
Abstract
Manganese is one of the most abundant metals on earth and is found as a component of more than 100 different minerals. Besides being an essential trace element in relation to the metabolic processes in the body, manganese is also a paramagnetic metal that possesses similar characteristics to gadolinium with regards to T1-weighted (T1-w) magnetic resonance imaging (MRI). Manganese, in the form of manganese (II) chloride tetrahydrate, is the active substance in a new targeted oral contrast agent, currently known as CMC-001, indicated for hepatobiliary MRI. Under physiological circumstances manganese is poorly absorbed from the intestine after oral intake, but by the use of specific absorption promoters, L-alanine and vitamin D3, it is possible to obtain a sufficiently high concentration in the liver in order to achieve a significant signal enhancing effect. In the liver manganese is exposed to a very high first-pass effect, up to 98%, which prevents the metal from reaching the systemic circulation, thereby reducing the number of systemic side-effects. Manganese is one of the least toxic trace elements, and due to its favorable safety profile it may be an attractive alternative to gadolinium-based contrast agents for patients undergoing an MRI evaluation for liver metastases in the future. In this review the basic pharmacological and pharmaceutical aspects of this new targeted oral hepatobiliary specific contrast agent will be discussed.
Most magnetic resonance imaging (MRI) contrast agents used in the clinic today contain the paramagnetic metal gadolinium (Gd), which is administered intravenously (i.v.) as chelate compounds. Some of these agents, such as gadoxetic acid (Primovist®/Eovist®, Bayer Schering Pharma AG, Berlin, Germany) and gadobenate dimeglumine (MultiHance®, Bracco Imaging S.p.A., Milan, Italy), have hepatobiliary-specific characteristics and are used for the detection and characterization of focal liver lesions. Another paramagnetic metal, manganese, possesses similar characteristics to Gd with regards to T1-weighted (T1-w) MRI. Manganese is a transition metal that contains five unpaired electrons as the manganese (II) ion (Mn2+). These unpaired electrons facilitate T1 relaxation by interacting with nearby hydrogen protons of water molecules (1). An i.v. formulation where manganese is chelated in a complex of dipyridoxyl diphosphate (mangafodipir, Teslascan®, GE HealthCare, Inc., Princeton, NJ, USA) was clinically available for more than a decade and also indicated for liver MRI (1). However, mangafodipir had to be administrated as a slow i.v. infusion over 15–20 min, which caused logistic difficulties and additional costs. This may explain why the contrast agent was withdrawn from the market in October 2003 in the US and in July 2010 in the EU (2).
If free manganese is administered i.v. or by another parenteral route it may result in serious side-effects specifically related to the central nervous system and the heart muscle (3, 4). Neurotoxicity has been documented in workers who have inhaled manganese containing dusts over a prolonged period of time and subsequently developed Parkinson-like signs and symptoms (3, 4). With regards to cardiotoxicity, manganese appears to affect the cardiac function by blocking calcium channels. However, experimental studies have shown that a relative high concentration of manganese is required (∼1 mM) to achieve this effect (4). In contrast, when manganese is administered orally it is exposed to a high first-pass effect in the liver, where it is taken up by the hepatocytes and subsequently actively excreted into the bile, thus resulting in only very small amounts of manganese reaching the systemic circulation (4). By combining the pharmacological knowledge about absorption of manganese from the intestine with the knowledge about the way the metal is “metabolized” in the liver, an oral manganese-based hepatobiliary specific MRI contrast agent has been developed (5, 6). The contrast agent is currently known as CMC-001 (CMC Contrast AB). In the last few years a number of articles have been published on the clinical performances of CMC-001 in relation to liver MRI (6–14). The aim of this review is to summarize the basic pharmacological and pharmaceutical aspects of this new oral hepatobiliary specific contrast agent.
Manganese
Manganese is one of the most abundant metals on earth and it is often found together with iron. It does not occur naturally in its pure form but as a component of more than 100 different minerals. Manganese can exist in 11 oxidative states, but in the most important biological compounds it is found as Mn2+, Mn4+, or Mn7+ (15). The diet represents the major source for the human intake and, apart from drinking water, amounts of up to approximately 45 mg/kg can be found in certain vegetables, nuts, grains, legumes, fruits, and products of these different sources. The normal daily dietary intake of manganese for an adult person is in the range of 2–10 mg/day depending on the type of diet (15).
