
Abstract
Background
Radiofrequency ablation (RFA) of liver tumors is a mainstay of interventional oncology. Its application, however, is limited by tumor size and location with lesions located within 1 cm to the gallbladder being at increased risk for complications.
Purpose
To evaluate the safety of hepatic RFA after bile aspiration with or without additional hydrodissection for lesions adjacent to the gallbladder.
Material and Methods
Six patients undergoing RFA of tumors with a distance of less than 1 cm to the gallbladder were retrospectively identified from a computer database. All patients underwent RFA combined with percutaneous bile aspiration from the gallbladder. In four patients additional hydrodissection was performed. Technical success and post-interventional complications were assessed by reviewing images and patient charts.
Results
Ablations were successfully completed in 5/6 patients. In one patient with incomplete ablation re-ablation was performed 2 months after the initial procedure. Minor complications occurred in three patients, including right-sided pleural effusion, hematoma in the gallbladder fossa, and intralesional hemorrhage in one patient each. There were no cases with cholecystitis or damage to the gallbladder during follow-up.
Conclusion
Bile aspiration with or without additional hydrodissection permits safe RFA of tumors located close to the gallbladder.
Hepatocellular carcinoma (HCC) and colorectal cancer (CRC) are among the most common tumors worldwide (1–3). Liver metastases from colorectal cancer occur in more than 50% during the lifetime of patients suffering from CRC (2). As only about 5–15% of patients with HCC and 20–30% of patients with hepatic metastasis from CRC are considered candidates for surgery, various interventional techniques such as chemoembolization or thermal ablation have been introduced in clinical routine practice.
Currently, the liver represents the best investigated organ for thermal ablation with radiofrequency ablation (RFA) being the most commonly used ablative treatment for liver tumors (4,5). Hepatic RFA is considered safe with a complication rate below 8% (6). In a recent meta-analysis major complications were reported in 4.1% of procedures with a mortality rate of 0.15% (7). Complications are commonly related to the biliary system. De Baère et al. described liver abscess as the most common major complication after the RFA, especially in patients with bilioenteric anastomosis (8). Furthermore, changes of the bile ducts, e.g. post-interventional dilatation or biloma, may develop after the RFA (9,10). Performing RFA close to structures adjacent to the liver contributes the potential risk of damaging the respective structure. In case the area of ablation is close to the gallbladder complications such as cholecystitis and gallbladder perforation may occur (10–12). Chopra et al. described self-limited mild cholecystitis in 42% of procedures after the ablation of tumors adjacent or within 1 cm to the gallbladder (13).
We were interested to evaluate whether gall bladder aspiration is suited in reducing the risk of thermal injury to the gallbladder by minimizing the contact with the heated area. Therefore, the goal of this retrospective study was to assess the safety of hepatic RFA after gallbladder aspiration with or without additional hydrodissection in lesions within 1 cm to the gallbladder.
Material and Methods
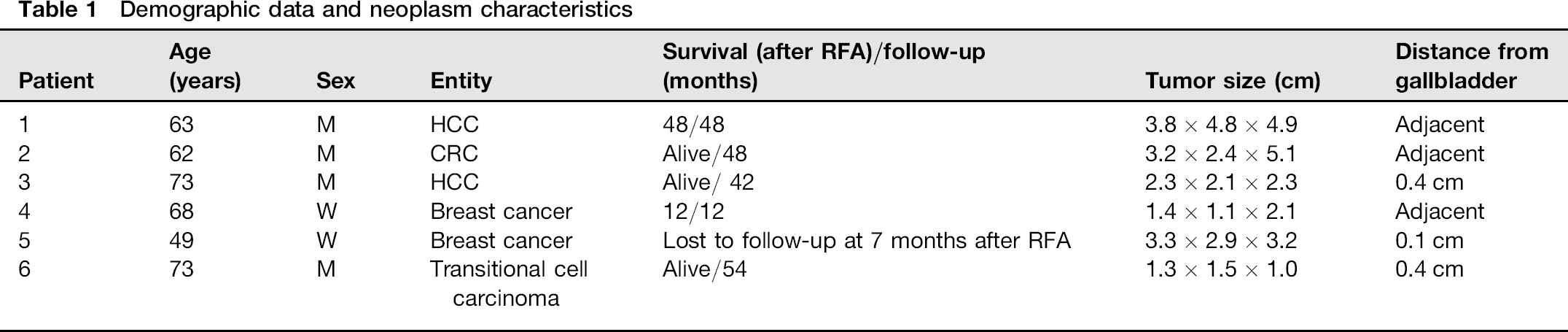
A retrospective database query retrieved six patients who underwent CT-guided RFA for lesions in close proximity to the gallbladder with a minimum distance of <1 cm. Patients suffered from HCC (n = 2), breast cancer (n = 2), transitional cell carcinoma (n = 1), and CRC (n = 1; Table 1). Written informed consent was obtained from all patients.
