
Abstract
Background
Previous studies have shown that magnetic resonance imaging (MRI) has a high sensitivity for peroneal tendon pathology but more studies with surgery as a reference standard are needed.
Purpose
To evaluate the accuracy of MRI compared to surgery for characterizing chronic peroneal tendon pathology.
Material and Methods
Ninety-seven patients (57 men, 40 women; mean age, 39 years; range, 15–64 years) with chronic lateral ankle instability underwent MRI followed by surgery, with a mean MR to surgery interval of 30 days. Sagittal, coronal, and axial T1-weighted spin-echo and fat-suppressed T2-weighted fast spin-echo images were obtained for all patients. Two blinded observers evaluated the MR images without clinical information, and the results were compared to surgical findings. The following peroneal injuries were observed: tendon split, interstitial tear, swelling of the tendon, fluid collection, superior peroneal retinaculum injury, and tendon dislocation.
Results
Swelling of the peroneus longus tendon was the most common finding on MR imaging, followed by fluid collection and a split of the peroneus brevis tendon. Surgical findings showed that nine cases (9%) of interstitial tears were in the peroneus brevis and two cases (2%) were in the peroneus longus, with eight cases (8%) of splits in the peroneus brevis tendon. The sensitivity and specificity for detecting interstitial tears in the peroneus brevis were 44% and 99%, respectively. The sensitivity and specificity for detecting swelling in the peroneus brevis were 50% and 99%, respectively. The sensitivity and specificity for detecting interstitial tears for peroneus longus injuries were 50% and 96%, respectively. The sensitivity and specificity for detecting swelling in these injuries were and 100% and 96%, respectively.
Conclusion
MRI findings of chronic peroneal tendon pathology are diagnostically specific but not sensitive. MRI showed high sensitivity for diagnosing tendon swelling in the peroneus longus, but not in the peroneus brevis. MRI is sensitive but not specific for detecting negative findings.
Peroneal tendon disorders are caused by trauma, overuse, degeneration, and chronic inflammation resulting in tendinosis, tenosynovitis, and tearing (1–3). They can be associated with systemic conditions, such as rheumatoid arthritis, psoriasis, diabetes, and hypothyroidism. Anatomic variants such as peroneal tubercle, flat or convex retromalleolar fibular groove, os peroneum, and peroneus quartus muscle are also associated with peroneal tendon disorders (4). Disorders of the peroneal tendons may be misdiagnosed as acute lateral ankle sprains (1) and patient presentation and the subsequent diagnosis of peroneal tendon diseases are often delayed (2). Magnetic resonance (MR) findings for the disorders include splitting of the tendon, interstitial tears, swelling, dislocation, and fluid collection around the tendon sheath. Peroneal tendon tears are most commonly longitudinal and partial. Longitudinal tears are also called splits (5). Although previous studies have shown high magnetic resonance imaging (MRI) sensitivity for diagnosing peroneal pathology (6), these reports are mainly based on clinical information (symptoms and signs) and not on gross morphologic study. Therefore, the purpose of this study is to evaluate the accuracy of MRI compared with surgical findings for characterizing chronic peroneal tendon pathology.
Material and Methods
Patient selection
Our institutional ethics review board approved this study, and informed consent was obtained from the patients for the use of their medical records. Of patients who had visited our hospital for chronic ankle pain lasting more than 6 months between January 2006 and July 2010, the study included 97 patients who underwent lateral ankle reconstruction for chronic lateral ankle instability diagnosed based on MRI findings. The study population included 57 men and 40 women, aged 15–64 years (mean 39 years). All patients had chronic posterolateral ankle pain for at least 6 months and point tenderness over the peroneal tendons on physical examination. The exclusion criteria were acute trauma and underlying systemic pathology, such as rheumatoid arthritis, psoriasis, or hypothyroidism because the pain in the latter cases does not arise from tendons.
MRI parameters
All MRI examinations were performed with the same protocol on a 1.5-T magnet (Intera, Philips Medical Systems, Best, The Netherlands) using a knee-foot coil and fast spin-echo imaging. T1- and fat-suppressed T2-weighted images were obtained in the axial and sagittal planes, with the foot and ankle in a neutral position. All sequences used a 15 cm field of view, slice thickness of 4 mm for axial imaging and 3 mm for sagittal imaging, bandwidth of 20 kHz, and a 224 × 224 matrix. MR sequences were as follows: sagittal T1-weighted spin-echo (repetition time msec/echo time msec = 500–600/12–17), proton density (2000–2500/15–30), and fat-suppressed fast spin-echo T2-weighted image (2900–3000/60–80); axial proton density (2000–2500/15–30), and fat-suppressed fast T2-weighted spin-echo (3000–4000/60–80); and coronal proton density (2000–2500/15–30) and fat-suppressed fast T2-weighted spin-echo (3000–4000/60–80). The turbo spin-echo factor was 4 with double signal averaging.
