
Abstract
Background
Benign regional lymph nodes (LNs) are sometimes enlarged in gastric cancer patients due to reactive or inflammatory changes. Frequently these enlarged LNs can mimic LN metastasis and lead to overstaging.
Purpose
To assess frequency of benign regional LNs in gastric cancer patients compared with that in a healthy population and to assess the frequency of benign regional LNs in gastric cancer according to T-staging.
Material and Methods
Between August 2005 and June 2009, 177 patients with surgically proven gastric cancer without LN metastasis (TanyN0M0) who had previously undergone preoperative multidetector row CT (MDCT) and 168 healthy patients who visited the healthcare center and underwent an abdominal MDCT were included in this retrospective study. An abdominal radiologist evaluated the distribution of regional LNs and measured the short diameter of LNs ≥6 mm, ≥8 mm, and ≥10 mm. The number of enlarged benign LNs was compared between the two groups, and the distribution of LN with regard to T-stage of gastric cancer was also evaluated.
Results
At least one LN ≥6 mm, ≥8 mm, and ≥10 mm was detected in 64.4% (114/177), 22.0% (39/177), and 4.0% (7/177) of patients in the gastric cancer group, respectively, compared to 29.8% (50/168), 4.2% (7/168), and 0% of patients in the healthy group, respectively. The difference between the two groups was statistically significant (P <0.0001). The LN ≥8 mm was found in 14.9% (20/134) in early gastric cancer (T1), and 44.2% (19/43) in advanced cancer (T2 or higher); the difference was statistically significant (P = 0.0002). However, the frequency of LN ≥6 mm in mucosal cancer (T1a) and submucosal cancer (T2b) was not significantly different, regardless of its size.
Conclusion
Benign regional LNs ≥6 mm are more frequently detected in gastric cancer patients than in a healthy population and in advanced gastric cancer than in early cancer.
Gastric cancer is the fourth most common cancer, and despite a decrease in incidence in recent decades, it is still the second leading cause of cancer-related deaths worldwide (1, 2). Lymph nodes (LN) are important prognostic indicators for gastric cancer with respect to long-term survival, and debate continues over the extent to which LN dissection should be carried out (2). Knowledge of LN status before treatment of gastric cancer would be important for predicting prognosis, as well as for determining the treatment strategy with respect to the extent of lymphadenectomy and selecting patients suitable for neoadjuvant chemotherapy (2, 3).
In multidetector row computed tomography (MDCT), nodal involvement in gastric cancer has been determined based on the size, CT attenuation values, and configuration of LNs (4, 5). Among those criteria, the size of the LN is currently most widely used for the diagnosis of LN metastasis in gastric cancer. Reported CT accuracies for N staging, however, are not that satisfactory, ranging only from 64–80% when a short axis diameter of a LN >8 mm was considered to be LN metastasis (6–9), 78% with a long axis diameter >8 mm (10), and 59–67% when LN > 6 mm was considered to be metastasis (8, 11). This poor diagnostic performance is mainly due to the high frequency of microscopic tumor involvement of small-sized LNs, which was reported to occur at a range of 21–55%, according to surgical data (12, 13). Another reason is the poor differentiation between reactive or inflammatory and metastatic nodal involvement. A histologic correlation study of LN in gastric cancer patients revealed that 59.2% and 47.5% of all LNs with a long axis diameter of 6–9 mm and 10 mm or greater, respectively, were tumor-free (13). While the small-sized LN metastasis raises the rate of false-negative diagnoses, reactive or inflammatory LN enlargement is attributed to an increased false-positive diagnosis, leading to overstaging. Of those two aspects affecting N stage performance, enlarged benign LNs are of interest in this study. Therefore, the purpose of the study was to assess benign regional LNs in gastric cancer and to compare them with those in a healthy population, as well as assessing benign regional LNs in gastric cancer according to T-staging.
Material and Methods
Patient population
This retrospective study was approved by the Institutional Review Board of our hospital, and patient informed consent was waived.