Manganese is an essential trace element that is found in all tissues and it is required for lipid, carbohydrate, and protein metabolism. A number of different manganese metalloenzymes are involved with several organ systems and their functions, such as bone growth, immune function, digestion, regulation of blood glucose level and cellular energy, and the defence against free radicals (16). Together with vitamin K, manganese is also involved in blood coagulation (16). A relatively high concentration of manganese is found in the liver, which is mainly related to the biliary elimination and its role in the manganese homeostasis (4, 15).
After oral intake manganese is poorly absorbed from the intestine, normally only 2–5% of the ingested amount is taken up (16). The absorption from the intestine into the hepatic portal vein is negatively influenced by several factors such as the intake of dietary fibre, oxalic acids, phytic acids, and divalent cations such as Ca2+, Fe2+, and Mg2+. Tannins found in tea can also reduce the absorption of manganese (15). Magnesium-containing antacids and laxatives and the antibiotic medication tetracycline or tetracycline derivates also have a negative impact on the amount of manganese absorbed (17). Contrary, there are also factors promoting the absorption of manganese from the bowel, such as vitamin C, vitamin D3, and the non-polar amino acid alanine (5, 18).
Iron deficiency has also been described to be associated with increased absorption of manganese, and as a curiosity, there seems to be a gender-specific difference with men having a poorer absorption compared to women. The reduced absorption in men is probably due to their higher iron status and serum ferritin concentration (15, 16). When it comes to iron, there seems to be a competition with manganese in relation to the intestinal absorption, mediated via Divalent Metal Transporter 1 (DMT1), which may explain the mechanism behind the gender-specific difference (19).
After manganese has been absorbed from the intestine it is mainly bound to α2-macroglobulin and transported via the portal blood to the liver where it is taken up by the hepatocytes (20). Contrary to most other metals manganese is very efficiently filtered out by the liver and thereby prevented from reaching the systemic circulation. The first-pass effect for manganese has been estimated to be between 95% and 98% (21, 22). After the manganese has been taken up by the hepatocytes it is actively excreted into bile and subsequently into the intestine. Only a very small fraction of the dietary manganese reaches the main circulation, and the amounts excreted by the kidneys into the urine is negligible (14, 22, 23). As described above, the liver plays a central role in the manganese homeostasis, and a major impairment of its function may result in an increased systemic exposure and subsequent retention of the metal in the body (23).
Pharmaceutical formulation and administration
The pharmaceutical form of CMC-001 is powder for oral solution, which consists of two sachets. One sachet contains the active imaging substance in the form of 800 mg manganese (II) chloride tetrahydrate (MnCl2 . 4 H2O). The other sachet contains the absorption promoters, which are L-alanine 500 mg and vitamin D3 800 IU. These excipients in the CMC-001 formulation have been added in order to increase the absorption of manganese over the intestinal mucosa. The contents of the two sachets are mixed and diluted in a total of 200 mL of cold tap water and administered orally as a single dose after reconstitution. Before administration of the contrast agent the patient should have been fasting for approximately 6 to 8 h. The in-use stability of CMC-001 after reconstitution is 2 h (24).
Non-clinical pharmacology
In order to find the most optimal composition of CMC-001 a number of preclinical rat studies have been performed (5). A fixed amount of MnCl2 tetrahydrate (100 µmol/kg ∼ 19.8 mg/kg) together with varying amounts of L-alanine and vitamin D3 was given to 16 groups of rats that had been fasting for 18 h. Each group consisted of six animals. Three hours after administration of the test substances the rats were killed and the liver, kidneys, and heart were removed. The manganese content in these organs was subsequently measured by atomic absorption. These studies showed an increase in the liver content of manganese of 41% to 69% when the two absorption promoters were added to a formulation of MnC12 tetrahydrate compared to when it was given alone. Furthermore, and especially important for the safety of CMC-001, the manganese concentration in the kidneys from the rats that were given MnCl2 tetrahydrate plus the absorption promoters were within the range of the control animals. With regards to the heart, only one out of 16 groups of animals that were given MnCl2 tetrahydrate plus absorption promoters showed a statically significant increase in the manganese concentration. For the remaining groups the concentration was within the range of the control animals. No side-effects were observed in the animals that were exposed to CMC-001. From this series of experiments it was concluded that the addition of L-alanine and vitamin D3 increases the intestinal absorption of MnCl2 tetrahydrate (5). Moreover, from a safety perspective it was concluded that the high first-pass effect for manganese in the liver reduced the risk for potential systemic side-effects.