Retrospective MRI review
Two fellowship-trained, academic musculoskeletal radiologists with 12 and 10 years of experience interpreted the MR images in consensus. The radiologists evaluated the images for the presence of variable peroneal pathology (Table 1). The following pathologic conditions were recorded: splitting, interstitial tear, swelling of the tendon, fluid collection, superior peroneal retinaculum (SPR) injury, and dislocation of the tendon. An interstitial tear of the tendon was defined as the presence of predominantly intermediate or uniform intermediate signal intensity within the peroneal tendons on T1- and fat-suppressed T2-weighted images (Fig. 1). To exclude cases of the “magic angle” phenomenon, tendons were considered intact if there was an absence of abnormal signal intensity on T2-weighted images and a lack of morphologic changes in the tendon. The peroneal tendons were considered enlarged and diagnosed as swollen when they were larger than the posterior tibialis tendon or at least 50% larger than the intact proximal tendon on axial and coronal fat-suppressed T2-weighted images (6). Abnormal fluid collection was defined as follows to exclude the possibility of reactive fluid collection due to ligament injury. The amount of fluid within the common peroneal tendon sheath was determined by measuring the maximum width of the fluid at any point around the peroneal tendons on axial and coronal fat-suppressed T2-weighted images. The maximum width of the fluid was measured from the surface of the peroneal tendons to the outer margin of the common peroneal tendon sheath. Significant fluid collection was defined as the presence of circumferential fluid within the common peroneal tendon sheath with a maximal width greater than 3 mm (6). SPR was defined as elevation or stripping off of the periosteal attachment to the lateral malleolus or as a definite tear at the level of the fibular groove. The SPR injuries were classified according to the method described by Oden (7). In type I injuries, the SPR is elevated or stripped off at the level of the fibular groove, forming a pouch into which the peroneal tendons can dislocate. In type II injuries, there is a tear of the SPR at its attachment to the distal fibula. Type III injuries consist of an avulsion fracture of the SPR at its attachment to the distal fibula. Type IV injuries involve a tear of the SPR at its posterior attachment. The presence of a peroneus quartus (PQ) muscle was defined when the accessory tendon and muscle unit descending medial or posterior to the peroneal tendons was seen on the image. The radiologists had no knowledge of the surgical results during their initial interpretation of the MR images.
MRI and surgical findings
PB, peroneus brevis tendon; PL, peroneus longus tendon; SPR, superior peroneal retinaculum
Surgical findings
Most of the operations were performed as soon as possible after the MRI, with a mean MR to surgery interval of 30 days. No medical treatment, such as NSAIDs or physical therapy, was performed during that interval. An ankle fellowship-trained academic orthopedic surgeon with 10 years of experience performed all surgical procedures. Lateral ankle reconstruction was performed using a modified Brostrom technique to treat chronic lateral ankle instability and ankle discomfort. Small incisions were made on the tendon sheath and the superior peroneal retinaculum to identify tenosynovitis, interstitial tear, and peroneus quartus. The surgeon measured the size of the tendons and ascertained whether there was any fluid collection. An enlarged tendon diameter at least 50% greater than the intact tendon in the proximal portion was considered tendon swelling. Discoloration combined with fluid collection and loss of normal striation was regarded as compatible with a diagnosis of an interstitial tendon tear (Fig. 1) (8). Tenosynovitis and tendon tears were treated with debridement and coronal suture. After the radiologists had conducted their blind reading of the MR images, the surgeon and radiologists correlated the surgical and MRI findings.
