
Abstract
Background
Anterior talofibular ligament (ATFL) injury is a commonly seen sports-related injury and a major underlying pathology of chronic ankle instability. However, it is difficult to accurately identify chronic injury of the ATFL.
Purpose
To investigate the value of ultrasound (US) examination in identifying chronic ATFL injury.
Material and Methods
We evaluated 83 consecutive patients who underwent US examination for diagnosis of the ATFL injury and subsequent ankle arthroscopy. The arthroscopic findings were used as the reference standard.
Results
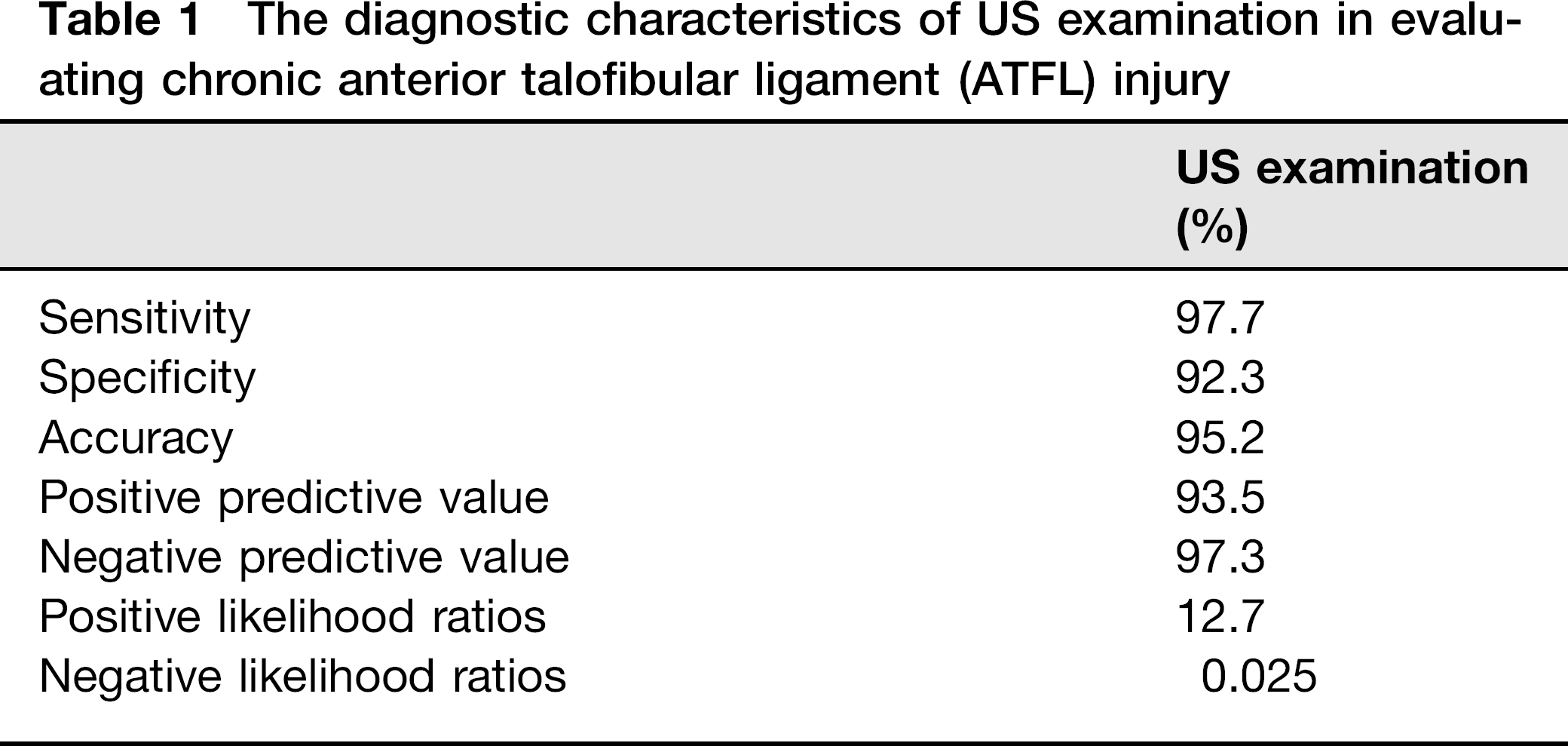
Forty-four patients were found to have ATFL injury on arthroscopy. The accuracy of US examination for the detection of ATFL injury was 95.2%, with sensitivity of 97.7%, specificity of 92.3%, positive predictive value of 93.5%, negative predictive value of 97.3%, positive likelihood ratio of 12.7, and negative likelihood ratio of 0.025.