Gastric cancer patient group: By query of our institutional database, between August 2005 and June 2009, we identified 345 consecutive patients who underwent a surgical resection for histologically proven gastric cancer for the cancer patient group. Inclusion criteria were as follows: (a) patients who underwent curative surgery; (b) final pathologic staging revealing no regional LN metastasis irrespective of the depth of invasion of the primary tumor (TanyN0M0); and (c) patients who underwent preoperative contrast-enhanced abdominal MDCT. Two hundred and sixteen patients were selected according to these inclusion criteria, and among them, 39 patients were excluded due to: (a) the number of dissected LNs less than 15 (n = 20); (b) presence of synchronous extragastric malignancy (n = 2; ovarian cancer [n = 1], and rectal cancer [n = 1]); (c) the presence of benign acute or chronic extragastric disease (n = 11; chronic cholecystitis [n = 4], liver cirrhosis [n = 2], chronic liver disease [n = 2], acute calculous cholecystitis [n = 1], ureter stone [n = 1], distal common bile duct stone [n = 1]); (d) a past history of upper abdominal surgery (n = 5; cholecystectomy [n = 4], subtotal gastrectomy for gastric cancer [n = 1]); and (e) suboptimal image quality caused by severe motion artifact (n = 1). We included patients with at least 15 dissected nodes, according to the suggestions provided by the current American Joint Committee on Cancer/Union Internationale Contre le Cancer (AJCC/UICC), which states that a minimum of 15 LNs should be examined in order to achieve adequate predictive ability (1). Finally, 177 patients were included in our study (117 men and 60 women; mean age 59 years; age range 24–85 years).
Healthy population group: By query of our institutional database, between August 2005 and June 2009, we identified 193 consecutive patients who visited the health promotion center at our hospital for the purpose of a routine medical check-up and complaining of no severe symptoms, and underwent an abdominal contrast-enhanced MDCT; 175 patients underwent upper gastrointestinal endoscopy. Among the 193 patients identified, 25 were excluded because of: (a) incidentally detected malignancy (n = 7; early gastric cancer [n = 3], esophageal cancer [n = 1], duodenal cancer [n = 1], ovary cancer [n = 1], and breast cancer [n = 1]); (b) presence of active gastric or duodenal ulcer on endoscopy requiring medication (n = 6), presence of active or chronic benign extragastric intra-abdominal disease (n = 9; chronic hepatitis [n = 2], chronic calculous cholecystitis [n = 2], liver cirrhosis [n = 1], chronic pancreatitis [n = 1], acute appendicitis [n = 1], benign gastric ulcer [n = 