmol/kg body weight, respectively. Rarely fixed contrast volumes are used. Imaging in 3T MRI systems holds potential for use of lower contrast doses than at 1.5T, due to longer tissue T1-values at 3T and the associated more efficient contrast-induced T1-shortening (35, 72).
Extracellular agents are formulated at different concentrations. Most have a concentration of 0.5 mol/L. Gadobutrol is formulated at 1 mol/L. The higher concentration of gadobutrol leads to a more compact contrast bolus, which have proven advantageous for peripheral CE-MRA (73, 74).
The high-relaxivity agent gadobenate is commonly used for peripheral CE-MRA. Studies have shown better performance with this agent, as compared to extracellular agents at equimolar doses, due to the high-relaxivity profile of gadobenate (75–77).
The blood-pool agent gadofosveset has markedly higher relaxivity than both gadobenate and extracellular agents (66). Accordingly, gadofosveset is administered at lower doses. The standard dose in gadofosveset-enhanced MRA is 0.03 mmol/kg body weight (59).
Nephrogenic systemic fibrosis
In many years gadolinium-based agents were considered to have an excellent safety profile. However, in recent years intravenous administration of gadolinium-based agents has been linked to development of nephrogenic systemic fibrosis (NSF), a potentially fatal disease causing fibrosis of both the skin and internal organs (78–80). NSF has solely been reported in patients with renal insufficiency, including dialysis patients (81). So far, NSF cases have been seen following administration of linear gadolinium-based agents (gadodiamide and gadopentate), with most cases being caused by gadodiamide. No unconfounded cases of NSF following administration of high-relaxivity agents have been reported in the peer-reviewed literature (64, 82). Two cases of NSF following exposure to the macrocyclic agent gadobutrol have been reported (83, 84). However, it is unclear whether or not the case reported by Elmholt et al. fulfill the clinicopathological NSF definition (85). There is evidence that cumulative doses of gadolinium increase the risk of NSF (86). It is believed that release of free Gd from their ligands play a role in NSF development. However, the exact pathophysiological mechanisms of NSF remain unknown. Currently, no curable treatment of NSF is available. Due to the awareness of NSF in the MRI community, the incidence of new NSF cases is very low. According to the guidelines on contrast media issued by the European Society of Urogenital Radiology (ESUR), the smallest amount of contrast medium necessary for a diagnostic result should be used. A clinically well-indicated MRI examination should never be denied and an agent that leaves the smallest amount of gadolinium in the body should always be used (87). Furthermore, the ESUR guidelines contain specific recommendations on use of the different Gd-based agents.
The incidence of non-renal adverse reactions is lower for Gd-based agents than for non-ionic iodinated contrast media. Prospective studies on Gd-based agents with different osmolality have not shown any difference in the incidence of non-renal adverse reactions (64).
Conclusion
Over the last decade CE-MRA has gained wide acceptance as an effective imaging method in the diagnostic work-up of patients with peripheral arterial disease. With optimized MRI technique the diagnostic accuracy of peripheral CE-MRA is close to that of DSA. However, it may be challenging to achieve diagnostic image quality. Especially venous contamination in the lower leg region causes technical failure. Knowledge of both MRI technique and contrast agents is fundamental to design effective peripheral CE-MRA imaging protocols.