
Abstract
Background
Sufficient radiopacity of stents is a prerequisite for safe interventions and minimization of the radiation dose for the patient and the interventionist. Modern nitinol stents are considered less radiopaque compared to formerly used stents.
Purpose
To evaluate the objective detection rate (ODR) and the subjective radiopacity score (SRS) of four self-expanding nitinol stents with their markers on a phantom human pelvis.
Material and Methods
We evaluated the ODR (as a percentage of correctly identified stents) and the SRS (on a scale from 0 = not visible to 4 = excellent visibility) for four self-expanding nitinol stents (SinusSuperflex, SMART, Luminexx, Zilver) with 8 mm diameter and 40 mm length. Stents were placed on a phantom human pelvis and images of the stents were taken in four different positions (right and left lumbosacral joint and near the right and left limbus acetabuli) using the following modes: spotfilm, pulsed fluoroscopy (4, 7.5, 15, and 30 pulses/min) and at three different digital magnification modes. Dose area products (DAPs) were assessed.
Results
ODR and SRS, respectively, were significantly increased for the SMART stent compared to all other tested stents (P < 0.05): SMART 93.53% and 2.43, SinusSuperflex 90.81% and 2.21, Luminexx 90.39% and 2.20, and Zilver 89.28% and 2.21. ODR was significantly reduced in position 3 where the bone overlap was more pronounced for all stents (detection rates 77.14-79.56%). An increase in magnification significantly improved the ODR and SRS for all stents (70.33-99.25% and 1.07-3.28, respectively, P < 0.05). Increased pulsing frequency did not improve the ODR of the various stents but did increase the DAP.
Conclusion
The SMART stent had the best overall performance. In the presence of bone overlap, all self-expanding nitinol stents had poor results. Increased pulsing frequency did not improve ODR or SRS but did increase the DAP. Use of digital magnification modes had no effect on DAP increasing ODR and SRS.
Percutaneous transluminal angioplasty (PTA) with optional stenting has become the treatment of choice for atherosclerotic stenosis and occlusion of peripheral arteries (1–3). In recent decades, stent manufacturers have developed a vast array of endovascular stents with superior visibility. Examples include stainless steel stents (e.g. Palmaz stents), Wallstents and stents made of tantalum (Strecker stents) (4–11). The radiopacity of stainless steel stents is good, and those stents are currently in use, e.g. in iliac or crural interventions. The standard, however, for some iliac and most femoropopliteal vascular interventions is the use of nitinol stents, which have been shown to provide better expansion rates, biocompatibility, and flexibility (8, 10–12).
Few data are available about the radiopacity of bare nitinol stents. Our study aimed to quantify radiopacity for those stents by evaluating objective detection and subjective stent visibility with variable magnification modes, pulsing frequencies, and stent positions. In previous studies using different stents, increased pulsing frequency was shown to improve stent detection and visibility (10). Aufrichtig et al. supposed that excessive pulsing frequencies might have limited benefits due to the limitations of the human visual system (13). A combination of pulse-dose and frequency was recommended for achieving improved image quality (14).
Radiopacity of stents is important for correct stent deployment, sometimes added by intravascular ultrasound (15). Stent displacements can close vascular side branches or worsen the pressure in type II endoleaks (16). For this reason, highly visible stents are safer for stent positioning and require less fluoroscopy time and less radiation exposure to the patients and the physicians.
Material and Methods
Four commonly-used self-expanding nitinol endovascular stents were evaluated in this study: Sinus Superflex, SSF (OptiMed; Ettlingen, Germany), SMART (Cordis; Johnson & Johnson; Miami Lakes, FL, USA), Luminexx (Angiomed/Bard; Karlsruhe, Germany), and Zilver (Cook; Bloomington, IN, USA). All stents were 40 mm long with a diameter of 8 mm. All stents possessed radiopaque markers consisting of tantalum markers for the Luminexx, SMART, and SinusSuperflex stent and gold markers in case of the Zilver stent (Fig. 1).
