
Abstract
Background
Adenoma malignum, also known as minimal deviation adenocarcinoma, is a subtype of mucinous adenocarcinoma of the cervix.
Purpose
To evaluate the clinical, pathologic, and imaging features of the adenoma malignum of the uterine cervix.
Material and Methods
We retrospectively analyzed the CT and MRI findings in 13 patients: size, endoluminal fluid, appearance of the solid and cystic component, margin, enhancement, characteristics of locules of the cystic lesion, tumor spread, and associated ovarian lesion. Clinical and pathologic features were determined in 24 patients.
Results
The mean of the major tumor diameter was 4.1 cm (range, 2.2-6.5 cm). In the imaging features, 77% of 13 tumors demonstrated endoluminal fluid. All tumors showed enhancing solid components; 62% were multicystic and 38% had solid lesions. Most solid lesions exhibited an irregular margin (80%). The locules of the multicystic lesions tended to have smooth margins (75%), to have an average major diameter of ≤1 cm (88%), and to be 11 -20 in number (75%). The solid lesions were associated with invasion and metastases (60%). Clinically, 38% of 24 patients had watery discharge and 13% had Peutz-Jeghers syndrome, while pathologically, most patients were low stage (I or II) (83%). Over the 2-year follow-up of 17 patients, 82% was free from disease. The patients with more aggressive tumors or an unfavorable prognosis that manifested as tumor recurrence or metastasis tended to have invasion, watery discharges, high stages (III or IV) (100%) and solid lesions, metastases, and associated ovarian lesions (67%).
Conclusion
Awareness of imaging features as well as clinicopathologic manifestations of adenoma malignum can aid in accurate diagnosis, treatment, and prediction of prognosis.
Adenoma malignum, also known as minimal deviation adenocarcinoma, is a subtype of mucinous adenocarcinoma of the cervix (1–4). The prevalence is very low, accounting for only about 1.3% of cervical adenocarcinomas (5, 6). Adenoma malignum is often associated with Peutz-Jeghers syndrome and mucinous tumors of the ovary (1–4). The most common initial symptom is watery vaginal discharge (1–4). Reports of the prognosis for patients with adenoma malignum have not provided uniform data. Several studies have reported a poor prognosis (7–9), whereas other studies found a relatively favorable prognosis similar to that of other well-differentiated cervical adenocarcinomas (5, 10).
The imaging features characteristic of adenoma malignum, especially as seen in magnetic resonance imaging (MRI), are multicystic lesions with solid components that extend from the endocervical glands to the deep cervical stroma. The characteristic MRI findings of adenoma malignum may be useful in the early diagnosis (1–4). However, in recent years, there have been reports describing benign glandular lesions, which are often histologically and radiologically confused with adenoma malignum (11–14). In cases where cysts are microscopic or few in number, the lesions may be recognized as solid (1, 15).
The aim of this study was to evaluate the imaging features of adenoma malignum and correlate them with the clinical and pathological features. Furthermore, to determine whether the imaging features could be used to predict a more aggressive versus a less aggressive form of adenoma malignum based on histological characteristics.
Material and Methods
Our study was approved by the institutional review board. However, as this study was a clinical and mainly retrospective study, informed consent was not required by our institutional review board.
Patient population
A computerized search was conducted to identify cases of surgically confirmed adenoma malignum between January 1996 to December 2010 at three institutions, which revealed 24 cases. Each patient's medical records, including clinical and pathological data, were reviewed retrospectively (24 patients) and prospectively (17 patients, evaluated follow-up data more than 2 years, to May 2011). Of these 24 adenoma malignum patients, 13 preoperative imaging studies were available. Six computed tomography (CT) scans and nine MRIs were available, while two patients had both CT and MRI. Eleven enhanced imaging studies had been performed (six CT scans and seven MRIs). All imaging was performed within 2 weeks prior to initial treatment (surgery, radiation therapy, or chemotherapy). The mean patient age was 43.17 years (age range, 30–59 years).
CT and MR examination
The CT examinations were performed using a single-detector row helical CT scanner (Somaton Plus-S; Siemens Medical Systems, Erlangen, Germany) in four patients. Multidetector row helical CT scanners (Light Speed QX/I; GE Healthcare Milwaukee, WI, USA) were used for the remaining two patients. Intravenous contrast material (Iopamiro 300 [iopamidol]; Bracco, Milan, Italy or Ultravist 300 [iopromide]; Bayer Schering Pharma AG, Berlin, Germany) was administered into the antecubital vein using a power injector at a dose of 2 mL/kg to a maximum dose of 160 mL at a rate of 3.0 mL/s. The scan delay for contrast-enhanced scanning was 100–120 s for single-detector row helical CT scanning and 90–100 s for multidetector row helical CT scanning. Scan coverage was from the diaphragmatic dome to the ischial tuberosities.