1], tuberculous lymphadenitis [n = 1]); and (c) past history of upper abdominal surgery (n = 3; cholecystectomy [n = 2], subtotal gastrectomy [n = 1]). Finally, 168 patients were included in the healthy population group in our study (118 men and 50 women; mean age 53.9 years; age range 24–96 years). A flow chart of the study profile based on recommended standards for reporting diagnostic accuracy is presented in Fig. 1.
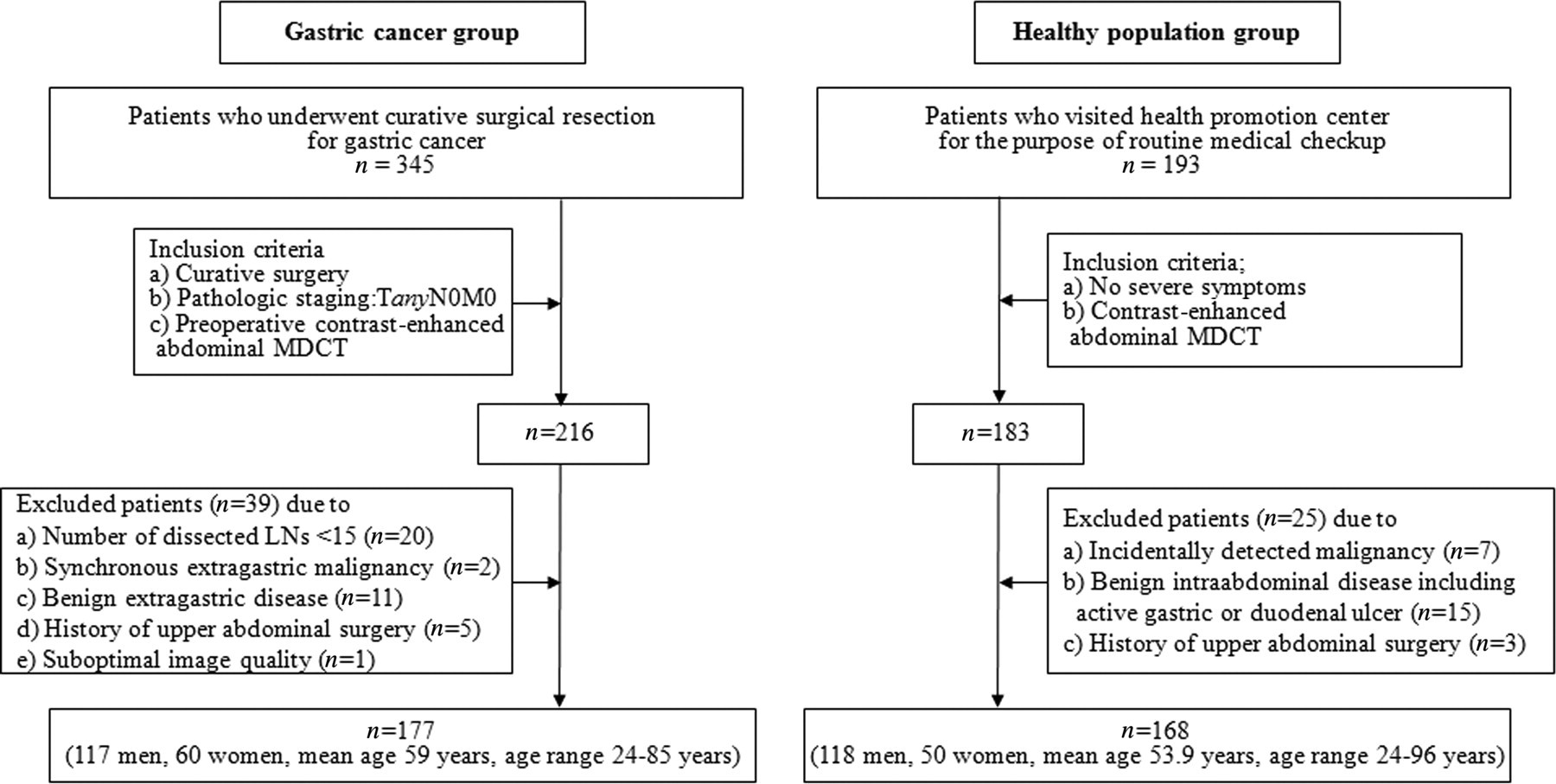
Flow chart of the study profile based on recommended standards for reporting the diagnostic accuracy
CT techniques
CT examinations were performed using one of three kinds of MDCT scanners: 64-(Somatom Definition, Siemens Medical Systems, Erlangen, Germany; LightSpeed VCT XT; GE Healthcare, Milwaukee, WI, USA); 16-(LightSpeed Pro 16; GE Healthcare, Milwaukee, WI, USA) channel CT. One hundred and thirty-two patients belonging to the gastric cancer group underwent a CT with a stomach protocol performed after the ingestion of an effervescent agent to obtain gastric luminal distension. CT included an unenhanced scan in the supine position, arterial phase scan in the right decubitus position for better visualization of gastric fundus, and a portal phase scan with a 30° left posterior oblique position for appropriate distension and preparation of the lower two-thirds of the stomach (14, 15). The remaining 45 patients in the gastric cancer group and all patients in the healthy population group underwent a general protocol abdominal CT, which included unenhanced and portal phase scans in the supine position.
Unenhanced scans were obtained, and then arterial and portal phase scans were followed with a 15-s delay after attenuation of the aorta at the thoracolumbar junction had reached 100 HU and a fixed 80-s delay, respectively, after the intravenous injection of 150 mL of iopromide (Ultravist 370; Bayer Schering Pharma, Berlin, Germany) administered at a rate of 3 mL/s with an autonomic injector. Images of unenhanced and portal phase scans were obtained from the level of the lower chest to the pelvic cavity, and those of the arterial phase scan were obtained from the lower chest to the iliac crest. The scan parameters had a detector collimation of 64 × 0.625 mm, beam pitch of 0.984, 120 kVp, automated dose modulation by using the maximum allowable tube current set at 200 mAs, and section thickness/reconstruction interval of 3 mm/3 mm (Somatom Definition scanner) or 3.75 mm/3.75 mm (LightSpeed VCT XT scanner) for the 64-channel CT scanner. The parameters for the LightSpeed Pro 16 scanner had a detector collimation of 16 × 1.25 mm, beam pitch of 0.938, 120 kV, 200 mAs, and a section thickness/reconstruction interval of 3.75 mm/3.75 mm.