Conclusion
US examination is a reliable and accurate method to evaluate chronic ATFL injury.
Chronic ankle instability (CAI) is a commonly seen sports-related injury in the clinic. One of the major underlying pathologies of CAI is injury of the anterior talofibular ligament (ATFL), which may require surgical intervention as part of the strategy to reconstruct the ankle stability (1).
Until now, it remains difficult to identify chronic injury of the ATFL accurately. The majority of surgeons make a diagnosis based on the symptoms and physical examination findings. However, this method has high variability as it depends on the experience of the doctor and has been reported to have a high misdiagnosis rate (2).
Ultrasound (US) examination is generally accepted to be a sensitive method for identification injuries of ligaments and other soft tissues (3), and has been used as an accurate and reliable method for evaluating acute injuries of the ATFL (2). However, the usefulness of US examination for detection of chronic ATFL injury is not well understood. The aim of this prospective study was to investigate the value of US examination in identifying chronic ATFL injury, compared with arthroscopy findings.
Material and Methods
Subjects
A total of 83 consecutive patients underwent ankle arthroscopy during September 2009 to September 2010. The study group comprised 51 men and 32 women, with a mean age of 32.2 years (range, 17–57 years). The preoperative clinical diagnosis was: (i) chronic ankle instability, 37 cases; (ii) loose body, six cases; (iii) impingement syndrome, including anterior bony impingement and anterior soft tissue impingement, 42 cases; (iv) osteochondral lesions (OCL), 11 cases; (v) arthritis, including infectious arthritis, reactive arthritis, traumatic arthritis, and osteoarthritis, 18 cases; (vi) synovial chondromatosis, one case; (vii) frozen ankle, three cases; and (viii) chronic syndesmotic injury, six cases.
The study had ethical approval from the Human Ethics Research Board of our hospital.
US examination
All the patients agreed to US examination before the surgery. All US examinations were performed by a senior radiologist (the second author) who has 15 years of experience in musculoskeletal US. An ALT HDI 5000 US unit (Philips Medical Systems, Bothell, WA, USA) was used. The radiologist was blinded to the diagnosis or other examination findings of the patients.
Patients were in a supine position with the ankle passively placed in a maximal inversion and plantar flexion position. A wide frequency linear array transducer with center frequencies from 5 to 17 MHz was used. The transducer was placed over the lateral side of the ankle with coupling gel and moved slightly around the tip of the lateral malleolus to find the ATFL. The transducer was positioned along the long axis of the ATFL to examine the whole ligament, and was then rotated 90° to show the short axis of the ATFL. The ATFL of the contralateral side was also examined. The ligament was showed as a thin, anisotropic, hyperechoic, rectilinear band at the long axis, and as a small ovoid structure filled with uniform hyperechoic dots at the short axis (4). Scar tissue was showed as a uniform hyperechoic area, and the joint capsule was showed as an anisotropic cross-arrangement band with a moderate to strong signal (but a weaker signal than the ligaments).