The scanning parameters for single-detector row helical CT were: section collimation, 7 mm; pitch, 1.5; table speed, 7.5 mm per rotation (10 mm/s); reconstruction interval, 5 mm; and an X-ray tube voltage of 120 kV and a tube current of 210 mA were used. For multidetector row helical CT, a section collimation of 5 mm × 4, a beam pitch of 1.5, a reconstruction interval of 5 mm, an X-ray tube voltage of 120 kV, and a tube current of 210-240 mA were used.
MRI was performed using a 1.5-T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany, Signa; GE Healthcare, Milwaukee, WI, USA, Archiva; Philips Medical System, Best, The Netherlands). In nine patients, T1-weighted spin-echo images using a body or pelvic array coil (TR range/TE range, 400-600/ 8-11; section thickness, 5-7 mm; intersection gap, 1-3 mm; field of view, 32 cm; number of acquisitions, 2; and matrix, 256 × 256) were obtained from the renal hila to the femoral neck. Axial, sagittal, and coronal T2-weighted fast spin-echo images using a body or pelvic array coil (TR range/TE range, 3500-4500/100-120; echotrain length, 8; section thickness, 4 mm; intersection gap, 1-2 mm; field of view, 32 cm; number of acquisition, 3; and matrix, 256 × 256) were obtained. In two patients, axial, sagittal, and coronal T2-weighted fast spin-echo images using an endovaginal coil (3500-4500/100-120; echotrain length, 8; section thickness, 4 mm; intersection gap, 1 mm; field of view, 15 cm; number of acquisition, 3; and matrix, 512 × 512) were obtained. In seven patients, after a rapid bolus intravenous injection of gadopentetate dimeglumine (Magnevist; Bayer Schering Pharma AG, Berlin, Germany), axial and sagittal T1-weighted fast spin-echo images were obtained.
Imaging features analysis
Three radiologists evaluated the imaging features by agreement. We retrospectively analyzed the CT and MRI findings in 13 patients, focusing on well-known, typical multicystic lesions and atypical solid lesions for the following morphologic features: size, presence of endoluminal fluid, appearance of the composition of the solid component, margin, enhancement, characteristics of the locules of the cystic lesion, local tumor spread (invasion into the vagina, parametrium/parametria, and adjacent organs), as well as distant tumor spread (metastases including lymphadenopthy) and associated ovarian lesion.
The lesion size was assessed as the major tumor diameter among the three dimensions. We divided the lesion size into two groups (>4cm or ≤4cm). The presence of endoluminal fluid was judged to be positive when there was any visible fluid within the endometrial cavity, vagina, or fallopian tubes. We classified appearance by semi-quantitative assessment of the amount of solid components as predominantly solid, mixed solid and cystic, or predominantly cystic. A predominantly solid mass was indicated when the tumor was composed of more than 80% solid components and a predominantly cystic mass was indicated when the tumor was composed of more than 80% of cystic components. The margin of the lesions was evaluated as smooth or irregular, and enhancement of solid components including septa within the lesion was evaluated as present or not. We evaluated the following characteristics of locules of the cystic lesion: average major diameter of locules of the cystic lesion (≤1 cm or >1 cm), number of locules of the cystic lesion (≤10 or 11-20), and signal intensity of locular fluid on T1-weighted MRI (low or high).
Lymphadenopathy was considered to be present when the short diameter of a lymph node was >1 cm or when three or more lymph nodes were conglomerated. We classified the associated ovarian lesions as benign or malignant by features suggestive of malignancy including a thick, irregular wall; thick septa; papillary projections; a large soft tissue component; necrosis (16).
Clinical features analysis
We retrospectively analyzed the clinical features in 24 patients, focusing on typical symptoms or signs such as watery discharge or signs of Peutz-Jeghers syndrome. We also evaluated treatment methods (surgery and radiation therapy) and neo- or postadjuvant therapy (none, radiation therapy, and/or chemotherapy). We retrospectively and prospectively evaluated more than 2 years of follow-up data in 17 patients and classified patients as being disease-free or having tumor recurrence or metastasis.
Pathologic features analysis
After surgery, the resected specimens were examined and reviewed. The imaging features were correlated with the surgical and pathologic features based on the medical records with regard to tumor morphology, invasion, and metastasis on gross and microscopic assessment. The tumor stage and the associated ovarian lesion were evaluated as well. Fifteen of the patients underwent a radical hysterectomy with pelvic and paraaortic lymph node dissection with the specimens evaluated using the TNM staging system, all 24 of the patients including seven patients underwent a simple hysterectomy or two patients underwent a biopsy with specimens evaluated using the FIGO staging system (17, 18).