Image analysis
All CT images were retrospectively reviewed on a picture archiving and communication system (PACS) workstation monitor (Centricity® RA1000, GE Healthcare, Milwaukee, WI, USA), by two attending radiologists (HSP and YJK, with 4 and 8 years of clinical experience in abdominal radiology, respectively). The observers determined the presence, location, and the number of regional LNs according to the Japanese LN classification (16) by consensus, using transverse and coronal reconstructed CT images. Next, one of the two observers (HSP) measured a short diameter of the regional LNs on maximally magnified transverse CT images on the PACS monitor using an electronic caliper. The caliper showed the diameter of each LN to two decimal places. The measurement was performed three times for each LN and the three measured values were averaged to minimize the measurement error. The order of image analysis was randomly mixed in the two patient groups. We considered a regional LN as significantly enlarged when the size of the short diameter, measured on CT, was ≥6 mm, which is the lowest cut-off value adopted by earlier reports on nodal staging of gastric cancer with MDCT (8, 11). When there were greater than six enlarged lymph nodes, the largest six lymph nodes were measured and recorded.
Statistical analysis
The frequency of patients with enlarged regional LNs in the two patient groups were counted by applying cut-off values of 6 mm, 8 mm, and 10 mm, and were compared among the two patient groups using Fisher's exact test. The distribution of LNs according to the depth of the primary tumor invasion in the cancer patient group was assessed, and a comparison was made between early gastric cancer (T1) versus advanced gastric cancer (T2 or higher), and mucosal cancer (T1a) versus submucosal cancer (T1b), using Fisher's exact test. The mean size of the enlarged LNs were calculated and compared between the cancer and healthy groups, early and advanced cancer groups, and mucosal and submucosal cancer groups, by way of a Student's t-test. A P value less than 0.05 was considered to indicate statistical significance. Results of the statistical analysis were obtained using commercially available software (MedCalc, version 10.1.0.0; MedCalc Software, Mariakierke, Belgium).
Results
Surgical and pathologic findings in cancer patient group
Curative surgery was performed on all patients in the cancer group (subtotal gastrectomy [n = 155, including one patient who underwent laparoscopic surgery], total gastrectomy [n = 16], proximal gastrectomy [n = 2], and pylorus-preserving gastrectomy [n = 4]). The distributions of the depth of invasion for the tumors were: T1 in 134 patients (T1a, n = 86; T1b, n = 48) (134/177, 75.7%); T2 in 36 patients (20.3%); T3 in seven patients (4.0%); and no patients with T4 (0%).
A regional lymphadenectomy was performed for all patients in the group in conjunction with the gastrectomy. The number of dissected LNs ranged from 15 to 132 (mean ± standard deviation 39 ± 17.85).
MDCT findings of regional benign lymph nodes
In the gastric cancer group, a total of 210 enlarged (≥6 mm) regional LNs were detected in 114 (64.4%) patients. The mean size and standard deviation of the enlarged LNs was 7.26 ± 1.29 mm. The most frequent location of the enlarged LNs was the lesser curvature (n = 75), followed by left gastric (n = 50), common hepatic artery (n = 47), and others (n = 34). The number of enlarged LNs ≥ 6 mm was only one in 52 patients, two in 44 patients, three in 10 patients, as well as four and six in four patients, respectively. Further, the number of enlarged LNs ≥8 mm was 49 in 39 (22.0%) patients compared to LNs ≥10 mm was 11 in seven (4.0%) patients in the cancer group (Table 1).
Comparison of benign regional lymph nodes (LNs) between the gastric cancer and healthy population groups
*Numbers express mean ± standard deviation
†Fisher's exact test
‡Student t-test
N/A, not applicable
In the healthy population group, 61 enlarged LNs ≥ 6 mm were found in 50 (29.8%) patients, with a mean LN size of 7.01 ± 0.9 mm. The distribution of the location of the enlarged LNs was a similar distribution in the cancer group: lesser curvature (n = 20), common hepatic artery (n = 12), left gastric (n = 11), and others (n = 18). Forty-two patients had only one enlarged LN, while seven patients had two enlarged LNs and one patient had three enlarged LNs. Eight enlarged LNs ≥ 8 mm were found in seven (4.2%) patients, and no patients had enlarged benign LNs ≥ 10 mm in the healthy population group (Table 1).