Evaluated self-expanding nitinol stents in order, a = SSF, b = 
Experimental protocol
Before imaging, all stents were expanded in a water bath at 36°C. They were then placed on a phantom human pelvis (from a 55-year-old patient without any osteoporosis) with the pelvic osseous structures inside a plastic phantom human body. The plastic was enriched by plumb particles of the corresponding average X-ray density of pelvic human soft tissue. The stents were placed in projection of the right and left lumbosacral joint (positions 1 and 2, respectively) and in projection of the line from the posterior inferior iliac spine of the os ilium to the limbus acetabuli (position 3/right side, position 4/left side). Stent images were taken at spotfilm, pulsed fluoroscopy (4, 7.5, 15, and 30 pulses/min) and at three different magnification modes. All images were obtained with a conventional image intensifier (II) Fluorospot T.O.P system installed in 2005 (Siemens, Forchheim, Germany) at 80 kV with a 0.2-mm copper filter and at a 40-cm source-to-object distance and a 110-cm distance between the radiation source and the detector (values comparable to those used routinely). Exposure was performed in an anterior-posterior position at constant room temperature of 20°C. The angiography machine was composed of a 16-inch Image Intensifier (II) and two 21-inch high-resolution monitors (1024
Dose area products
For the evaluation of dose area products (DAPs), the corresponding values calculated by the Fluorospot TOP were recorded for every mode (fluoroscopy at 4, 7.5, 15, and 30 pulses/min) and averaged. The accuracy of the intrinsic measurement of DAP values was checked by the manufacturer. Further measurements by our institute's radiation physicist showed that the machine tended to overestimate the DAP in a range from 5-10% (verified with an ionization chamber, Diados PTW at 70 kV, 2.55 mm Al filter).
Reading
The DICOM images obtained were presented as follows. Each stent (n = 4) image plus one control image were presented to each of the six readers on a clinical routine diagnostic 3 Megapixel EIZO RadiForce GS 320 325 × 433 mm screen (1536 × 2048 pixel). The images were presented 10 × at each of the four positions, at each of the five pulse sequences and at each of the three magnifications. Additionally, images of a “sham” control (pelvis at the respective fluoroscopy modes/magnification modes without any stent) were shown to the readers at random. Altogether, each reader evaluated a total of 3000 pictures over the course of 10 sessions. All pictures were read by six different readers (two experienced radiologists with 6-12 years of experience in interventional radiology, four radiologists with 5-7 years of experience). The readers looked primarily at the stent contours/overall stent density and utilized the respective markers of the stents in cases when the contours were difficult to identify. We calculated the correct objective stent detection rates (ODR) defined as the percentage of correctly detected stents (including the respective marker) in the respective position of the human phantom. We also assessed the subjective radiopacity/visibility score (SRS), defined as subjective visibility of the respective stent (including the respective marker) in the respective position using a scoring score from 0 to 4 (0, not visible; 1, poor visibility; 2, moderate visibility; 3, good visibility; 4, very good visibility).
Statistical analysis
The radiopacity scores were analyzed with contingency analysis and the Wilcoxon and Kruskal Wallis tests for multiple comparisons. Statistical significance was assumed for P values <0.05. Sensitivity and specificity for correct stent detection were evaluated with the aid of JMP Version 7 (SAS Institute Inc., Cary, NC, USA). All differences were statistically significant at a P < 0.05 level.
Results
Radiopacity, correct stent detection rates
The overall best stent ODR over all modes was achieved with the SMART stent, which performed statistically better than the three other stents at a P < 0.05 level (93.53% vs. 90.81% for the Sinus Superflex (SSF), 90.39% for the Luminexx and 89.33% for the Zilver stent (Fig. 2). As shown in Fig. 3, ODR did not improve with increasing pulsing frequencies in the fluoroscopic modes for the respective stents, P < 0.05. However, when using fluoroscopy, the SSF stent and the Zilver stent performed worse than the SMART and Luminex stent (ODRs between 83.67% and 86.50% vs. 92.61% and 95.89%, P < 0.05 for the comparison SMART, Luminexx vs. Zilver, SSF respectively) (Fig. 3).