Results
Imaging features
The imaging features are summarized in Table 1. The mean of the major tumor diameter was 4.1 cm (range, 2.2-6.5 cm). The major diameter was >4 cm in seven patients (54%) and ≤4 cm in six patients (46%). Ten (77%) tumors showed the presence of endoluminal fluid.
Imaging features analysis of adenoma malignum (n = 13)
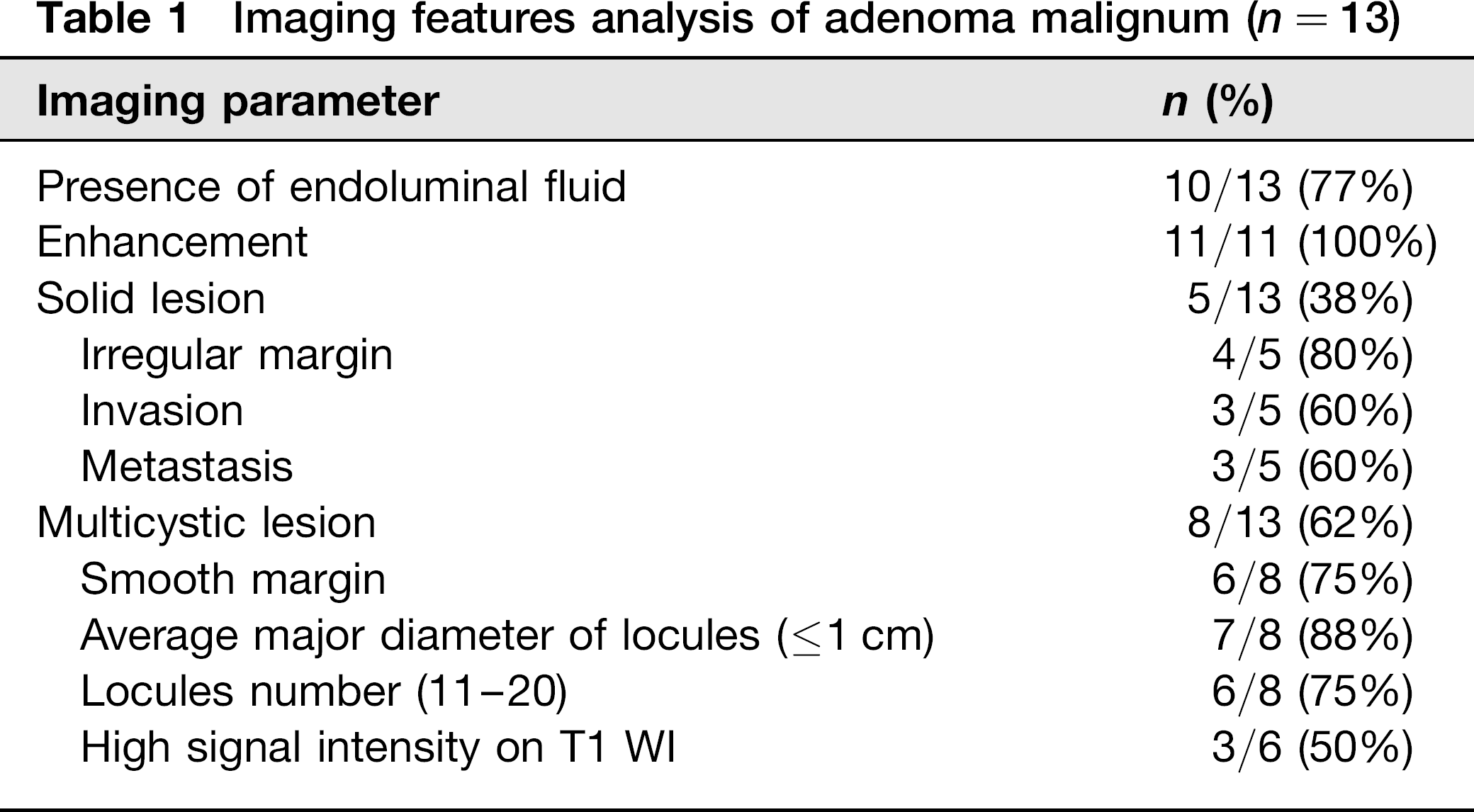
In terms of appearance, eight (62%) of 13 tumors showed up as multicystic lesions: four were predominantly cystic (Fig. 1), four mixed solid and cystic (Fig. 2), and the remaining five (38%) appeared as solid lesions (predominantly solid) (Fig. 3). All tumors showed enhancement (100%, 11/11). The most solid lesions exhibited an irregular margin (80%, 4/5). The locules of the multicystic lesions tended to have a smooth margin (75%, 6/8), have an average major diameter of ≤1cm (88%, 7/8), and were from 11 to 20 in number (75%, 6/8). Three multicystic lesions demonstrated high signal intensity on T1-weighted MRI (50%, 3/6).