Comparison of regional benign lymph nodes in the two patient groups
On a per patient basis, LNs ≥6 mm in size were more frequently detected in the cancer group than in the healthy population group (P = 0.0001). Likewise, LNs ≥8 mm and LNs ≥10 mm in size were also more frequent in the cancer group than the healthy group (P = 0.0001 and P = 0.0149, respectively). However, the mean sizes of all enlarged LNs between the two groups were not significantly different (P = 0.1634). The results of this statistical analysis are shown in Table 1, and a scatterplot showing the LNs according to their size distribution in the two groups is displayed in Fig. 2. Also, representative cases showing regional benign LNs in a gastric cancer patient and a healthy patient are displayed in Figs. 3 and 4, respectively.
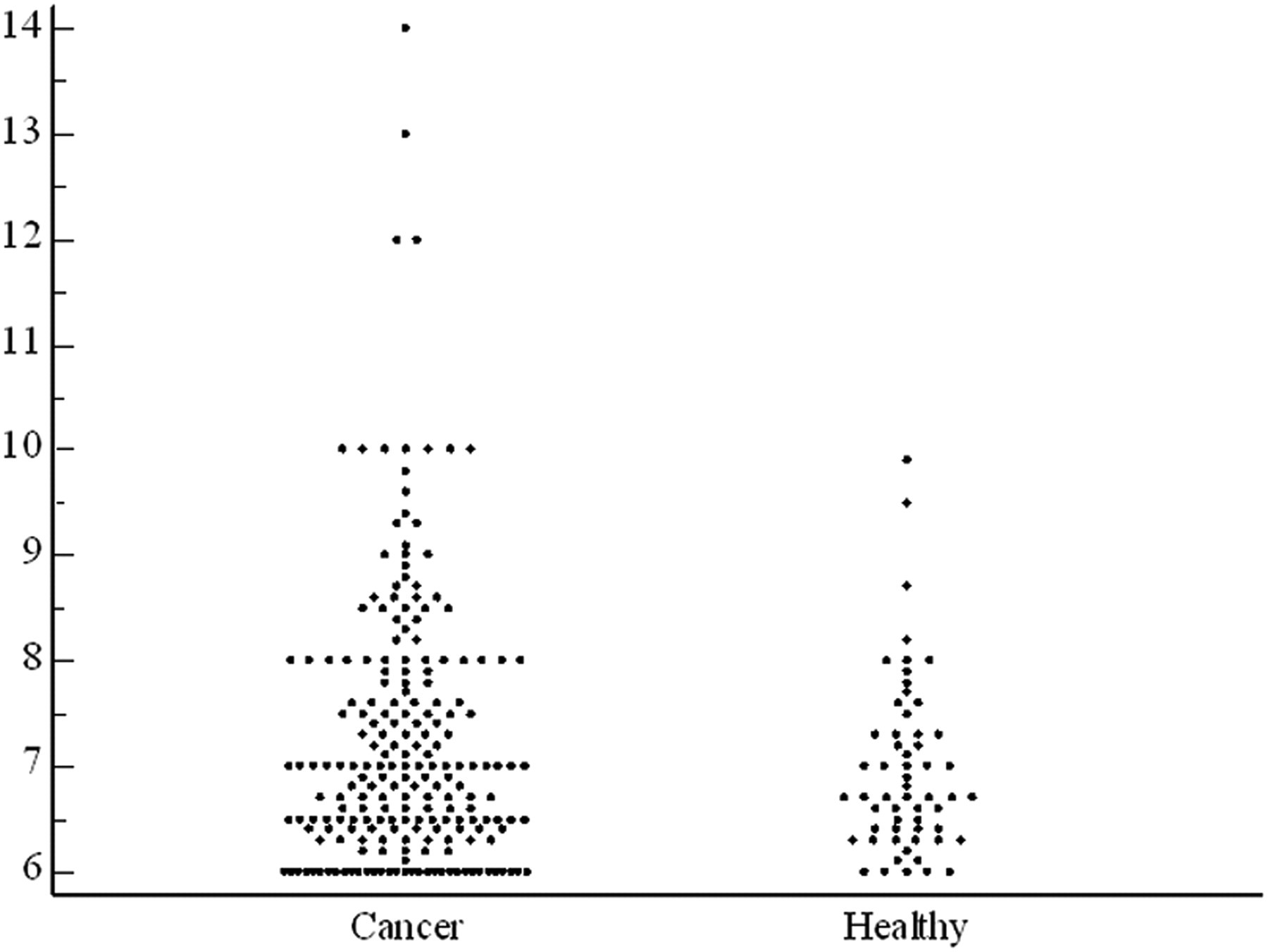
Scatterplot showing the distribution of benign regional LNs ≥ 6 mm in the gastric cancer and healthy population groups. Numbers in the vertical axis of the graph indicate millimeters of LNs

A 52-year-old man with advanced gastric cancer (T2N0M0). The contrast-enhanced CT performed in the right anterior oblique position shows multiple enlarged LNs at the left gastric (arrowhead) and the lesser curvature (arrows). The short diameter of the left gastric LN is 14 mm and those of the lesser curvature measured 10 mm and 8 mm
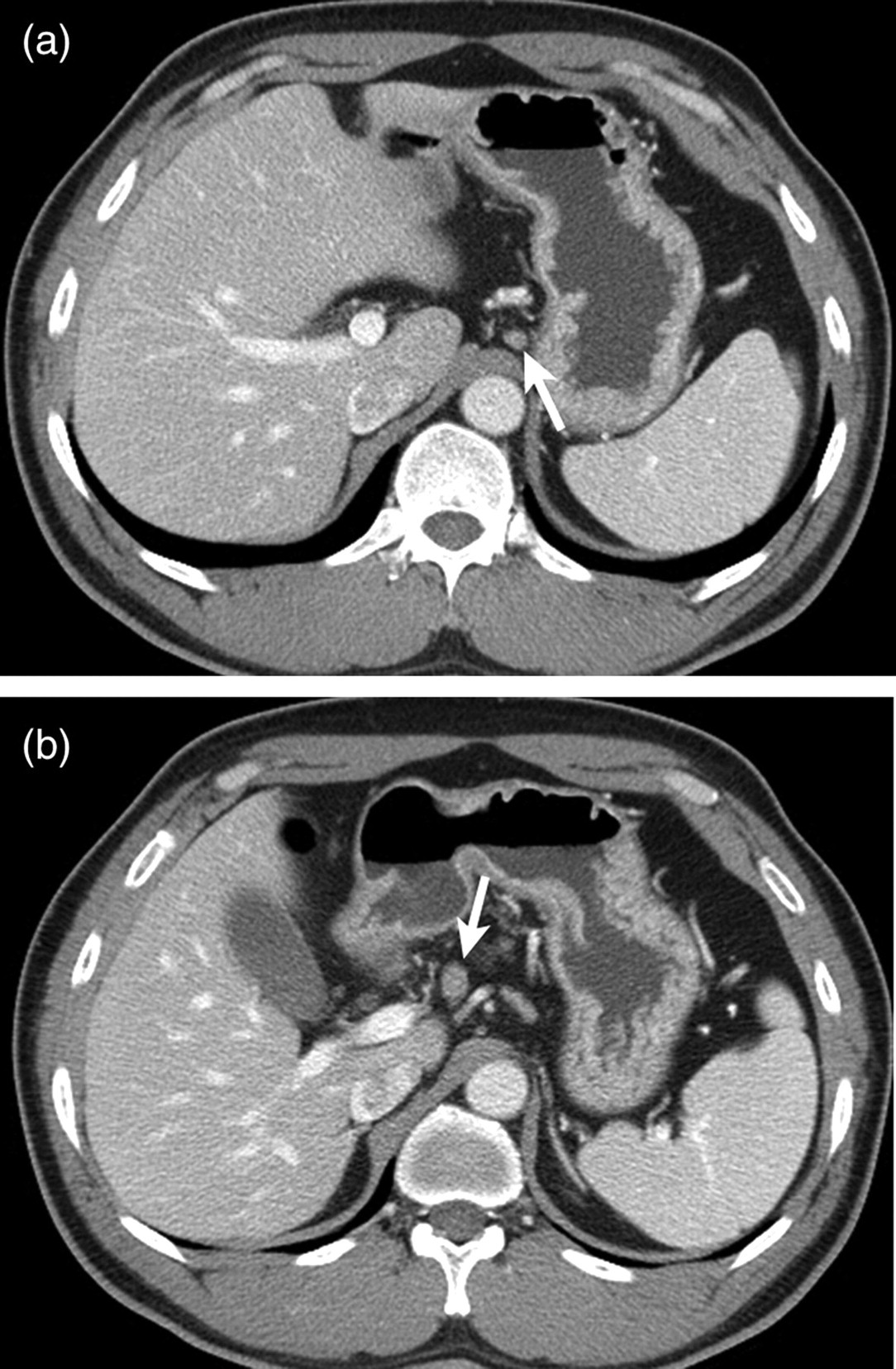
A 46-year-old man who presented for a routine check-up. (a) Contrast-enhanced CT scan shows an enlarged benign left gastric LN with its short diameter measuring 6.3 mm (arrow). (b) An additional caudal scan reveals a benign common hepatic artery LN with a 9.5 mm diameter (arrow)