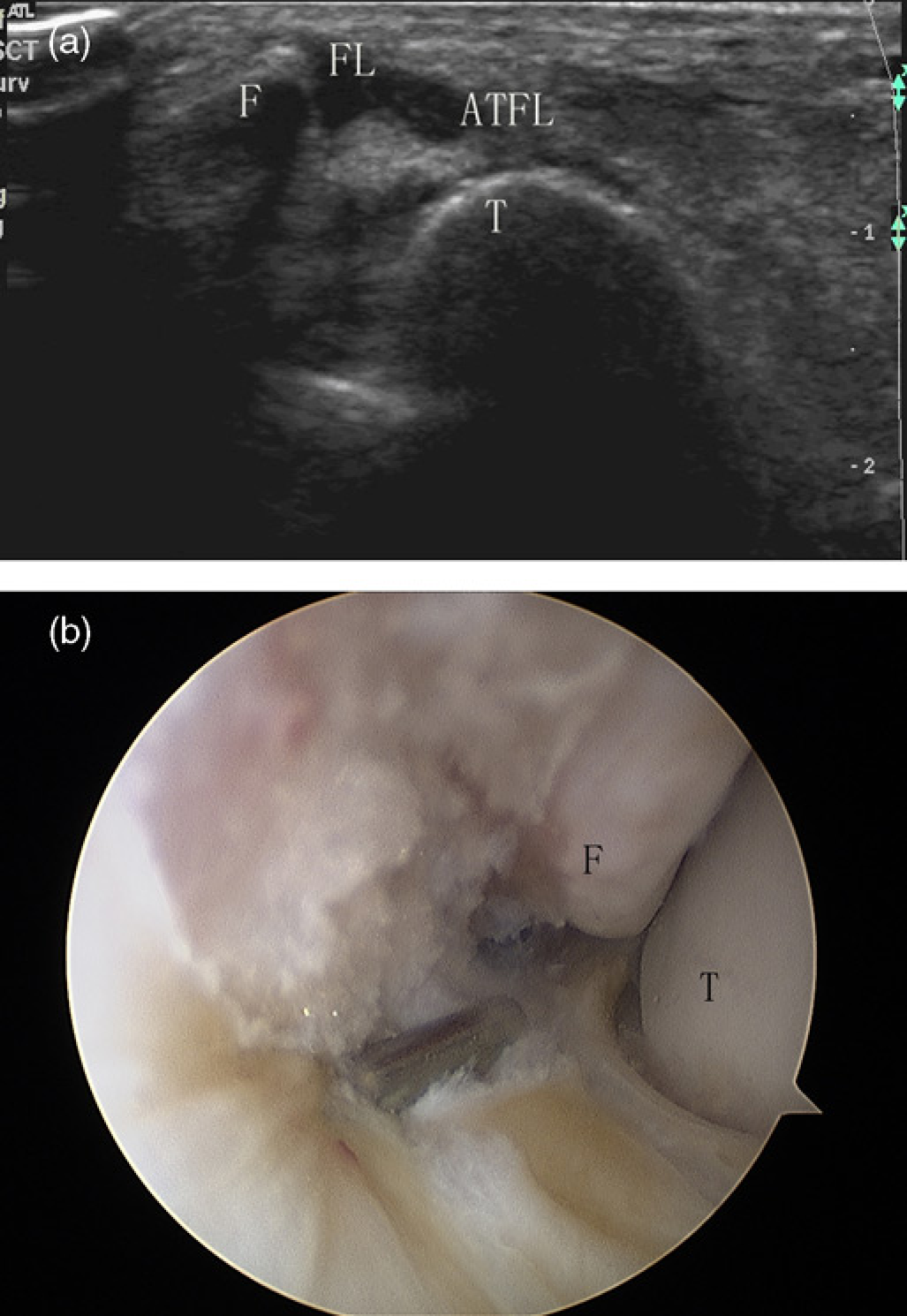
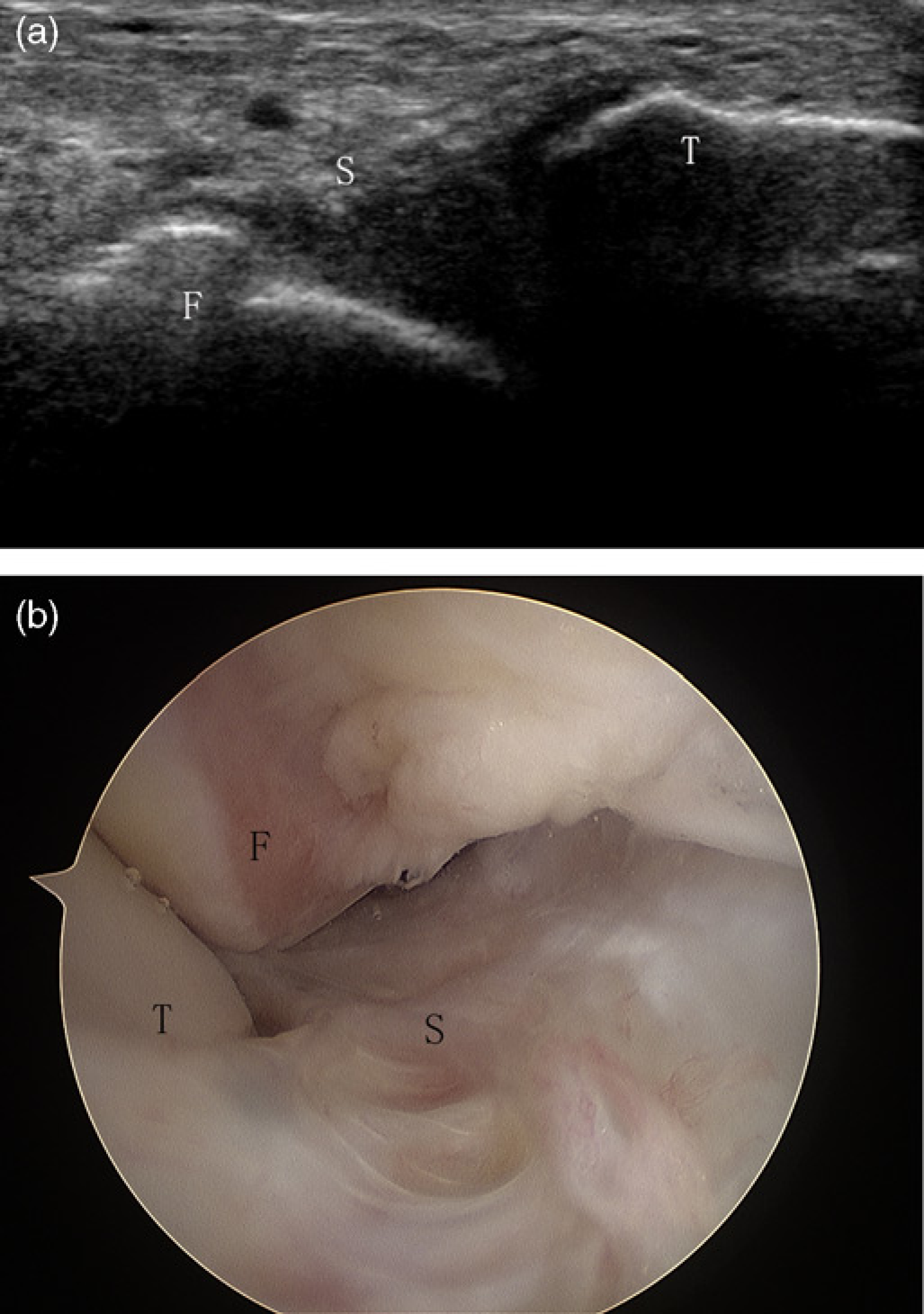
The US criteria for ATFL pathology were: (i) ligament tear: a partial or total interruption of the ligament fibers at the fibular side, talar side or in the midsubstance; (ii) lax ligament: the ligament remained curved when the ankle was in the maximum inversion and plantar flexion; (iii) thick ligament: the width of the ligament was >2.4 mm or >20% of the contralateral normal ligament (5); (iv) ligament absorbed: no ligament fibers were seen; and (iv) non-union of avulsion fracture of the lateral malleolus.
Surgical procedure
A sports medicine surgeon who was blinded to the US findings performed all surgical procedures (the first author). The patients were placed in a supine position under lumbar anesthesia. A 4-mm diameter arthroscope was used for the operation. An arthroscopic procedure was employed to evaluate the injury of the ATFL from the joint space. An injury of the ATFL was diagnosed if there is the laxity or the tear of the ligament, obvious swollen ligament, no ligament structure or an avulsion fracture when observed or detected by a probe.
Statistical analysis
The findings of the US examination and the surgery were recorded. Sensitivity, specificity, accuracy, positive predictive values, negative predictive values, and positive and negative likelihood ratios for detection of ligament injury by US examination were calculated. Analysis was performed by a statistician using SPSS 18.0 software (SPSS Inc., Chicago, IL, USA).