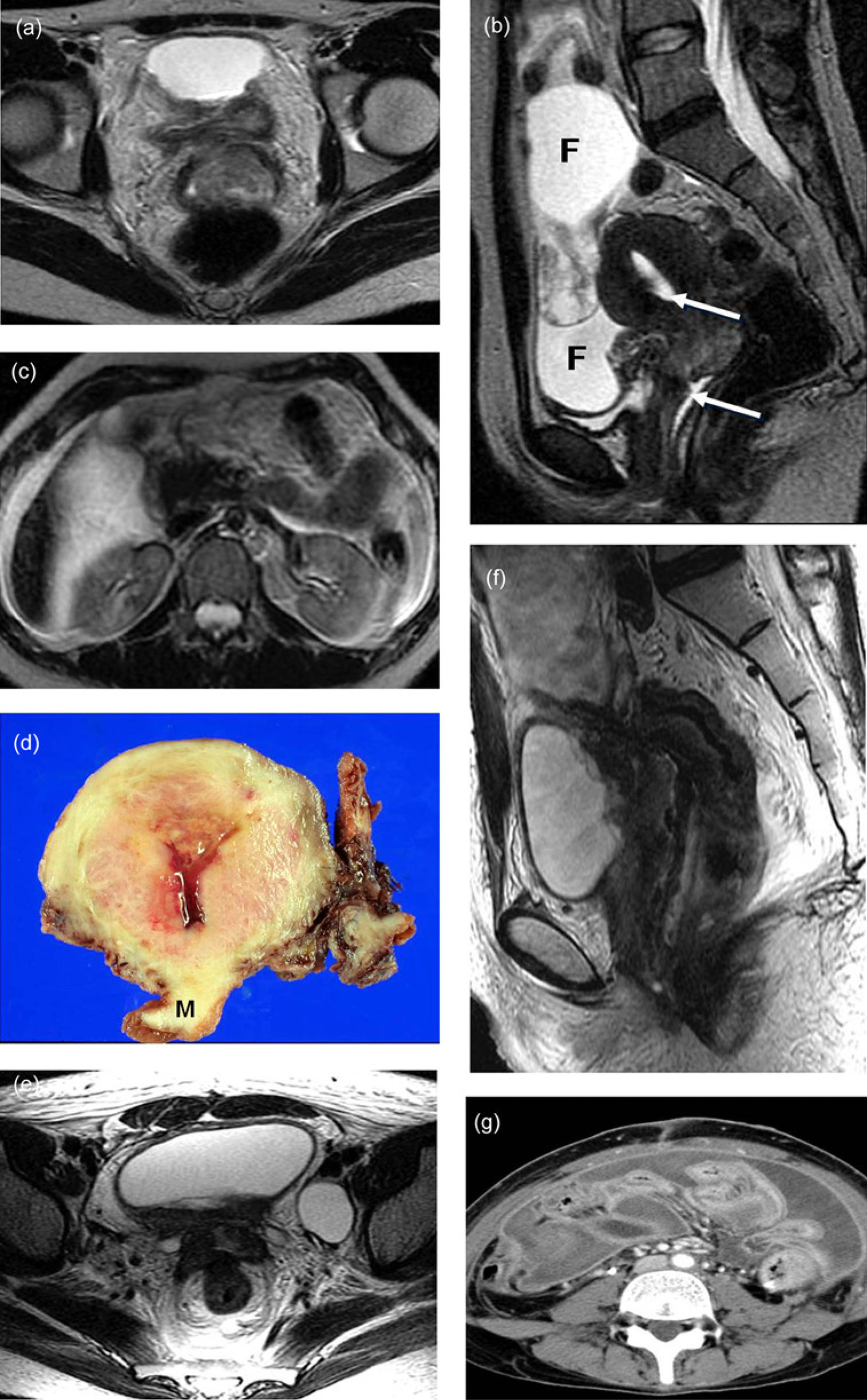
A 30-year-old woman with adenoma malignum in the uterine cervix and Peutz-Jeghers syndrome. Axial (a) and sagittal (b) T2-weighted MRIs show high signal intensity multicystic lesions within the enlarged uterine cervix. (c) Axial T1-weighted MRI shows high signal intensity fluid of the multicystic lesions within the enlarged uterine cervix. (d) Enhanced T1-weighted axial MRI shows an enhancing septa or solid component. (e) Photograph of the gross specimen via hysterectomy shows multicystic lesions (M) within the diffuse enlarged uterine cervix and cervical involvement of tumor cells. (f) Microphotograph shows multicystic lesions composed of a single layer of columnar cells that resemble normal endocervical glands. However, most glands have an irregular shape, cellular atypia, and structural dysplasia with multiple lobulations demonstrating a “hair-pin” shape (H & E stain, original magnification, x40) A 48-year-old woman with adenoma malignum in the uterine cervix with watery vaginal discharge. (a) Enhanced CT scan shows multicystic lesions with enhancing septa within an enlarged uterine cervix. (b) Axial T2-weighted MRI shows high signal intensity multicystic lesions within the enlarged uterine cervix. (c) Contrast medium enhanced T1-weighted axial and (d) subtraction MRIs show enhancing septa or solid component (arrows) A 38-year-old woman with adenoma malignum with watery vaginal discharge. Axial (a) and sagittal (b) T2-weighted MRIs show high signal intensity solid lesions within the enlarged uterine cervix. Presence of endoluminal fluid (arrows) in the endometrial cavity and vagina are also noted. A large amount of peritoneal free fluid collection (F) surrounding the ovary is evident. (c) Axial T2-weighted MRI at the renal hilar levels shows a large amount of free fluid collection, suggesting peritoneal metastases. Bilateral irregular septated cystic ovarian lesions and free fluid collections along