Comparison of regional benign lymph nodes with regard to the T-stage of the gastric cancer group
When the LNs ≥6 mm were compared in the patients with early cancer (T1; 82/134, 61.2%), and those of advanced cancer (T2 or higher; 33/43, 76.7%), the difference was not statistically significant (P = 0.0687). However, a LN ≥ 8 mm was significantly more frequent in patients with advanced cancer (19/43, 44.1%), than in those with early cancer (20/134, 22.0%) (P = 0.0002). The frequency of LNs ≥10 mm was not significantly different between patients in the early cancer groups (P = 0.3629) (Table 2). The mean size of all benign enlarged LNs in early cancer was 7.03 ± 1.08 mm and that of advanced cancer was 7.66 ± 1.51 mm; the difference was statistically significant (P = 0.0006).
Comparison of benign regional lymph nodes (LNs) between the early gastric cancer and advanced gastric cancer groups
*Numbers express mean ± standard deviation
†Fisher's exact test
‡Student t-test
N/A, not applicable
When the mucosal (T1a, n = 86) and submucosal cancer groups (T1b, n = 48) were compared, the frequency of the enlarged LNs, regardless of its size, did not find a significant difference between the two groups (P = 0.6179–1.0000). The mean size of LNs between the two groups was also not found to be statistically significant (T1a, 6.94 ± 0.98 mm; T1b, 7.21 ± 1.25 mm, P = 0.1874) (Table 3).
Comparison of benign regional lymph nodes between the mucosal cancer (T1a) and submucosal cancer (T1b) groups