Upper left image = SinusSuperflex, upper right = Smart, lower left = Luminexx, lower right = Zilver stent in position 1 at 30 pulses/s fluoroscopy mode without magnification
The percentage of correctly identified stents (the respective stents are named on the right: SSF = Sinus Superflex, 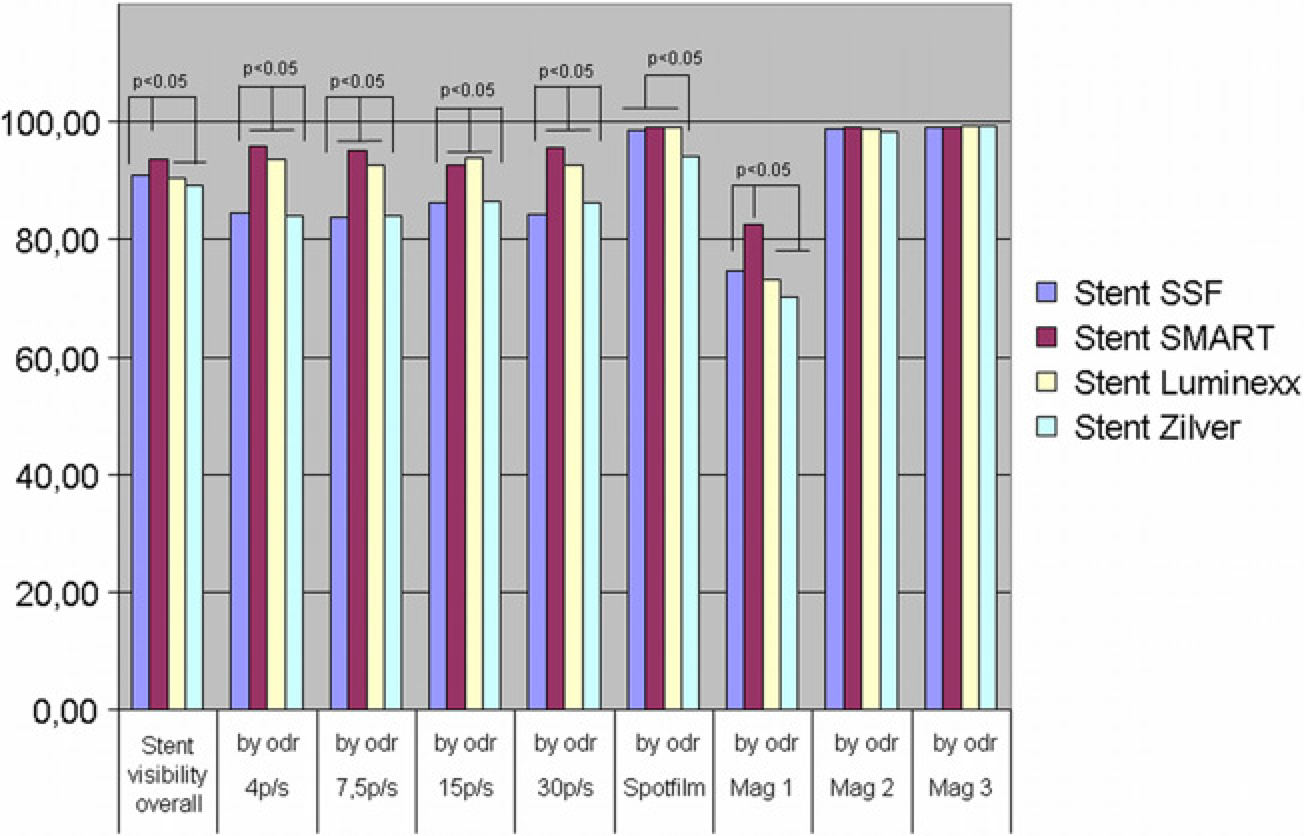
In spotfilm mode, the respective ODRs were 99.02% for the SMART and Luminexx stent compared to 98.46% (SSF) and 94.24% (Zilver stent), P < 0.05 for the comparison Zilver vs. the other three stents. For all stents, ODRs increased considerably using magnification modes (Fig. 3), showing a statistically better detection rate for the SMART stent than for the other three stents at baseline (82.50% vs. 70.33–74.67%, P < 0.05). For the Mag2 and 3 modes, the statistical advantage of the SMART stent compared to the others was lost (ODR values at Mag2: 98.25–99.08%, at Mag3 99.0–99.25% for all stents). As expected, correct stent detection rates diminished considerably in position 3 where the bone overlap was more pronounced (P < 0.05 in cases of all tested stents vs. all other positions). In contrast to baseline, the SMART stent did not have improved scores in position 3. Differences between the stents were minor and did not show a clinically relevant advantage for any of the tested stents (correct detection rates from 77.14–79.56%, P > 0.05). In position 1, ODR values for the four different stents ranged from 84.96–87%, from 96.10–97.22% in position 2, and from 99.00–99.78% in position 4.