both ovaries are also noted (not shown). (d) Photograph of the gross specimen via hysterectomy shows solid masses (M) within the diffuse enlarged uterine cervix and cervical involvement of tumor cells. Microphotograph shows the same features seen in Fig. 1f: a multicystic lesion composed of a single layer of columnar cells that resemble normal endocervical glands with irregular shape, cellular atypia, and structural dysplasia (not shown). Axial (e) and sagittal (f) T2-weighted MRIs at 6 months show tumor recurrence with invasion to the bladder and rectum. (g) Axial CT scan after another 2 months shows peritoneal metastases

Four (30%) of 13 tumors showed vaginal invasion and one (8%) showed parametrial and bladder invasion. Three (23%) of 13 tumors showed both ovarian and peritoneal metastases. One (8%) showed lymph node metastasis. Three (23%) of 13 tumors had associated ovarian lesions. Solid tumors were associated with invasion (3/5, 60%) and metastases (3/5, 60%).
In five patients, the tumor had invaded the vagina; CT and MRI detected the vaginal infiltration in four of these patients. In two patients, the tumor had infiltrated the parametria and in one, the tumor also infiltrated into the bladder. CT and MRI detected parametrial and bladder infiltration in one of these patients. In three patients, the tumor had metastasized. CT and MRI correctly diagnosed metastasis in all of these patients.
Clinical features
Clinical features are summarized in Table 2.
Clinical and pathologic features analysis of adenoma malignum (n = 24)
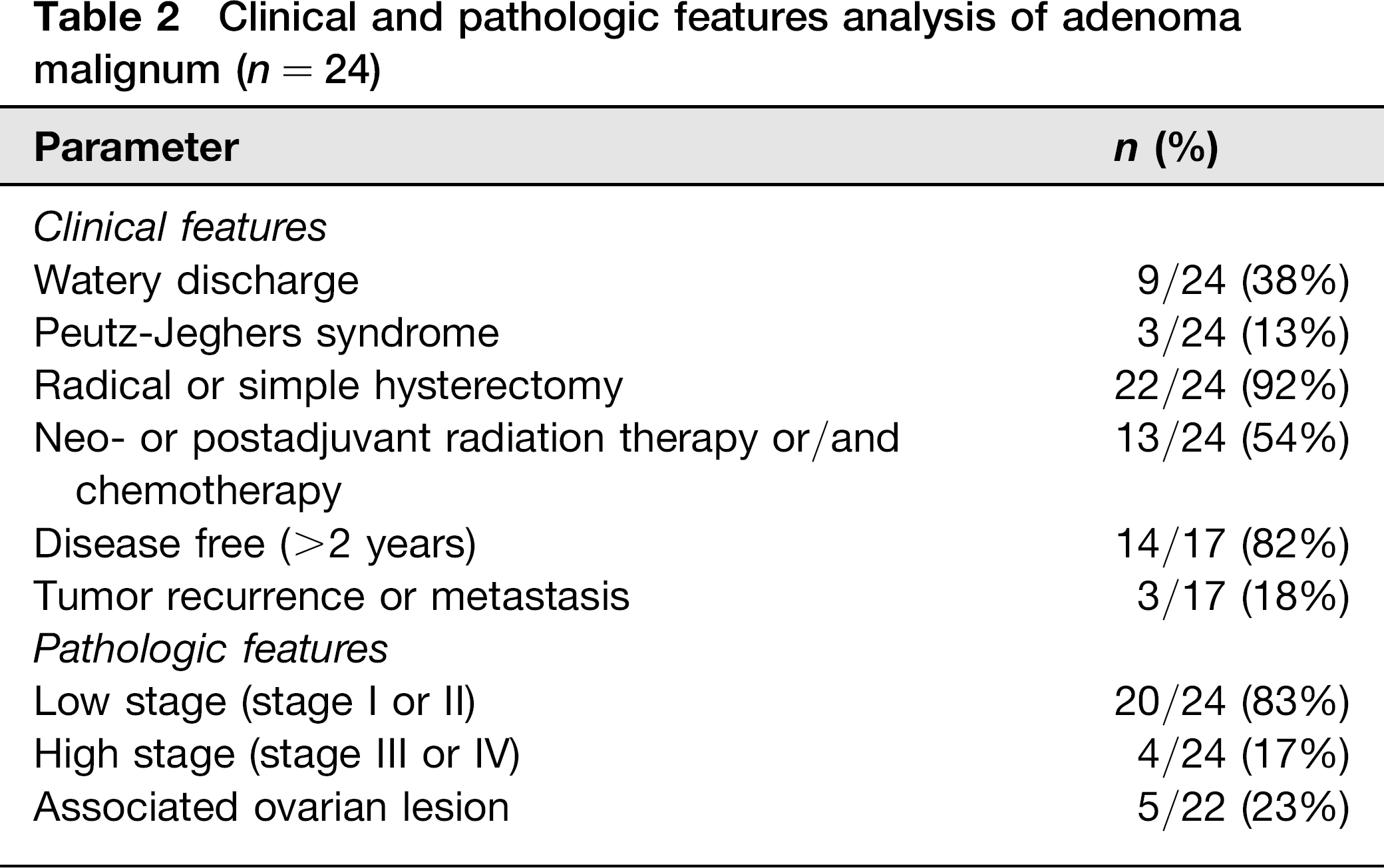
On review of the clinical features, nine (38%) of the 24 patients had watery discharge, three (13%) had Peutz-Jeghers syndrome and one patient both. The remaining patients had non-specific clinical presentations including abdominal pain in eight patients, vaginal bleeding in three patients, and an abnormal Papanicolaou test (Pap smear) result in two patients. Radical (15 