*Numbers express mean ± standard deviation
†Fisher's exact test
‡Student t-test
N/A, not applicable
Discussion
Our study results have demonstrated that benign regional LNs with a clinically relevant size are significantly more frequently observed in gastric cancer patients relative to asymptomatic healthy patients. As referenced by several previous studies on gastric cancer staging on CT, overstaging of LN status on a size-based diagnosis was reported to range from 11% to 47.5% (4, 7, 17). In line with the results of those reports, enlarged benign LNs in gastric cancer patients in our study consequentially led to overstaging of gastric cancer.
The exact mechanism for benign LN enlargement is not clear. Lesion-by-lesion histopathologic correlation of each benign LN was not performed in this study. But in general, the pathology of the LNs is known as reactive hyperplasia or inflammatory infiltration (5). One of the possible explanations for our result is the links between cancer and inflammation, on a molecular and cellular basis. Much evidence based on epidemiological studies of patients or molecular studies of animals, have led to a general acceptance that inflammation and cancer are linked (18–21). According to those reports, cancer cells generate an inflammatory microenvironment in tumors for which there is no underlying inflammatory condition by activating inflammatory mediators (19). Even though those reports deal with the inflammatory microenvironment of the tumor itself, rather than inflammatory LNs, we assume that cancer-induced inflammation is also likely to affect regional LNs.