Clinical pharmacology
The pharmacokinetic aspects have been an important part of several of the clinical studies performed with CMC-001, where the absorption, distribution and excretion of manganese have been studied in detail (6, 7, 11–14). In a phase I study, CMC-001 was given to 12 healthy volunteers at dose levels corresponding to 800 mg or 1600 mg MnCl2 tetrahydrate and with six healthy volunteers allocated to each dose level. The enhancement of liver and gallbladder was evaluated at three different magnetic field strengths (0.23 T, 0.6 T, and 1.5T). MRI was performed in the time interval from 2.5 to 4.5 h after oral administration of CMC-001. In order to study the absorption of MnCl2 tetrahydrate blood samples were drawn at various time points from 0 to 24 h (6, 7). This phase I study showed that both dose levels significantly increased the relative signal intensity (SI) of the liver at T1-w imaging at all field strengths, indicating that a substantial amount of manganese had been transported from the intestine via the portal system to the liver. The highest increase in SI was observed with the 1600 mg dose at 1.5T (6, 7). This increase in SI was localized in the liver only, and no or negligible changes were observed post-contrast within the muscles and other organs such as the spleen and pancreas, underlining the target approach of CMC-001. The mean whole blood manganese concentration in the healthy volunteers pre-contrast was 203 nmol/L while the post-contrast mean values, averaged over all time points, was 168 nmol/L for the 800 mg dose and 156 nmol/L for the 1600 mg dose (7). The normal range for the whole blood manganese concentration has been reported as 100–271 nmol/L (25). In this study it was concluded that it is possible to increase the SI of the liver significantly by oral administration of CMC-001 in humans (6). Further, it was also shown that the whole blood manganese concentration was not affected by the intake of CMC-001(7).
In a phase II study the time course and dose-response relationship with regards to the relative liver SI enhancement after administration of CMC-001 were evaluated. Using a parallel randomized study design CMC-001 was administered in doses corresponding to 800 mg or 1600 mg MnCl2 tetrahydrate, respectively (11). A total of 20 patients with liver metastases were randomized. MRI was performed pre-contrast (at 0 h) and post-contrast at 1, 2, 3, and 6 h after administration of CMC-001 using a breath-hold T1-w gradient echo sequence (GRE) and a field strength of 1.5 T. The enhancement in signal intensity of the liver was plotted as a function of time after contrast media administration. The area under curve (AUC) was calculated in order to estimate the liver uptake and total signal enhancement. Blood sampling for measurement of whole blood manganese was performed pre-contrast (0 h) and 3 and 24 h after administration of the contrast agent. The study showed that the time course with regard to the relative liver SI enhancement for both dose groups continued to rise up to 3 h post-contrast administration where it reached its maximum of 55% in signal increase (median of pooled data from both dose groups) as shown in Fig. 1a. When the AUC for the 800 mg and 1600 mg doses were compared (Fig. 1b), no statistically significant difference could be detected (P = 1.00). Thus, oral administration of both the 800 mg and the 1600 mg dose resulted in similar relative liver SI enhancement, which may indicate that the liver had reached a kind of “saturation point”, where an increase in the dose of CMC-001 did not result in an increase of the SI enhancement. The study also demonstrated that CMC-001 offers a long diagnostic window ranging from 2 h until at least 6 h after administration with a relatively constant enhancement of liver SI, as shown in Fig. 1a.