Subjective visibility of the stents
The SRS values for the respective stents correlated well with the ODR. As shown in Fig. 4, the best overall subjective visibility value was achieved by the SMART stent (2.43 points) followed by the SSF and Zilver stents (2.21 points) and the Luminexx stent with 2.20 points over all modalities and positions (P < 0.05 for the SMART vs. all other stents). As for the ODR, the SRS for the respective stents in the different fluoroscopy modes (4, 7.5, 15, and 30 pulses/ min) did not differ significantly (SSF 1.91–1.99, SMART 2.10–2.36, Luminexx 1.89–1.98, Zilver 1.88–2.00). However, the SMART stent performed subjectively better than the other three stents for fluoroscopy (P > 0.05 for SMART vs. rest) (Fig. 4).
Subjective visibility ratings (SRS) overall and for the respective pulsing frequencies in fluoroscopy (4–30 pulses/min) and at the respective magnification modes (Mag1 = baseline, Mag2, and 3 correspond to the first and second magnification of the Fluorospot T.O.P., Siemens) for the respective stents (named on the right of the graph). Columns showing significantly different values at a P < 0.05 level are linked by parenthesis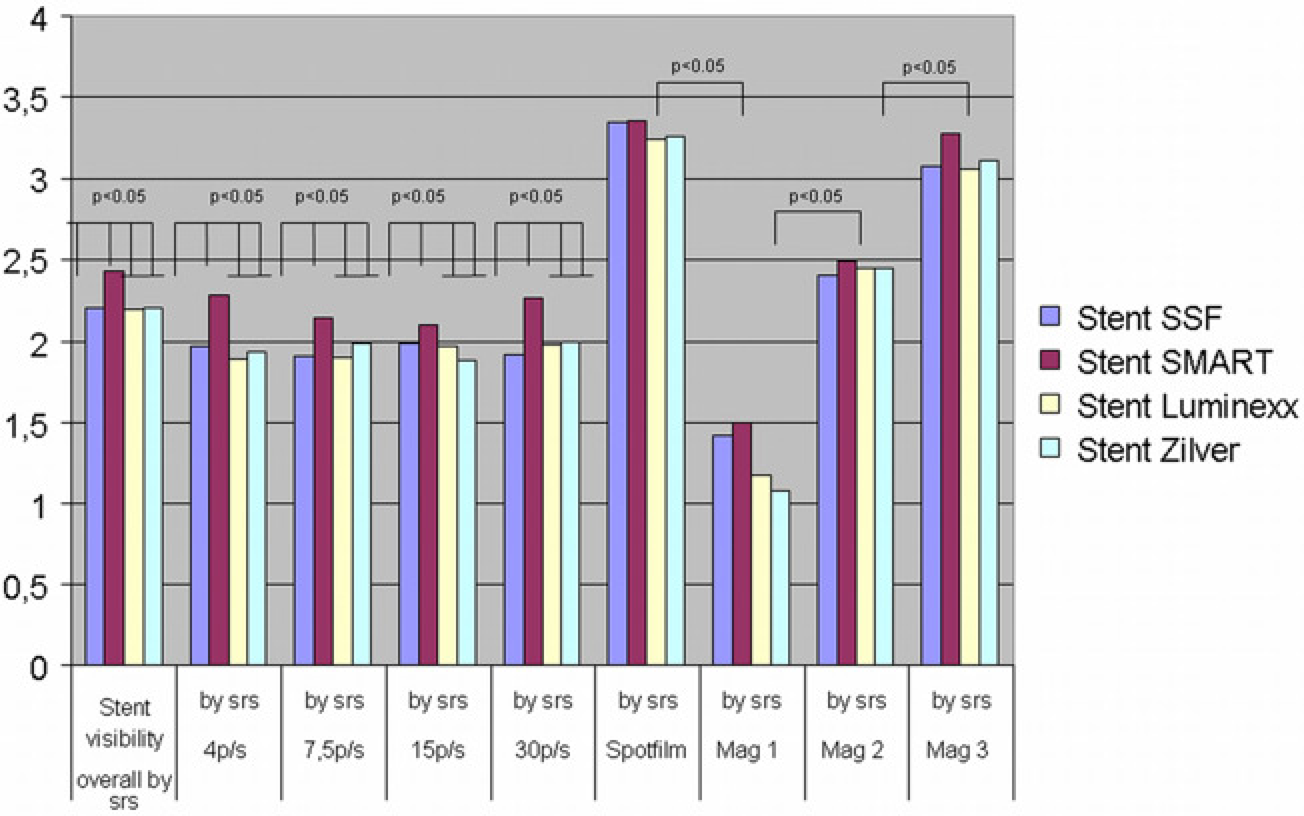
At spotfilm mode, the differences between the four stents were much less pronounced and SRS increased significantly in comparison to fluoroscopy (3.26–3.36 vs. 1.88–2.28, P < 0.05, respectively). Magnification is subjectively an