On the contrary, another possible explanation for inflammatory diseases is the increase in risk of developing many types of cancer. Since Virchow proposed that chronic inflammation promotes carcinogenesis, accumulating studies support the hypothesis that chronic inflammations increase the risk of cancer development (18–21). Microbial infections, autoimmune disease, and inflammatory conditions of unknown origin are recognized as triggers of chronic inflammation related with cancer development, as well as the association of Helicobacter pylori (H. pylori) with gastric cancer and gastric mucosal lymphoma (18, 19, 22). Because a detailed histology of dissected regional LNs other than absence of tumor involvement is not obtained in this study, information as to the infection with H. pylori of the resected gastric specimens or regional LNs in gastric cancer patients is not available. However, considering the high prevalence of H. pylori infection in the Korean adult population (59.6%) and the significantly high incidence of H. pylori in a gastric cancer patient compared with the control group (23), inflammatory regional LNs in gastric cancer are thought to be related to H. pylori gastritis due to its omnipresence.
Our study also showed that enlarged benign regional LNs were more common in advanced gastric cancer than in early cancer. Considering the theory of the cancer-inflammation relationship which was described above, this result is predictable because the higher the tumor stage, the higher the chance that the tumor promotes inflammation will be. With advances in the endoscopic techniques, endoscopic mucosal resection or endoscopic submucosal dissection has become first line treatments for EGC without evidence of LN metastasis (24, 25). Conventionally, endoscopic resection for EGC was not indicated in the case of undifferentiated or signet ring cell histology, size of lesion larger than 2 cm, submucosal involvement of tumor, and endoscopic findings of ulceration that have lymphovascular invasion (26, 27). However, according to the extended criteria for endoscopic resection of EGC which was recently proposed in Japan, indications are expanded to the EGC lesion of large size, lesion having ulceration, lesion with undifferentiated or signet ring cell pathology, or lesion with submucosal layer invasion (less than 500 µm) (26, 28). Consequently significance of accurate N-staging in EGC is becoming higher for the decision of treatment strategy. A previous study of EGC on MDCT revealed approximately 6% of the overstaging rate in the diagnosis of LN metastasis based on its diameter (29).
As for EGC, our assumption was that tumor involving the submucosal layer is more likely to engage in regional LNs compared with those involving the mucosal layer, and therefore showing a higher frequency of benign enlarged LNs, since lymphatics are located in the submucosal layer of the stomach. However, the result was against our expectation and the frequency of enlarged benign regional LNs was not significantly different between mucosal (T1a) and submucosal (T1b) cancer. Only the mean size of the LNs was slightly larger in the submucosal cancer group, without statistical significance.
Our study has several limitations to be monitored; first, owing to its retrospective nature, a histopathologic analysis with lesion-by-lesion matching of each LN was not feasible. Exact radiologic–pathologic correlation is practically almost impossible if benign and metastatic regional LNs are intermixed. Therefore, only patients in the N0 stage were included in the cancer patient group; hence, a selection bias was inevitable. Also, we presume that benign regional LNs are enlarged mainly due to inflammation, but histologic evidence inflammation is not available in this study and differentiation of inflammation and reactive hyperplasia was also not possible. Future prospective studies with full histologic examinations, including the presence of H pylori infection, the dissected benign LNs in cancer patients seems to be necessary. Second, this study may be half-completed in terms of N staging because it dealt with only the aspect of false-positive diagnosis. The other arm regarding the false-negative aspect, which is about small-sized metastatic LNs, is not available. Furthermore, studies on the distribution and frequency of benign enlarged LNs regarding N stage and T stage in gastric cancer patients must be of interest. Third, MDCT protocols in the study population are not homogeneous because some of CT scans in the gastric cancer patients group were performed with maximal gastric distension and in the decubitus position. We agree that different scan positions or gastric distension status may affect the size measurement of regional LNs, especially those abutting the gastric wall. However, those measurement errors may not significantly influence the overall study results.
In conclusion, benign regional LNs ≥6 mm are more frequently detected in gastric cancer patients than in healthy populations, and more frequent in patients with advanced cancer than those with early cancer. Therefore, in the N staging of gastric cancer, these enlarged benign LNs may lead radiologists to overstage the disease.
Footnotes
ACKNOWLEDGEMENTS
This paper was supported by Konkuk University in 2009.