patients) or simple (seven patients) hysterectomy was performed in 22 (92%) of the 24 patients. The remaining two (8%) patients received radiation therapy after histopathologic proof by biopsy. Thirteen (54%) of 24 patients had neo- or postadjuvant radiation therapy and/or chemotherapy. Over the 2-year follow-up, 14 (82%) of 17 patients were disease-free and the remaining three (18%) patients manifested a tumor recurrence or metastasis.
Pathologic features
Pathological features are summarized in Table 2. Multicystic tumors (mixed solid and cystic, and predominantly cystic lesions) appeared grossly as multilocular cystic lesions on CT and MRI. Microscopic evaluation revealed lesions mainly composed of well-differentiated endocervical glands that extended from the surface to the deeper portion of the cervix. Pathological analysis demonstrated conjugation of small cystic spaces lined predominantly by mucincontaining columnar epithelial cells with the cystic spaces filled with mucin. The interstitial space was composed of normal cervical stroma, which was often edematous (Fig. 1). However, predominantly solid lesions in CT and MRI appeared grossly as solid lesions (Fig. 3). Microscopic evaluation revealed the same features seen in multicystic lesions. The predominantly solid lesions differed, however, in that very few dilated glands were recognized in the cases with non-cystic appearance (Fig. 3).
Eighteen patients were diagnosed as stage I, two patients as stage II, one patient as stage III, and three patients as stage IV disease. Most patients were low (stage I or II) stage (83%, 20/24). Five (23%) of the 22 patients that underwent surgery had associated invasions: three vaginal invasions, one vaginal and parametrial invasion, and one vaginal, parametrial, and bladder invasion. Five (23%) of the 22 patients that underwent surgery had associated ovarian lesions: three metastases, one bilateral borderline mucinous tumor, and one mucinous cystadenoma.