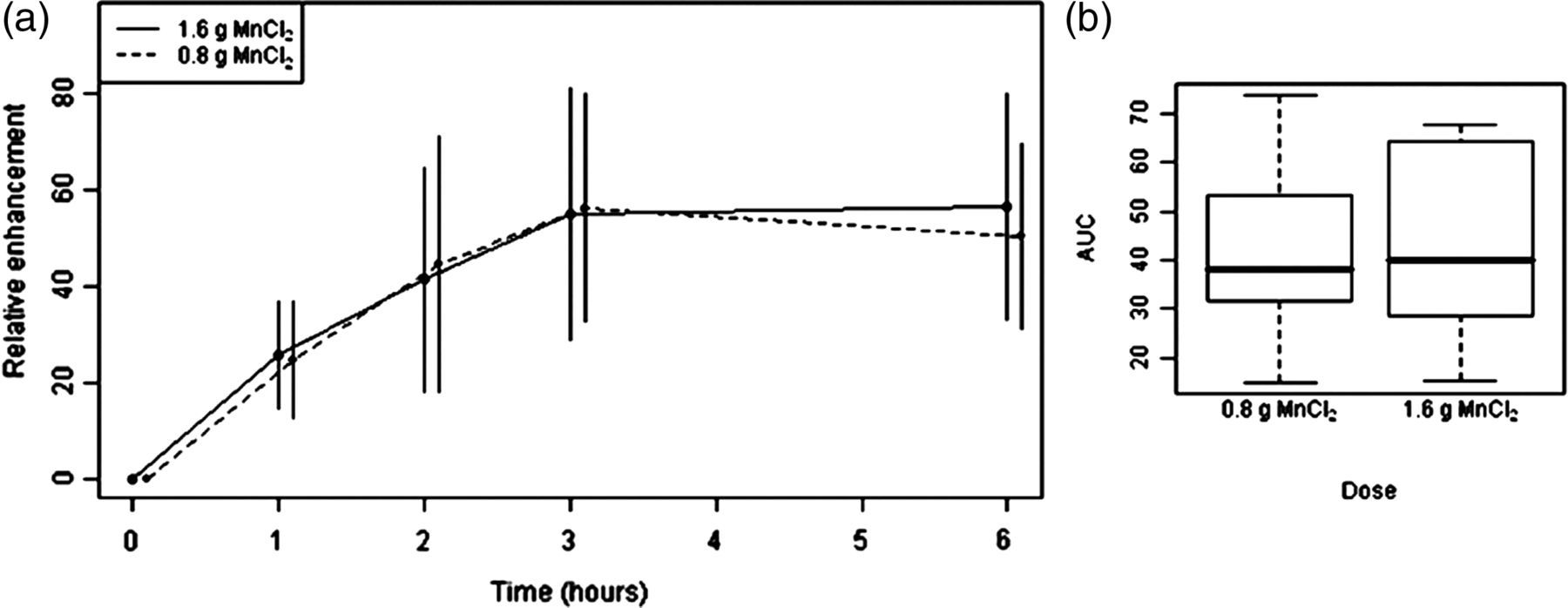
Time course of the relative liver SI enhancement after administration of CMC-001 at two different dose levels. (a) Time course of liver SI enhancement (%) after administration of 0.8 g and 1.6 g MnCl2 tetrahydrate (mean ± SD). (b) AUCs of liver SI enhancement after administration of 0.8 g and 1.6 g MnCl2 tetrahydrate. The AUCs were compared using Wilcoxon rank-sum test for independent samples (P = 1.00) (10). The figure is reprinted with permission from Investigative Radiology
The time course with regards to the active biliary excretion of manganese was also subject to investigation in the above described phase II study (11). As shown in Fig. 2 the excretion of manganese into the bile started early on after oral administration of CMC-001. Already 1 h post-contrast a noticeable increase in SI of the gallbladder was observed and it continued to increase until at least 3 h post-contrast. Despite this excretion a sufficiently high concentration of manganese was still present in the liver at 6 h after administration of CMC-001, with a relative increase in the liver SI enhancement of 47% compared to pre-contrast.

Axial T1-w GRE images from a patient with liver metastases after oral administration of CMC-001 (800 mg MnCl2 tetrahydrate). The images were acquired immediately before administration of CMC-001 (0 h) and 1, 2, 3, and 6 h after. The gallbladder is indicated by an arrow. The images were obtained at Department of Radiology, Charité – Universitätsmedizin Berlin, Berlin, Germany and previously unpublished
How long will the manganese concentration in the liver be elevated? This question was answered in another phase II study where 18 cancer patients with liver metastases were given a dose of CMC-001 corresponding to 1600 mg MnCl2 tetrahydrate (13). Liver MRI was performed pre-contrast (0 h) and 3 h post-contrast, and for five of the 18 patients an additional liver MRI was performed 24 h post-contrast. In this latter group of patients the liver SI enhancement had declined to below baseline, showing a normalized manganese concentration in less than 24 h after oral administration of CMC-001.