Demographic data and neoplasm characteristics
Imaging procedures
All patients underwent pre-interventional arterial and venous phase multislice CT (Sensation 16, Siemens, Forchheim, Germany) within 3 days prior to the procedure. A standardized scan protocol was used as follows: collimation, 16 × 0.75 mm; tube voltage, 120 kV; effective tube current-time product, 160 mAseff; pitch, 1. Images were reconstructed with slice thicknesses of 5 mm and 2 mm with corresponding reconstruction increments of 4 mm and 1 mm, respectively. A medium smooth convolution kernel (B30f) was chosen for image reconstruction. Multiplanar reformats along the coronal and sagittal plane were computed from thin section axial images. For contrast enhancement 120 mL of contrast material (Ultravist 300, Bayer Healthcare, Leverkusen, Germany) was administered at a flow rate of 4.5 mL/s via an antecubital vein followed by a 30 mL saline chaser bolus. In all patients post-interventional CT scans were performed 1 day and 6 weeks after ablation using the same scan protocol. Thereafter follow-up CT scans were obtained every 6 months.
Radiofrequency ablation
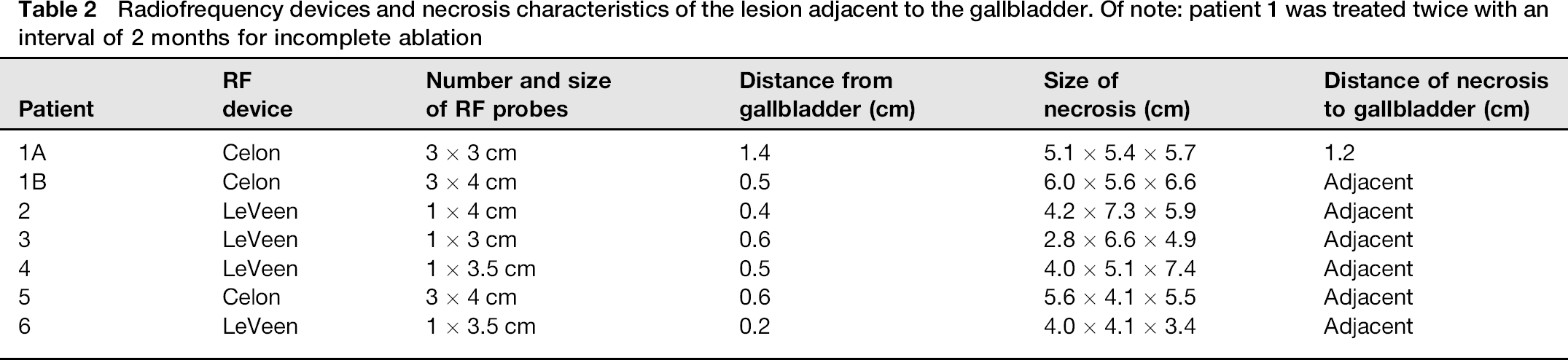
All procedures were carried out under general anesthesia using CT guidance. Two different radiofrequency devices were used for the ablation: the monopolar RF 3000 generator with umbrella-shaped LeVeen-probes (Boston Scientific, Natick, MA, USA) and the multipolar CelonPOWER system with needle electrodes (Celon, Teltow, Germany). The size of the probes was chosen according to the tumor size at the interventionalist's choice (Table 2). Energy was applied following the recommendations of the vendors.
Radiofrequency devices and necrosis characteristics of the lesion adjacent to the gallbladder. Of note: patient 1 was treated twice with an interval of 2 months for incomplete ablation
To protect the gallbladder from thermal damage CT-guided bile aspiration was performed in all patients immediately before ablation using a 20G or 22G fine needle. In four patients additional hydrodissection was performed. For hydrodissection a 20G fine needle with an end-hole was placed under CT-guidance between the liver capsule and the gall bladder. In this position 10–35 mL of 5% dextrose (n = 2), dextran (n = 1), or 0.9% saline (n = 1) mixed with contrast material (Ultravist 300, Bayer Healthcare, Leverkusen, Germany) were injected between the gallbladder and the liver parenchyma. Distribution of the fluid was monitored by repeated sequential CT scans. Injection was ended once a 5 mm distance between liver capsule and gall bladder was achieved.