Possible prognosis prediction
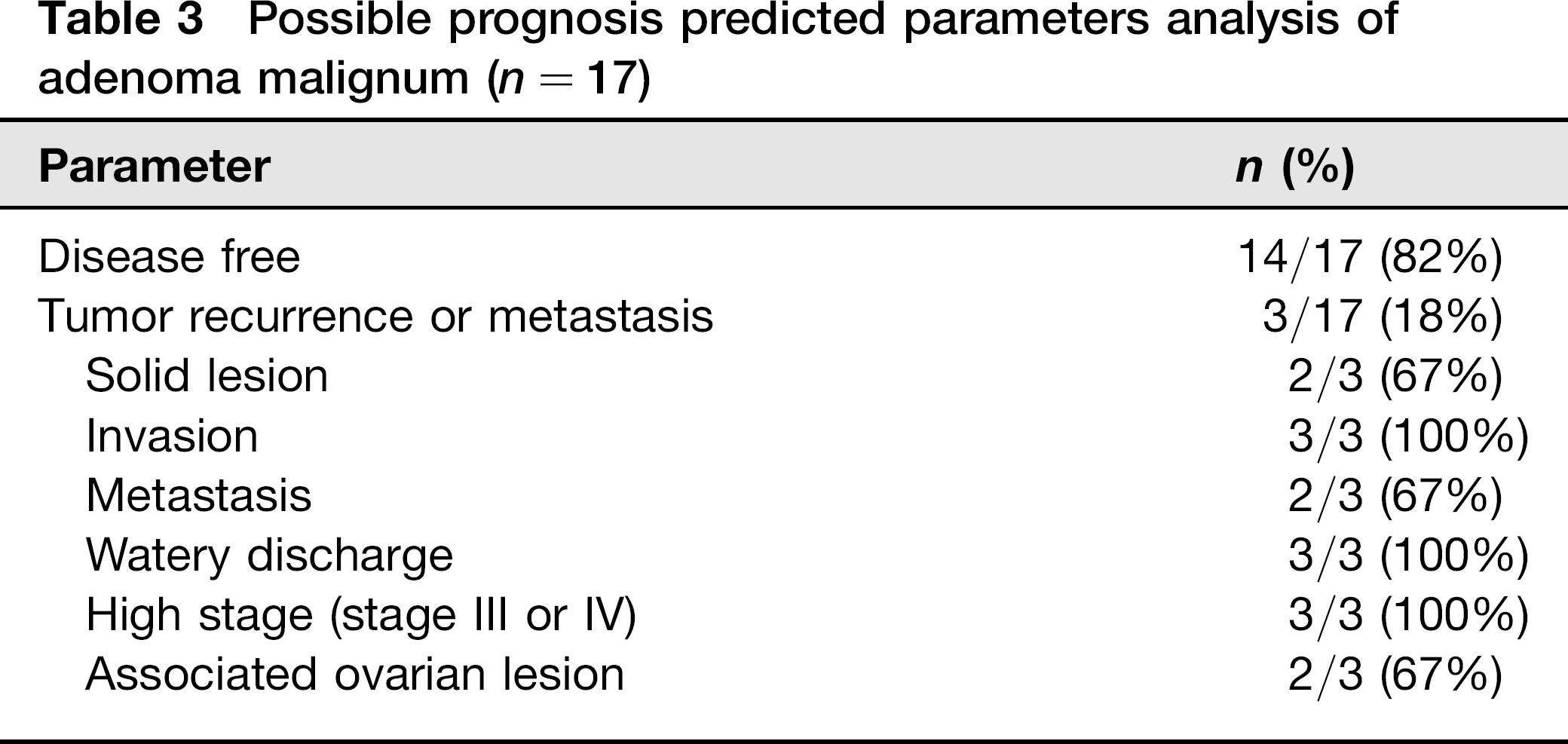
Possible prognosis predictions are summarized in Table 3. The patients with more aggressive tumors or an unfavorable prognosis that manifested as tumor recurrence or metastasis tended to have solid cervical lesions (2/3, 67%), invasions (3/3, 100%), metastases (2/3, 67%), watery discharges (3/3, 100%), high stages (3/3, 100%), and associated ovarian lesions (2/3, 67%).
Possible prognosis predicted parameters analysis of adenoma malignum (n = 17)
Discussion
The presence on imaging studies of a multicystic lesion that invades the deep cervical stroma and contains solid components may suggest malignancy. There appears to be a continuous spectrum from hyperplasia to high-grade malignancy based on the percentage of solid components within a lesion (11, 19). In contrast, benign lesions do not generally deeply invade the cervical stroma, are of small size with well-defined margins, and do not contain solid components (1, 2, 11).
However, in recent years there have been many reports describing benign glandular lesions, including uterine cervicitis, tunnel cluster, deep endocervical glands, deep nabothian cysts, lobular endocervical glandular hyperplasia, metaplasias, endometriosis, and infectious and reactive atypias, that were confused histologically and radiologically with malignant adenoma malignum. The important differential point on pathology is that true adenoma malignum invariably contains atypical cells that are usually located deep in the cervical stroma (20). Although reliable differentiation between malignant and benign cystic lesions and their differential diagnosis remains problematic, imaging features may give clues for diagnosis of adenoma malignum. In our study, all tumors showed enhancement within the mass (100%, 11/11) and 10 (77%) of 13 tumors demonstrated the presence of fluid within the endometrial cavity, vagina, or fallopian tubes. The role of the radiologist is to ensure the identification of a broad spectrum of multi-lcystic lesions in the uterine cervix and to possibly differentiate malignant from benign lesions using either imaging or clinical features (or both) to prevent unnecessary radical surgery before histopathologic proof of malignancy (11).