Results
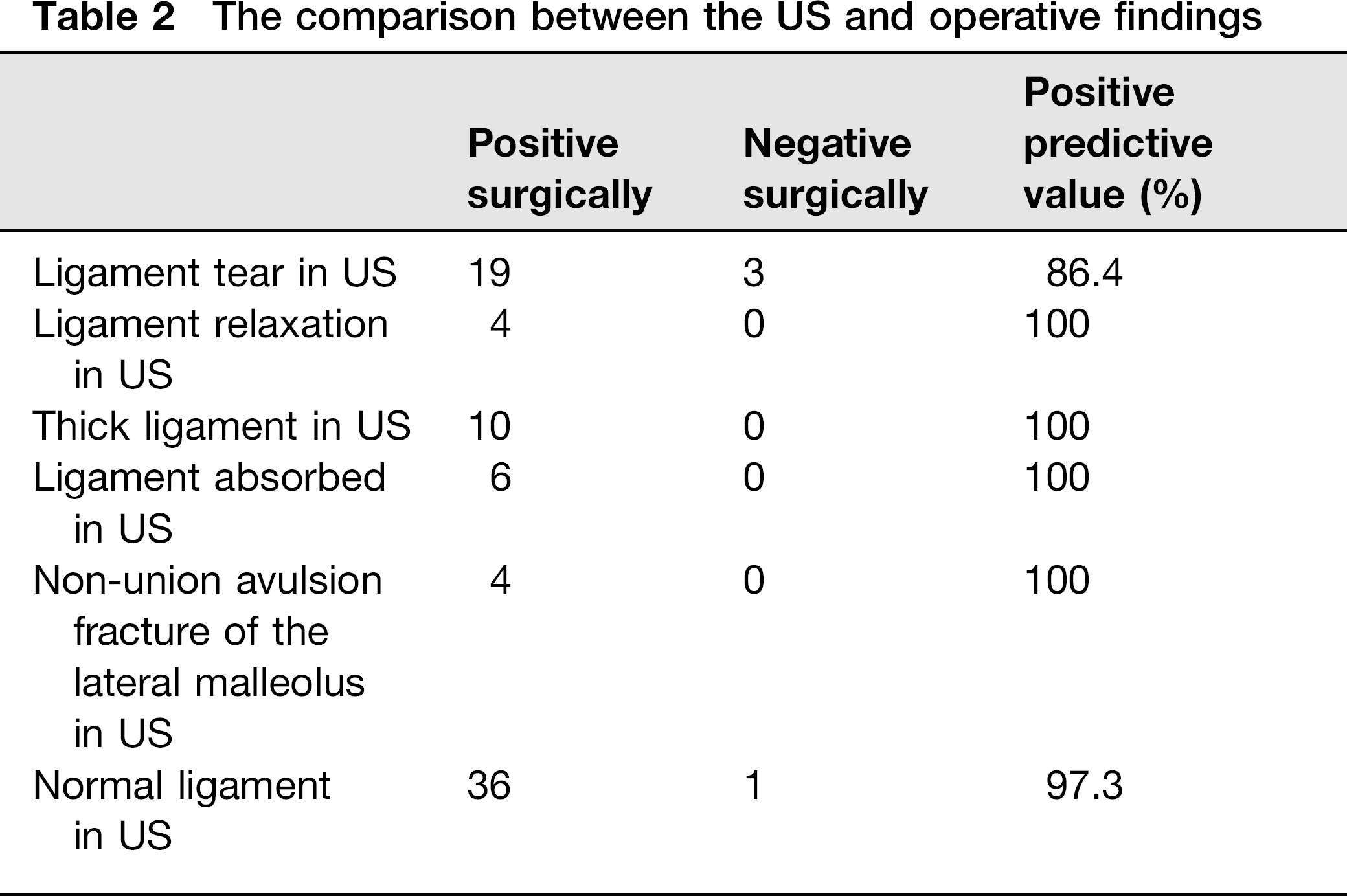
Forty-four patients were diagnosed with ATFL injury during the operation (Figs. 1–3), including: (i) the relaxation of the ATFL, five cases; (ii) tear of the ligament, 19 cases; (iii) no ligament structure, six cases; (iv) an avulsion fracture, four cases; (v) an obvious swollen ligament, 10 cases. The accuracy of US examination for the detection of ATFL injury was 95.2%, with a sensitivity of 97.7%, specificity of 92.3%, positive predictive value of 93.5%, negative predictive value of 97.3%, positive likelihood ratio of 12.7, and negative likelihood ratio of 0.025 (Table 1). The positive predictive value was 86.4% in patients with an ATFL tear detected on US examination, and 100% in patients with other positive findings on US examination (Table 2).