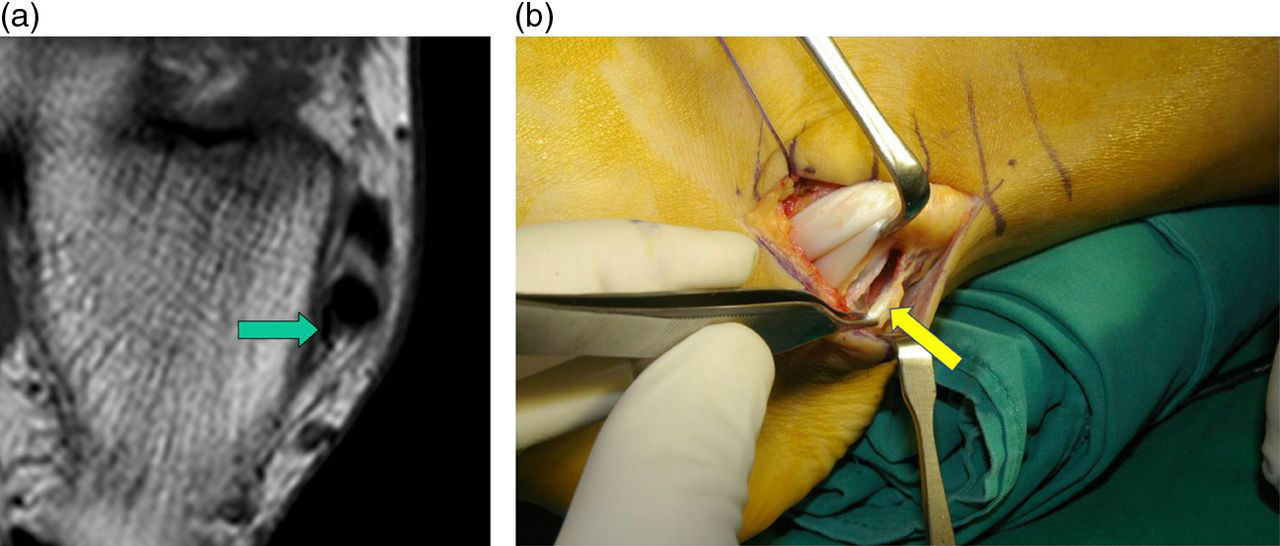
A 23-year-old woman with chronic ankle instability. (a) Axial fat-suppressed T2-weighted image (3000/60, TR/TE) shows increased signal intensity (arrow) of the peroneus brevis tendon. (b) Photograph taken during surgery reveals an interstitial tear (arrow) of the peroneus brevis tendon
Statistical analysis
The MR findings were compared with the surgical findings. Using the surgical findings as the standard of reference, the sensitivity, specificity, accuracy, and negative and positive predictive values were calculated with 95% confidence intervals. The statistical software program SAS (version 9.1, SAS Institute) was used to perform the analysis. A P value ≤0.05 was considered statistically significant.
Results
The MR and surgical findings gave different results in some parts. The incidence of abnormal findings is listed in Table 1. Peroneus longus tendon (PL) swelling was most common (9 cases, 9%) on MR images, followed by fluid collection (8 cases, 8%) and a split of the peroneus brevis tendon (PB) (8 cases, 8%) (Fig. 2). Dislocation and SPR injuries were less commonly observed (3 cases, 3% and 5 cases, 5%, respectively). On surgical evaluation, interstitial tears of the PB and split tendons were common (9 cases, 9% and 8 cases, 8%, respectively). Simultaneous injuries of the PB and PL were observed in two cases (2%). One was a PB split combined with an interstitial PL tear and the other was swelling of the PL combined with an interstitial tear of the PB. A combined injury of the SPR and PL was seen in one case, and SPR injury combined with a PB split was seen in one case. There were 65 cases (67%) with negative MR findings and 73 patients (75%) with negative surgical findings.

A 35-year-old woman with chronic ankle instability. (a) Axial fat-suppressed T2-weighted image (3065/60, TR/TE) shows a split (arrow) of the peroneus brevis tendon. (b) Photograph taken during surgery reveals a definite split (arrow) of the peroneus brevis tendon
The MRI findings compared with surgery are listed in Tables 2 and 3. MR imaging was 100% sensitive and specific for detecting dislocation, but there were only three cases. Five cases (5%) of type I SPR injuries were noted, and four cases were confirmed as type I by surgery. MRI initially diagnosed surgically-detected SPR loosening as intact. In one case diagnosed as a PB split, the PB was intact, but a PL tear was apparent during surgery (Fig. 3). In another case of a surgically diagnosed PB split, no abnormal findings were found on a second retrospective review, even with knowledge of the surgical findings (Fig. 4).