Adenoma malignum is a representative of malignant multicystic lesions in the uterine cervix. Although it has been reported that a multicystic lesion with some solid components in the deep cervical stroma seen upon imaging is evidence of adenoma malignum, there have been few studies about solid appearing adenoma malignum. A previous study by Ito (15) reported that non-cystic fine villous lesions were detected mostly on T2-weighted MRI. Another study by Takatsu (20) reported that predominantly solid parts in tumor, often associated with various-sized cystic structures, were detected mostly on T2-weighted MRI. In our study, five (38%) of 13 tumors had predominantly solid lesions, but no lesion was a fine villous lesion. These results indicated that adenoma malignum would not always reveal a multicystic feature.
Ultrasonography (US) remains the method of choice in the initial evaluation of suspect uterine cervical lesions because it is non-invasive, inexpensive, and widely available. MRI can be used as a problem-solving tool (21). MRI is the ideal modality for visualization of the uterine cervix due to its superior soft tissue contrast. It accurately depicts the cervical stroma, endocervical canal, and paracervical structures. The multiplanar capability of MRI allows tailoring of the image plane to follow the orientation of the cervix and to optimally visualize the relationship of the cervix to surrounding organs and structures. MRI can play a pivotal role in the staging and preoperative evaluation of uterine cervical cancers (22). CT is not generally advocated as the first-line imaging modality. However, multidetector row helical CT allows improved visualization and diagnostic accuracy (21, 23).
CT and MRI may be feasible for the evaluation of local or distant tumor spread as well as primary tumors. In our study, CT and MRI detected four (80%) of five vaginal invasions, one (50%) of two parametrial invasions, and three (100%) of three ovarian or peritoneal metastases. All missed cases were performed by single-detector row helical CT scan. Thus, such evaluations would be more accurate using MRI or multidetector row helical CT scan.
Although controversial, an unfavorable prognosis has been reported for adenoma malignum. As detection is technically difficult, the tumors disseminate into the peritoneal cavity even in the early stage of the disease, and the response to radiation or chemotherapy is poor (7–9). In our study, the prognosis was favorable. Over a 2-year follow-up, 14 (82%) of 17 patients were disease-free. Patients with an unfavorable prognoses with tumor recurrence or metastases tended to have solid cervical lesions (2/3, 67%), invasions (3/3, 100%), metastases (2/3, 67%), watery discharges (3/3, 100%), high stages (3/3, 100%), and associated ovarian lesions (2/3, 67%). We presume that the unfavorable prognosis of the early reports may be the result of inadequate therapy and higher malignancy potentials.
There are limitations to our study. First, our study was a retrospective consensus review. Thus, we can not determine several parameters accurately. Second, our study included a relatively small number of patients with available preoperative CT and MRI with adenoma malignum. This small number may not accurately reflect the full spectrum of imaging features of these tumors. For instance, we determined the parameters for unfavorable prognosis from only three patients. Third, there was no comparative analysis of the imaging findings between adenoma malignum and other benign glandular lesions. Fourth, CT of the uterine cervix may not be optimal. However, CT evaluation of adenoma malignum has been shown to be acceptable in a study by Ito (15) and particularly in the larger multicystic cases in our study. CT was also useful in the assessment of distant disease (Fig. 3g). Fifth, we established non-homogeneous and uniform criteria so as to combine patients with and without imaging studies, and with and without enhanced studies. We also collected data over a 14-year period and three institutions, so there were variations in the CT and MRI parameters and the facilities used, such as single- or multidetector, pelvic array or endovaginal coil.
Nonetheless, we believe that our study is a useful contribution. First, to our knowledge, there have been few studies of the imaging, clinical, and pathologic features of adenoma malignum. Furthermore, previous studies did evaluate imaging, clinical and pathologic features separately. Our study analyzed and correlated imaging, clinical, and pathologic features. Second, our study also evaluated prognosis, which was correlated with imaging, clinical, and pathologic features. Furthermore, our study population (n = 24) was the second largest group compared to previous studies (1, 5–10, 15). Third, we analyzed solid-appearing adenoma malignum as well as multicystic lesions.
In conclusion, adenoma malignum exhibits solid as well as multicystic lesions. Although the prognosis of adenoma malignum patients was relatively favorable, patients with an unfavorable prognosis tended to have solid cervical lesions, invasion, metastases, watery discharges, higher stages, and associated ovarian lesions. Awareness of the imaging features as well as clinicopathologic manifestations of adenoma malignum can aid in accurate diagnosis, treatment, and prediction of prognosis.
Footnotes
Acknowledgements
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science of Technology (grant number 2012-0003944). The authors would like to thank