(a) Sonogram shows a normal anterior talofibular ligament. (b) Arthroscopic image shows a normal anterior talofibular ligament. ATFL, anterior talofibular ligament; F, fibula; T, talus (a) Sonogram shows a ligament tear at the fibular side. (b) Arthroscopic image shows a ligament tear at the fibular side (arrow). ATFL, anterior talofibular ligament; F, fibula; FL, fluid; T, talus Sonogram shows the ligament fiber has been absorbed and could not be seen. (b) Arthroscopic image shows the scar tissue instead of the ligament fiber. ATFL, anterior talofibular ligament; F, fibula; S, scar tissue; T, talus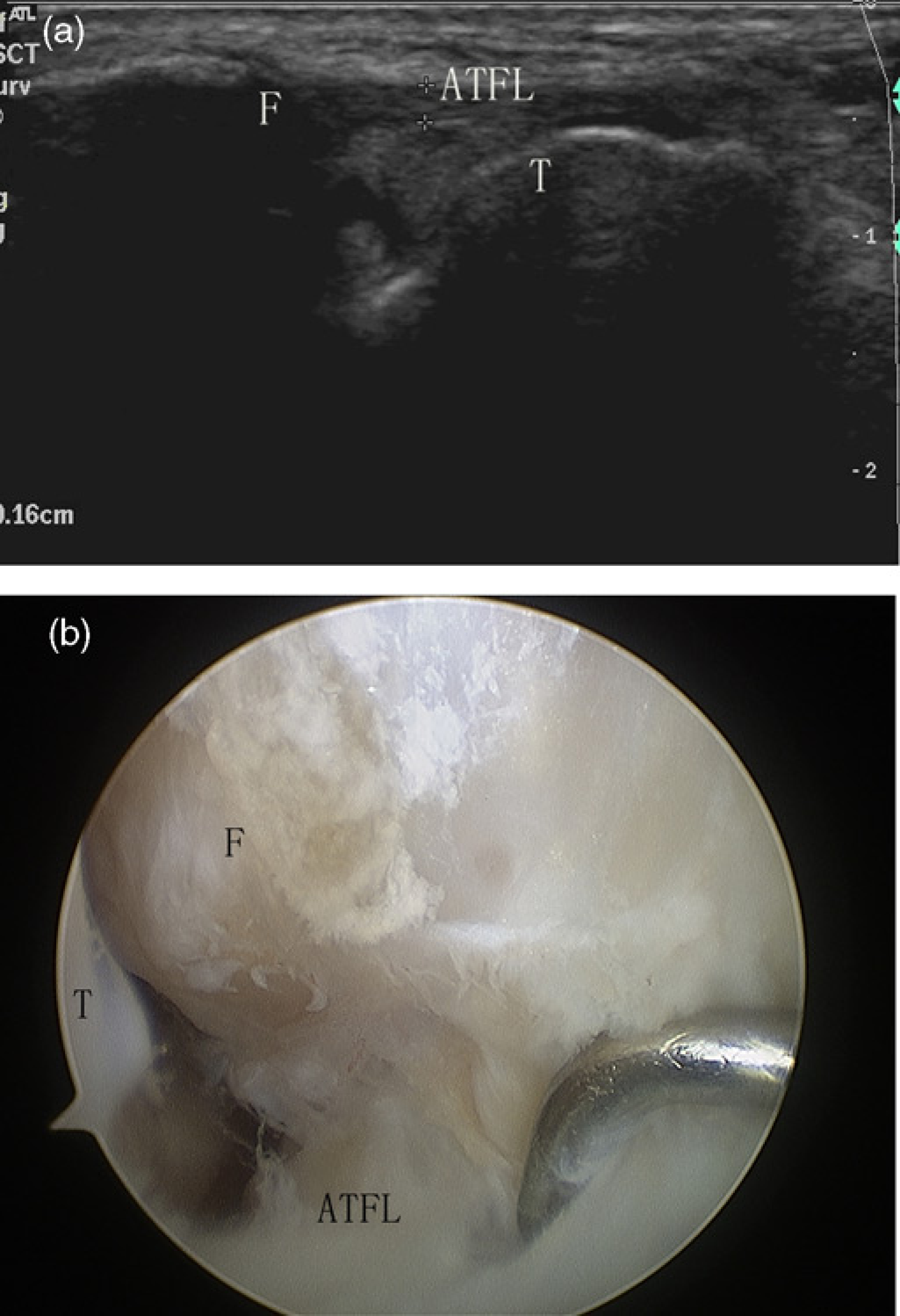
The diagnostic characteristics of US examination in evaluating chronic anterior talofibular ligament (ATFL) injury
The comparison between the US and operative findings
Discussion
Several methods have been used to identify ATFL injuries. A widely used method is stress radiograph, which uses the distance between the tibia and the talus when stress is applied to evaluate ATFL injury (6). However, Frost and Amendola undertook an extensive review of the role of stress radiography in diagnosing ATFL injury and reported that its findings are poorly correlated with actual ligament pathology (6). Additionally, fluoroscopy and arthrography have also been found to provide insufficient information regarding chronic ATFL injury (7).