It has previously been reported in the literature that there is a gender-specific difference in the oral absorption of manganese (15, 16). Such a difference might have an impact when using CMC-001 for MR imaging of the liver with a potential need of gender-specific dosage. In most of the phase I and phase II studies conducted with CMC-001 measurements of whole blood manganese have been performed before and at several time points after the oral administration. Data are currently available from 162 administrations of CMC-001 to patients and healthy volunteers, representing 58 women and 104 men (6, 7, 11, 13, 14). When making a “meta-analysis” of the maximum concentration of manganese in whole blood obtained after administration of CMC-001 the mean concentration of manganese is 201.3 nmol/L (SD 66.6) in women and 200.0 nmol/L (SD 66.2) in men. Both mean values are well within the normal range for blood manganese, which is 100 to 271 nmol/L (25), and no statistically significant gender-specific difference in the manganese absorption after CMC-001 administration could be found (P = 0.47, Wilcoxon rank sum test stratified by dose level). A plausible explanation might be that the absorption promoters, L-alanine and vitamin D3, equalize the previously observed gender-specific differences in dietary manganese uptake.
The knowledge of the sensitivity and specificity of CMC-001 for liver IMR in relation to Gd-based contrast agents has so far been rather limited, and until now only one comparative phase II study has been conducted. The aim of this study was to compare the sensitivity of MRI to detect colorectal cancer liver metastases of CMC-001 and gadobenate dimeglumine (12). The study showed that CMC-001 and gadobenate dimeglumine had equally high sensitivity and both agents were able to detect liver metastases as small as 3 mm. However, the study also showed that the number of false-positive lesions was somewhat higher for CMC-001 compared to gadobenate dimeglumine, which is likely explained by the lack of a dynamic phase for CMC-001. The question about sensitivity and especially the specificity of CMC-001 will be further addressed in phase III studies.
As mentioned previously, manganese is taken up by the hepatocytes. However, when using mangafodipir, unexpected uptake has been described in tumors of non-hepatocyte origin. In one study on liver metastases from neuroendocrine tumors (carcinoids and pancreatic islet cell tumors) SI enhancement of variable degree was observed in all measured lesions, but significantly less than that of the surrounding liver parenchyma (26). In another study, uptake was observed in 8% (13/152) of non-hepatocellular tumors, of which 10 were malignant (metastases from colorectal, transition cell, and breast cancer and lymphoma) and three were benign (two hemangiomas and one cyst) (27). In a more recent study, no such paradoxical uptake of mangafodipir was observed (28). A paradoxical uptake is less likely to occur when using CMC-001. This is because CMC-001 is ingested and distributed to the liver via the portal system, while mangafodipir is infused and reaches the liver via the liver arteries too. Therefore, it is assumed that lesions lacking portal veins, or having predominantly arterial supply, will not be reached by CMC-001, thus resulting in a minimized risk of paradoxical uptake. However, this should be further monitored prospectively in a phase III clinical trial.
In a phase II study conducted recently the dose-response relationship for CMC-001 was evaluated with regards to image quality (14). The study was designed as a double-blind, randomized, cross-over study. Thirty-two healthy volunteers were enrolled and liver MRI was performed before and 3 h after oral administration of CMC-001 in doses corresponding to 200 mg, 400 mg, and 800 mg of MnCl2 tetrahydrate, respectively. The administration of the three different doses of CMC-001 was separated by a wash-out period of minimum 6 days. A pair-wise comparison showed that the three dose levels were significantly different with regards to the relative liver SI enhancement (P < 0.05) with an almost linearly relative increase in liver SI enhancement with the increase in dose (Fig. 3). The mean relative increase in liver SI was 19% for the 200 mg dose, 33% for the 400 mg dose, and 57% for the 800 mg dose. In this study it was concluded that the 800 mg dose provides the strongest liver SI enhancement and a statistically significantly better imaging quality compared to the 400 mg and 200 mg doses. A brief summary of the phase I and II studies described in relation to the clinical pharmacology of CMC-001 is given in Table 1.