A 43-year-old woman with chronic ankle instability. (a) Axial fat-suppressed T2-weighted image (3232/60, TR/TE) shows a split (arrow) of the peroneus brevis tendon. (b) Photograph taken during surgery reveals an intact tendon (arrow)

A 24-year-old woman with chronic ankle instability. (a) Axial fat-suppressed T2-weighted image (2799/60, TR/TE) shows an intact peroneus brevis tendon (arrow). (b) Photograph taken during surgery reveals a thin cleft (arrow) in the peroneus brevis, suggesting a tendon split. The surgeon who performed the operation confirmed the split of the tendon
Comparison of MR imaging and surgical findings (n = 97)
PB, peroneus brevis tendon; PL, peroneus longus tendon; SPR, superior peroneal retinaculum
Sensitivities, specificities, and accuracies of MR findings (%)
NPV, Negative predictive value; PB, Peroneus brevis tendon; PL, Peroneus longus tendon; PPV, Positive predictive value; SPR, Superior peroneal retinaculum
Only one case was defined as having an accessory PQ muscle, which was surgically confirmed (Fig. 5). The sensitivity and specificity for detecting the existence of PQ were 100%, but there was only one case. The sensitivity and specificity for a negative examination were 97% and 68%, respectively.
A 20-year-old woman with chronic ankle instability. (a) Axial proton density image (2000/15, TR/TE) shows an accessory muscle (arrow) posterior to the peroneus longus tendon. (b) Photograph taken during surgery reveals the peroneus quartus (arrow)
Discussion
The PL passes into a common tunnel with the PB behind the lateral malleolus and underneath the SPR. It then runs under the PB and the peroneal process of the calcaneus (5, 9, 10). The peroneus brevis muscle also has a long musculotendinous junction, with the muscle fibers inserting on the tendon from the midcalf down to the lateral malleolus and often 2 – 3 cm beyond (5).
The most common peroneal tendon pathology is synovial fluid collection. Synovial fluid around the peroneal tendons is a frequent finding in asymptomatic subjects, but large volume fluid collection or fluid present only proximally typically represents an abnormality (1). We measured the amount of fluid within the common peroneal tendon sheath according to the method proposed earlier (6). Moderate grade was defined as the presence of circumferential fluid within the common peroneal tendon sheath that was greater than 3 mm in maximum width. In our study, eight of the 97 cases (8%) showed moderate to severe synovial fluid accumulation, and three cases (3%) were surgically confirmed.
PB tears occur in the young, in athletes, and in the elderly (11). Young, athletic patients complain of longstanding retromalleolar pain and swelling along the course of the peroneal tendons. A history of recurrent inversion injuries and ligamentous sprains may accompany the findings (12). PB tears in older individuals are presumably due to chronic attrition and mechanical wear and tear of the tendon (13). The tendon is prone to stress. It is positioned along the bone, superior retinaculum, and the peroneus longus tendon as it bends around the hard cortical surface of the fibula. Attrition and longitudinal tears can be caused by repetitive dynamic compression of the tendon against the retromalleolar groove by the overlying PL during ankle dorsiflexion (14). The MR findings of the torn tendon manifest as a C-shaped appearance that partially encircles the PL. The torn tendons are typically thickened and have increased intrasubstance signal intensity on T1- and T2-weighted images (5). Clefts and defects can also be found extending into the substance of the tendon.
In our study, eight cases (8%) showed PB splits and seven cases (7%) were confirmed by surgery. Interstitial tears were observed in five cases (5%) on T1- and T2-weighted fat-suppressed images (axial and sagittal) with surgical confirmation in four cases (4%). Swelling of the tendon was seen in two cases (2%) with surgical confirmation in one case (1%). MR was specific for detecting interstitial tears of the PB tendon and PB swelling, but it was not sensitive. Kijowski et al. (6) reported that increased T2 signal intensity within the peroneal tendons is highly specific, but relatively insensitive. They suggested that higher incidence of increased signal intensity within the PB than within the PL on axial images reflects the fact that the PB is more prone to attrition within the common peroneal tunnel. PL tears usually start either at the tip of the lateral malleolus or at the peroneal process of the calcaneus, near the insertion of the inferior extensor retinaculum. The tear can extend distally to the cuboid groove (15). Degenerative chronic tears may also be caused by increased friction of the PL against either a hypertrophic peroneal tubercle or the cuboid bone as the tendon curves underneath it (4). Tears of the peroneus tendon at the level of the retromalleolar groove are often associated with PB tears (11). In our study, we diagnosed only one case (1%) of simultaneous PB and PL tears, but this diagnosis did not correlate with surgical findings.