important factor for stent visibility. At Mag1, the SRS values were significantly higher for the SMART and SSF stent than for the Luminexx and Zilver stent at a P < 0.05 level (1.50 and 1.42 vs. 1.17 and 1.07, respectively). Increased magnification improves the subjective stent visibility (Mag2 2.41–2.49, Mag3 3.06–3.28). In contrast, the ODR improvement is marginal between Mag2 and 3 as shown in Fig. 3. In position 3, where bone overlap is present, SRS is similar for all stents (1.59–1.63, P > 0.05 in between the stents) correlating with minor differences in ODR (77.14–79.44%, P > 0.05).
Dose area products
DAP depends proportionally on the pulse frequency during fluoroscopy. At the spotfilm mode, images were obtained at 80 kV with a DAP per image of 0.41 μGy*m2. Using the digital magnification modes, DAP was 0.40 and 0.43 micro Gray per square meter, μGy*m2, respectively (Mag1 and 2). In the fluoroscopy mode (30 s fluoroscopy time) the mean DAP was 1.32 μGy*m2 at 80 kv and 30 pulses/min. At 15 pulses/min and 80 kV, the mean DAP was 0.66 μGy*m2. At 7.5 and 4 pulses per min (80 kV) in the fluoroscopy mode, the mean DAP was 0.32 μGy*m2 and 0.19 μGy*m2, respectively (Fig. 5). All DAPs showed a statistically significant difference for the respective pulsing frequencies at a P < 0.05 level. In contrast, digital magnification does not increase DAPs but does have a considerable impact on objective and subjective stent visibility.