Axial fat-saturated 3D gradient-echo T1w images from the same healthy volunteer after oral administration of CMC-001 in increasing doses (pre-contrast, 200 mg, 400 mg, and 800 mg). An increase in liver SI enhancement is clearly demonstrated with increasing dose of CMC-001. The images were obtained at Department of Radiology, Karolinska Insitutet, Karolinska University Hospital, Huddinge, Stockholm, Sweden and previously unpublished
Summary data of the phase I and II studies described in the article related to the clinical pharmacology of CMC-001
*Pooled data from both dose groups at 3 h
Safety of CMC-001
The evaluation of safety has been an important part of all the clinical studies conducted with CMC-001, which also includes the blood manganese concentration measurements in the patients and healthy volunteers pre- and post-contrast. The most frequent adverse events reported after oral administration of CMC-001 are: diarrhoea, nausea, and headache. The adverse events related to the gastrointestinal tract are probably caused by the hyperosmolar solution of CMC-001, resulting in fluid effusion to the intestine and a subsequent laxative effect. Nearly all of the adverse events reported were of mild intensity and all were transient. In the phase I and II studies that have been conducted the administered dose ranged from 200 mg to 1600 mg of MnCl2 tetrahydrate, and especially the adverse events related to the gastrointestinal tract showed to be dose dependent. For example, at the 1600 mg dose, diarrhea tended to be more commonly reported, to have a faster onset, and to be of higher intensity compared to the other dose groups. When it comes to adverse events related to the cardiovascular system, two cases of extrasystoles have been reported and one of these was judged by the investigators to be related to CMC-001. In total, 196 patients and healthy volunteers have been exposed to CMC-001 so far. No serious adverse events related to the administration of CMC-001 have been reported.
When analyzing the blood manganese concentration obtained in the different clinical studies, a small mean increase from baseline can be observed with a maximum at 3–4 h. After 24 h the mean values were almost back to baseline, but with a large interpatient variability. About 5–10% of the patients and healthy volunteers had baseline values close to or slightly above the upper limit of the normal range for blood manganese. These individuals continued to be close to or slightly above the normal range after administration of CMC-001, but their values decreased towards baseline at 24 h. When the concentration of manganese in blood was correlated to ECG values, blood pressure, and liver enzymes there was no statistically significant association. This indicates that there is no or very limited systemic interaction after administration of CMC-001 at doses of up to 1600 mg.
Based on the initial clinical safety experiences with CMC-001 from close to 200 patients and healthy volunteers it can be concluded that the adverse events are mainly localized to the gastrointestinal tract, and few systemic reactions have been reported. The latter may be explained by the high first-pass effect of manganese in the liver, which prevents a systemic exposure.
Conclusion and future perspectives
Manganese is one of the least toxic trace elements (29) and due to its favourable safety profile it may be an attractive alternative to the more toxic Gd (30, 31) based contrast agents in the future for patients undergoing an MRI evaluation for liver metastases. Because of the way manganese is “metabolized” by the human body it may even be an alternative in patients with renal insufficiency, as the non-clinical pharmacological studies seem to indicate (5). However, before recommending CMC-001 to patients with severely decreased kidney function, this hypothesis needs to be tested very carefully in well-controlled non-clinical and clinical studies.
Besides an advantageous safety profile, CMC-001 seems to offer favourable efficacy. There is a dual explanation. First, contrary to the hepatocytes most metastases do not take up manganese. Second, metastases only have arterial blood supply and lack portal vessels. Thus, manganese which is taken up from the portal venous blood after intestinal absorption only reaches the hepatocytes of the liver parenchyma but not the metastases. Both of these mechanisms result in a higher concentration of manganese in the healthy parenchyma compared to that of the malignant lesion. At MRI this will result in hypointense metastasis surrounded by hyperintense liver tissue as shown in Fig. 4.

Axial T1-w images of the liver of a 55-year-old woman with a colorectal liver metastasis (arrow) obtained at 1.5 T before (a) and after (b) administration of CMC-001(1600 mg MnCl2 tetrahydrate). The images were obtained at Department of Radiology, Karolinska Insitutet, Karolinska University Hospital, Huddinge, Stockholm, Sweden and previously unpublished
Based on the non-clinical and the clinical data available it can be concluded that the oral administration route of the manganese-based contrast agent CMC-001 offers advantages both with regards to safety and efficacy. CMC-001 will now enter the final clinical evaluation in phase III, where a larger number of patients with liver metastases will be exposed to the compound, and thus increase our knowledge of how to use this contrast agent in the most optimal way in the clinical setting.