The MRI findings of PL tears are signal-intensity and morphologic abnormalities within the tendon, including longitudinal splits or disruptions (4). In our study, nine cases (9%) showed peroneus longus tendon swelling, and five cases (5%) were confirmed by surgery. Six cases (6%) showed interstitial tears on T1- and T2-weighted fat-suppressed images (axial and sagittal), and one case (1%) was confirmed surgically. MRI was more sensitive for detecting swelling of the PL than of the PB. Khoury et al. (5) indicated that increased signal intensity is difficult to characterize in some cases and that it can be mimicked by a longitudinal area of artifactual signal intensity resulting from the inability to image along the true longitudinal course of the tendon or from partial volume averaging. Hence, findings on sagittal images should always be correlated with those on axial images. We considered the finding positive only when we observed increased signals on both axial and sagittal images. In the evaluation of the PB and PL tendon itself, we found low sensitivity and high specificity. The intraoperative observation provides more detailed and direct visualization without overlying subcutaneous fat and skin tissue. In addition, the surgeon can manipulate the peroneal tendon freely, which would not be possible in an imaging study. MR imaging also can yield artifacts such as the partial volume effect and limitation of resolution. As a result, subtle pathology can be missed in the diagnosis and MR can show low sensitivity. Contrarily, we think that the pathology seen on MR could be detected from the surgical field.
Subluxation or dislocation of peroneal tendons occurs during sudden, violent reflex contraction of the peroneal muscles in an effort to overcome resistance of the fibro-osseous tunnel (16). We noted three cases of peroneal tendon dislocation (3%), and all were confirmed by surgery. Detecting tendon dislocation was relatively easy because normally, peroneal tendons lie distally in a concave groove of the distal fibula. However, when dislocated, this alignment changes and can be easily detected.
The SPR forms the posterolateral border of the peroneal tunnel and thus maintains the peroneal tendons in place within the fibular groove. Tears of the SPR allow dislocation of the peroneal tendon (17, 18). We noted simultaneous peroneal tendon dislocation and superior retinaculum injury in one case. However, the MR diagnosis did not correlate with the surgical findings. The mechanism of injury to the SPR includes sudden dorsiflexion of the foot with concomitant violent contraction of the peroneal muscle. This can cause the SPR to strip from its distal fibular attachment as well as secondary lateral dislocation of the peroneal tendons out of the retromalleolar groove (4). The SPR is optimally visualized on axial MRI as a low-signal band originating laterally from the distal fibula in the region of the fibular groove (4). SPR injuries were classified by the Oden method (7). Type I injury is the most common, followed by type III. We noted only type I SPR injuries (five cases), and four cases were confirmed by surgery.
The PQ muscle is one of a group of accessory peroneal muscles unique to humans (19). This muscle originates from the distal leg, frequently from the peroneal muscles, and the distal attachment is not absolutely fixed (20). The PQ muscle descends medial and posterior to the other peroneal tendons. Recognition is important because of occasional reports of ankle pain, ankle joint instability, and predisposition to peroneal tendon subluxation ascribed to the presence of PQ muscle (20). On axial MR images, a PQ is visualized posteromedial or medial to the PB and is separated from it by a fat plane (21). Cheung et al. (20) reported the incidence of PQ at about 10%, while our study showed a markedly lower rate (1%) of surgically confirmed cases.
The incidence of negative examinations (in other words, without positive findings) was about 67%. MRI was sensitive (97%) but not specific (68%) for negative examinations. In one case that we diagnosed as intact peroneus tendon, surgery revealed a PB split (Fig. 3). In another case that we diagnosed as PB swelling, surgery revealed a PL tear. It is not clear why such discrepancies occurred. We presume it was because MR imaging is a static study, while surgeons can dissect the tendon to identify even subtle splits or tears that may be missed on MRI.
A major limitation of our study was the small number of positive findings. The total study population was large, but the numbers of each MRI finding were small. Second limitation of our study was the population bias regarding age and sex. Efforts to reduce the deviation between sex and age were not attempted. The third limitation was that selected cases were confined to symptom-positive patients. Therefore data concerning accuracy only would apply to symptomatic group of patients. The fourth limitation was that our study was based on the 1.5 T MRI not on the 3.0 T MRI. 3.0 T MRI provide more detailed anatomic information with good anatomic resolution, so the accuracy of the data may not be the most up-to-date. However, a great number of 1.5 T MRI units are still in clinical use. The interval between the MRI and surgery was also problematic. We attempted surgical intervention as soon as possible after MR. Nevertheless, some tendon changes and fluid collection along the tendon sheath was inevitable during the interval. Because most of the patients had chronic, persistent pain and no particular therapy was performed, we assumed the change was minimal.
In conclusion, MRI findings of chronic peroneal tendon pathology are diagnostically specific but not sensitive. MRI showed high sensitivity for the diagnosis of tendon swelling in the PL, but not in the PB. MRI is sensitive but not specific for detecting negative examinations.