Applied radiation dose with standard deviation in cGy/cm2 (30 s fluoroscopy time) at the respective magnification mode (normal magnification = baseline, magnification 1 and 2 correspond to the first and second magnification of the Fluorospot T.O.P., Siemens) depending on the respective fluoroscopy mode (given on the right). All values within a magnification group were significantly different (P < 0.05). The magnification groups were not significantly different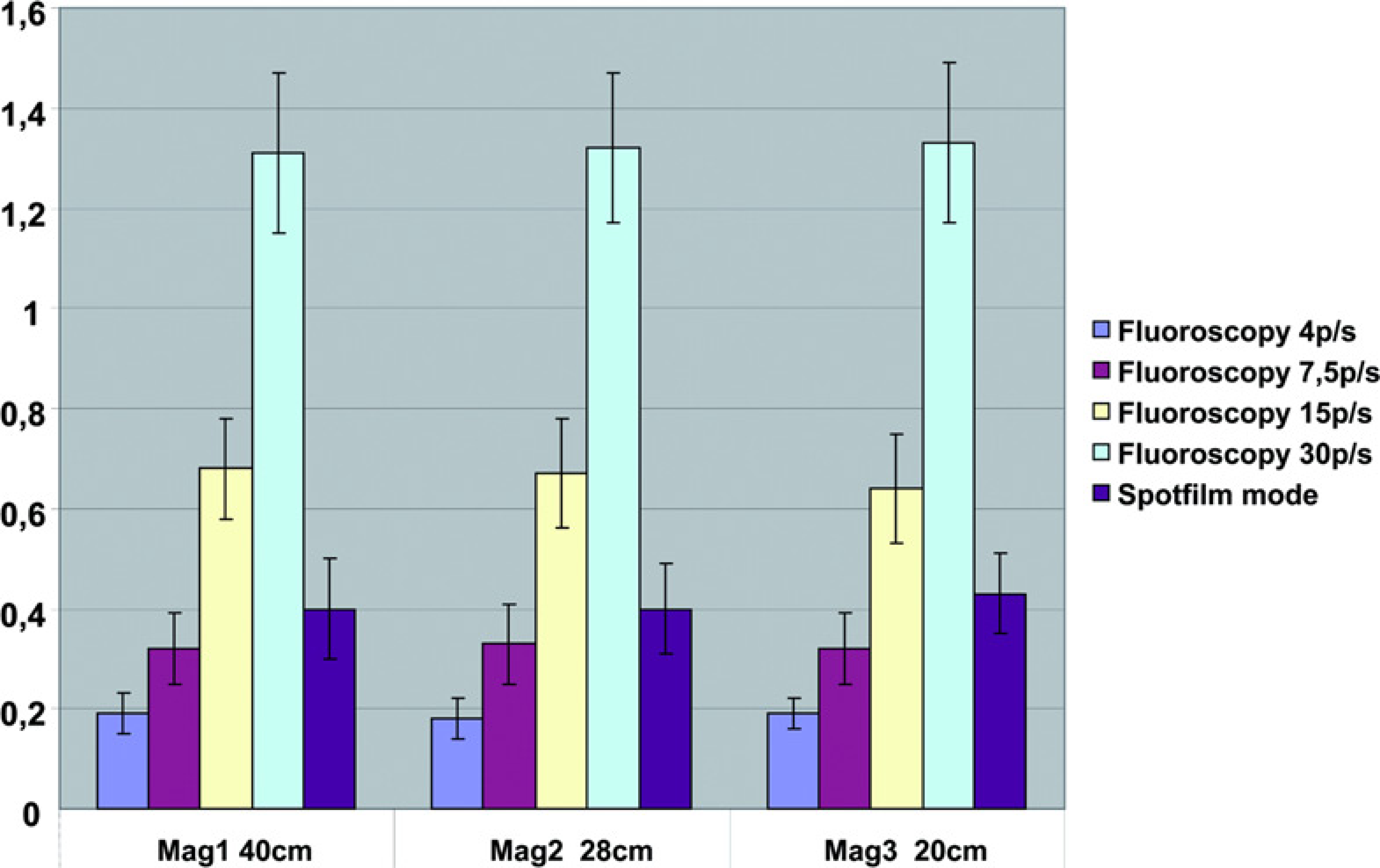
Discussion
It is important to quantify differences in stent detection rates and subjective stent visibility because superior stent/delivery device visibility aids in correct detection and placement of stentsin the desired area, e.g. into the lesion. This is especially important in the area of the aortic bifurcation orat side branch origins. Post-interventional stent detection may be important to assess the risk of eventually developing in-stent restenosis. Radiopacity of stent and deployment devices contribute to a more accurate stent placement and reduced procedure time, thereby also reducing the radiation doses to the patients, physicians, technicians, and nurses.
In the past, stent radiopacity was measured by analyzing the absorption of X-rays with a 256-step gray scale (12). Later, Diet et al. compared stents to a standardized aluminum step wedge and were able to assess the amount of aluminum required to make a stent invisible (17). We used a standardized in-vitro phantom of a human pelvis and placed the stents in four clinically relevant positions (iliac vessels) to obtain values that are more easily translated into a clinical routine context. This method was also used in 2004 by Wiskirchen et al. (10). We did not consider the use of computer-aided detection (CAD) systems to detect the stents even though this system could have isolated the visibility of the markers from those of the stent struts as it was felt the settings should be similar to daily routine conditions.