Magnetic resonance imaging (MRI) is reported to be more sensitive for the diagnosis of ATFL injury than physical examination or stress radiography (8). However, this method is time-consuming and expensive. Furthermore, in chronic patients, there is an absence of hemorrhage in the joint space, of soft tissue swelling around the lateral malleolus and of high bone signals at the ligament avulsion sites, which also decrease the accuracy of MRI (9). It has been reported that conventional MRI has demonstrated only an accuracy of 71% in diagnosing chronic ATFL tears (10).
US has been used to identify acute ATFL injury (11), but is rarely used to diagnose chronic ATFL injury (1). During the past decade, the development of US equipment and techniques such as compound imaging and tissue harmonic imaging, has improved visualization of the scar tissue and ligament fibers, allowing the diagnosis of chronic ligament lesions (12,13).
In the present study, US examination had sensitivity of 97.7% and a specificity of 92.3% for detection of chronic ATFL injury, indicating the low percentages of false-negative and false-positive results. The positive likelihood ratios were >10 (12.7), and the negative likelihood ratios were <0.1 (0.025), indicating a difference between pretest and post-test probability (14). These results indicate that both negative and positive findings on US examination are likely to assist in diagnosis.
In a previous study (15), the efficacy of US in the detection of chronic ATFL injuries was evaluated using arthroscopic findings as the reference standard. The diagnosis of chronic ATFL injury with US was made with an accuracy of 87%, a sensitivity of 100%, and a specificity of 0%, which are different to the results of our study. However, that study only had a small number of cases, including only 15 chronic cases of chronic ATFL injury, of which 13 cases had positive findings on US examination. Too few cases with negative results might increase the error of the findings. In contrast, our study included 83 continuous cases reducing the error in statistics.
There were three cases of false-positive results on US examination in our series. All these cases were diagnosed as a partial ATFL tear with intraligamentous lesions on pre-operative US examination, but arthroscopy did not show ligament tear or relaxation. The lack of diagnosis of ligament injury during the surgery may be due to the limitations of the arthroscopic procedure, because the surgeon could only observe the surface of the ligament and evaluate the tension of ligament (15). Thus, we could not detect intraligamentous injury when the tautness was normal.
There was one case of a false-negative result in which a ligament with the diameter of 2.3 mm exhibited no relaxation during US examination. However, we could detect the relaxation by probing the ligament during the operation. The thickened ligament may have been due to scar tissue or to a normal anatomical variation. As the normal width of the ATFL is approximately 2 mm, a ligament more than 20% thicker is considered to be abnormal (5). Some injured ligaments may not meet this criterion and may therefore be considered normal on US. New techniques that can detect biomechanical properties of ligaments in vivo may reduce such errors (16).
There are some limitations in this study. First, we used arthroscopic findings as the reference standard. Although the intraligamentous lesions or slight relaxation of the ATFL might not be detected by arthroscopy, it is not ethical to perform an open surgery to detect all the injuries. Arthroscopy remains the reference standard of choice and can be applied to all patients. Second, no test of intra-observer reliability was performed in this study. Because it was not easy to reach consensus among different radiologists (17), the single diagnostic opinions we gathered in this study could be argued. However, the consulting co-author of this study is experienced in the field of musculoskeletal ultrasound, we were confident about his diagnostic ability. Additionally, the diagnosis is based on subjective judgments to identify ligament relaxations, which may decrease the reproducibility of the results. However, currently, there is no generally accepted technique to accurately and objectively measure the relaxation.
In conclusion, we observed satisfactory results using US examination for the detection of chronic ATFL injury, using arthroscopic findings as the reference standard. Our study demonstrates that US examination is a reliable and accurate method to evaluate chronic ATFL injury.
Footnotes
Acknowledgements
The research was supported by the National Natural Science Foundation of China (Grant No 81101391).