Data analysis
Patients charts were reviewed for demographic data, type of tumor, and ablation parameters. The size of the lesions and the distance to the gallbladder were derived from pre-interventional CT scans. The lesion size was determined from axial images and multiplanar reformats along the coronal plane. The size of the necrosis and the distance of the necrosis from the gallbladder wall were measured on the first post-interventional CT scan. Side-effects and complications were derived from patient charts as well as the post-interventional and the 6-week follow-up CT scans.
Results
Three lesions were adjacent to the gallbladder, while the other three were located within 1.0 cm distance (range, 0.1-0.4 cm) from the gallbladder. Lesion sizes ranged from 1.4 × 1.1 × 2.1 cm to 3.8 × 4.8 × 4.9 cm (Table 1). In two patients pre-interventional CT revealed gallstones without signs of cholecystitis.
Ablation procedures were completed in all patients as planned. In one patient the ablation was incomplete and successful re-ablation was performed 2 months later (patient 1). In all other patients RFA was successful with a safety margin of at least 0.5 cm or to the liver capsule if there was less than 5 mm of parenchyma (Table 2).
There were no major complications. Minor complications occurred in three patients, including right-sided pleural effusion (n = 1), hematoma in the gallbladder bed (n = 1), and hemorrhage in the area of ablation (n = 1). The latter was associated with moderate abdominal pain and nausea. This patient underwent diagnostic angiography, which showed no signs of bleeding and the post-interventional course was otherwise uneventful. In one patient (patient 2) a small intramuscular abscess was detected at the puncture site at the 6-week follow-up. The patient was treated by i.v. antibiotics for 3 days (2 × 1.5 g/die cefuroxim) and the abscess was excised. The liver parenchyma was not affected and no further complications occurred. There was no cholecystitis or damage to the gallbladder during follow-up. The overall complication rate was 43%.
Discussion
RFA is regarded as a safe and effective treatment modality for a variety of primary and secondary hepatic malignancies. Its application, however, is limited by several factors such as lesion size and location. The distance of the area of the ablation to other structures as gallbladder or intestine is decisive for the efficacy of treatment with regard to incomplete ablation and frequency of complications (14). Cholecystitis with its typical signs as wall thickening and surrounding fat stranding or the rare perforation of gallbladder wall are possible complications after RFA of lesions close to the gallbladder (10).
In an in-vivo study in a pig model Lee et al. evaluated histolopathologic changes of the gallbladder wall in dependence of its distance from the treated lesion (12). RFA caused thermal damage of the gallbladder wall including delayed perforation up to 7 days after the RFA. The risk of developing a perforation increased with the decreasing distance of the RF-electrode to the gallbladder. The safe distance to the gallbladder for the RFA was claimed to be 1 cm (12). Another aspect which shows an influence on the rate of complications after RFA of lesions adjacent to gallbladder is the direction of the placement of the electrode. Perforation occurred more frequently if the electrode was placed parallel to the gallbladder (12). It has been hypothesized that bile-filled gallbladder could be helpful in reducing injury because of a possible thermal conduction effect dissipating heat from the wall (12,15).
In a case series including eight patients Chopra et al. analyzed the safety of RFA in tumors adjacent or within 1 cm from the gallbladder (13). In four patients (6/14 treatments) gallbladder wall thickening associated with pain was noticed. The symptoms were self-limited and required only analgesic medication. In one case, where the gallbladder wall was separated from the treated area by ascitic fluid, no gallbladder related complications were observed. The authors concluded that thermal damage from RFA causes mild cholecystitis (13).
To displace vulnerable structures from the area of ablation hydrodissection has been introduced (15,16). The vulnerable organ is separated from the target structure by creating a barrier by injecting a fluid. The use of 5% glucose, saline, or sterile water has been described (15–17). From theory glucose shows some advantages over saline and sterile water, as it does not conduct electric energy and is well-tolerated when injected intravenously or into body cavities. Saline is an ionic fluid, which on the one hand provides thermal protection by conducting heat away from the ablation zone, but on the other hand as an ionic fluid it will be heated by RFA potentially spreading heat. Nevertheless saline showed a protective effect in a previous study by Laeseke et al. (17) and did not cause a problem in this study. Sterile water as a non-ionic fluid does not conduct electricity, but due to its hypo-osmolar nature it may cause shifts in systemic fluid and should only be used in small amounts (17).