Data comparison, ODR, and SRS
Generally, ODR and SRS values correlated well for nearly all modes and magnifications. The SMART stent did show the best ODR and SRS values over all modes. Nevertheless, all stents were found to have insufficient radiopacity, especially when bone overlap was present.
Wiskirchen et al. (10) found much larger ODR differences in their stent evaluation. This is due to the more heterogeneous stent group composition, different stent lengths (21–44 mm), and different stent materials (stainless steel stents and nitinol stents).
In that same study, the SRS values varied between 0.97 (Palmaz Corinthian PQ294, 20 mm length) and 3.25 (Covent stent, 40 mm length), scale from 0–4. The SMART stent achieved a subjective visibility value of 2.15 points, and ODR was from 90–100% in fluoroscopy mode. In comparison, the SRS of the Covent stent was 3.25, and the objective detection rate was 99.375–100% (in fluoroscopy modes) (10).
Given that the absorption of X-rays depends on the number of protons of the elements being used, the visibility of nitinol stents is inferior compared to stainless steel stents, and the visibility of both stents is inferior compared to tantalum stents (Strecker Stents). The thickness of stent struts and the stent design and length are other factors that influence stent visibility. The SMART stent possessed the highest density of stent struts in our stent group, and this finding may offer a possible reason for its superiority (Fig. 1).
Efficacy of fluoroscopy modes
In our study, the SMART stent did not perform best when bone overlap was present. Evaluating the different fluoroscopy modes, the use of digital magnification was able to improve ODR and SRS considerably (without augmenting the DAP). However, the difference between the second and third magnifications in the SRS is substantially a subjective phenomenon. At baseline, the SMART stent performed significantly better compared to the other stents (P < 0.05). ODR and SRS were better for all stents using the spotfilm mode at the cost of higher DAPs. Interestingly, increasing pulsing frequencies in fluoroscopy modes did not improve either ODR or SRS values for any of the tested stents but did augment the applied DAPs. This important finding contrasts Wiskirchen's results. A reason for this might be the use of a more modern angiography machine or that the amplitude of pulses increased with frequency.
Dose area products
The DAP level using pulsed fluoroscopy is proportional to the pulse frequency used (the machine uses 5.4 μGy per pulse). Therefore, increasing fluoroscopy pulses leads to an increase of DAP. However, as observed above, the increase in pulsing frequency did not lead to an improved objective or subjective stent detection rate or visibility. In contrast, digital magnification did not increase DAP but had a considerable impact on objective and subjective stent visibility. This is because magnification is performed electronically with the FT machine so that no additional radiation dose is necessary. The same technique was found to dramatically reduce radiation dose in chemoembolization (18) and a dose reduction effect for digital magnification was also shown for flat panel angiography machines (19). However, electronic magnification is not favorable in all cases. For example, in screening mammograms, electronic magnification models were rated inferior to real magnification models in terms of microcalcification detection (20). This disadvantage in image quality is not significant for the needs of interventional radiology.
One limitation of our study is the intrinsic measurement of the DAP values (intrinsically measured by the machine). However, the values were proven to be reliable by measurement with an ionization chamber. Additionally, we did not explicitly distinguish whether the stents were recognized by their stent struts or by their marker. Another limitation is that our study design is valid for stent visibility in native vessels but objective and subjective stent visibility might differ in heavily calcified arteries or if the stents had been placed directly into a phantom (denser substances/calcified plaques in contact with the stent).
In conclusion, our data show that visibility of self-expanding nitinol stents is generally poor, especially over dense bones. In our setting, however, over all modes, the SMART stent performed significantly better than the Sinus Superflex, Luminexx, and Zilver stents in terms of subjective and objective visibility.
An important finding was that the increase of pulsing frequencies in the fluoroscopy mode did not improve ODR and SRS but did result in increased applied DAPs. In contrast, the use of digital magnification improved ODR and SRS without increasing DAPs. This means DAPs could potentially be easily reduced using low pulsing frequencies (and digital magnification) without losing quality, which is an important finding for everyday routine work. The use of low pulsing frequencies may not be applicable for dynamic aspects of interventions.