We hypothesized that bile aspiration increases the distance between the tumor and the gallbladder wall. Hydrodissection creates an additional distance and possibly dilutes the heat, thereby protecting the gallbladder itself (Fig. 1). In this case series bile aspiration with and without hydrodissection proved safe and effective and no gallbladder-related complication occurred, although in some patients the RF-probes were placed in parallel to the gallbladder. As different substances including dextran, 5% glucose, and 0.9% saline were used for hydrodissection, no conclusions on differences in fluid efficacy can be drawn. Interestingly sole bile aspiration was equally effective in this small series when performed without additional hydrodissection. As hydrodissection is more complex when compared to a simple fine-needle puncture of the gallbladder, the sole use of bile aspiration may help to shorten procedure time in selected patients.
A 49-year old female patient with liver metastasis from breast cancer. The lesion almost reaches the gallbladder wall with a distance of 0.1 cm (a). The lesion was treated using multipolar 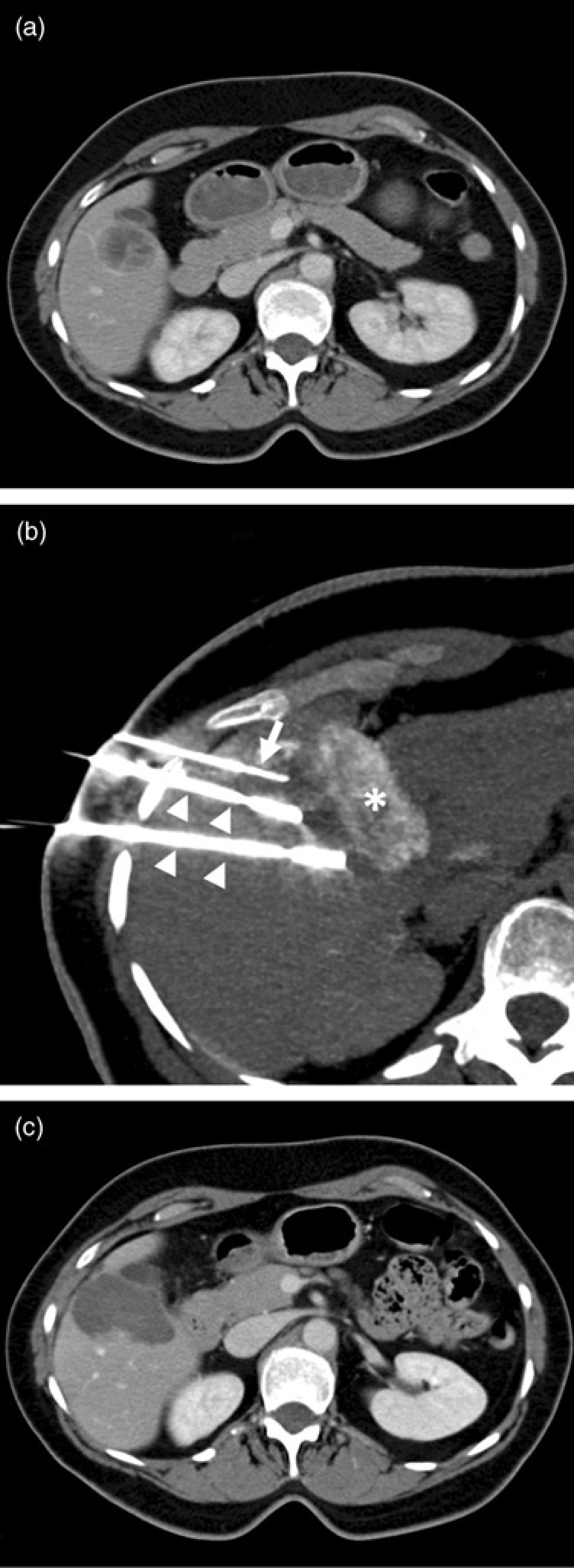
There are some limitations of this study. First, this is a small case series including only six patients. However, it supports data from previous reports and adds a new tool for protecting the gallbladder. Nevertheless, further data are needed to assess the efficacy of this approach. Second, different fluids were used to create a distance between gallbladder wall and tumor. Thus we cannot comment on advantages or disadvantages of a specific fluid, as the techniques were equally effective in all patients. Finally, different RF probes and generators were used. However, this reflects clinical routine practice and indicates the robustness of the technique of bile aspiration with or without hydrodissection.
In conclusion, the presented data indicate that bile aspiration with and without hydrodissection is a feasible technique for avoiding thermal damage of the gallbladder in RFA of liver lesions close to the gallbladder.