
Abstract
Background
Hybrid positron emission tomography/magnetic resonance imaging (PET/MRI) with simultaneous data acquisition promises a comprehensive evaluation of cerebral pathophysiology on a molecular, anatomical, and functional level. Considering the necessary changes to the MR scanner design the feasibility of arterial spin labeling (ASL) is unclear.
Purpose
To evaluate whether cerebral blood flow imaging with ASL is feasible using a prototype PET/MRI device.
Material and Methods
ASL imaging of the brain with Flow-sensitive Alternating Inversion Recovery (FAIR) spin preparation and true fast imaging in steady precession (TrueFISP) data readout was performed in eight healthy volunteers sequentially on a prototype PET/MRI and a stand-alone MR scanner with 128 × 128 and 192 × 192 matrix sizes. Cerebral blood flow values for gray matter, signal-to-noise and contrast-to-noise ratios, and relative signal change were compared. Additionally, the feasibility of ASL as part of a clinical hybrid PET/MRI protocol was demonstrated in five patients with intracerebral tumors.
Results
Blood flow maps showed good delineation of gray and white matter with no discernible artifacts. The mean blood flow values of the eight volunteers on the PET/MR system were 51±9 and 51±7 mL/100 g/min for the 128 × 128 and 192 × 192 matrices (stand-alone MR, 57±2 and 55 ± 5, not significant). The value for signal-to-noise (SNR) was significantly higher for the PET/MRI system using the 192 × 192 matrix size (P < 0.01), the relative signal change (δS) was significantly lower for the 192 × 192 matrix size (P = 0.02). ASL imaging as part of a clinical hybrid PET/MRI protocol could successfully be accomplished in all patients in diagnostic image quality.
Conclusion
ASL brain imaging is feasible with a prototype hybrid PET/MRI scanner, thus adding to the value of this novel imaging technique.
Simultaneous positron emission tomography (PET) and magnetic resonance imaging (MRI) with hybrid devices (PET/MRI) has become feasible with recent developments in PET detector technology, most notably the replacement of photomultiplier tubes (PMTs) by avalanche photodiodes (APDs) (1–7). Compared to whole-body devices the dedicated brain PET/MRI system evaluated in this work offers a notably better spatial resolution of the PET component that benefits imaging of small cerebral structures (8, 9).
The arterial spin labeling (ASL) technique for the measurement of cerebral blood flow with MRI (10, 11) would be a valuable complement to morphological imaging with MRI and molecular imaging with PET. A commonly applied ASL preparation is the Flow-sensitive Alternating Inversion Recovery (FAIR) scheme (10) that may be combined with true fast imaging in steady precession (TrueFISP) (12,13) and other techniques for data readout.
While being well established in stand-alone MRI systems (11, 14–16), ASL imaging may not work satisfactorily with hybrid PET/MRI devices dedicated to brain imaging. FAIR-ASL requires acquisition of images with global inversion of magnetization (in addition to slice selective inversion) which may be hampered by the spatially restricted excitation range of the radiofrequency (RF) pulses owing to the placement of the smaller transmit/receive coils inside the PET detector. Also the active electronic components of the PET system within the MRI field of view may interfere with MRI.
The aim of this study in eight healthy volunteers was to investigate the feasibility of ASL imaging with the BrainPET/MRI system using flow-sensitive alternating inversion recovery (FAIR) preparation and true fast imaging in steady precession (TrueFISP) readout and to compare signal-to-noise ratio, contrast-to-noise ratio, and relative signal change of the FAIR-TrueFISP sequence between the hybrid PET/MRI system and a corresponding MRI-alone 3.0T imager. Additionally, the feasibility of ASL imaging in a hybrid PET/MRI imaging protocol was demonstrated in five patients with intracranial tumors.
Material and Methods
Subjects and study design
Eight healthy volunteers (seven men, one woman; age range, 27-48 years; median age, 33 years) participated in the study. The volunteers underwent ASL imaging of cerebral blood flow under resting conditions with the 3T BrainPET/MRI prototype system and with a 3T stand-alone MRI scanner on the same day.
In addition, the inclusion of ASL in a clinical hybrid PET/ MRI protocol was demonstrated in five patients with intracranial tumors (1 × glioblastoma multiforme, 1 × anaplastic astrocytoma, 2 × low grade glioma, 1 × meningioma [two men, three women; age range, 30-73 years; median age, 54 years]) who had undergone PET/CT imaging with the radiotracers [11C]methionine (patients with gliomas) or with the somatostatin receptor ligand [68Ga]DOTA-D-Phe1-Tyr3-octreotide (DOTATOC) (patient with meningeoma) immediately prior to PET/MR scanning as previously described (17). Patients did not undergo additional stand-alone MR imaging.
The study was conducted according to institutional guidelines and was approved by the local ethics committee. Written informed consent was obtained from all subjects.
PET/MR imaging
MRI was performed on a hybrid PET/MRI system consisting of a small-bore PET system (BrainPET, Siemens AG, Erlangen, Germany; axial and transaxial fields of view: 19.1/32.0 cm) inserted into a slightly modified 3T whole-body MRI scanner (Magnetom Trio, Siemens AG, Erlangen, Germany; body-coil disconnected and patient table positioning altered) (7). A dedicated outer birdcage transmit/receive head-coil was used for spin excitation, which was combined with an inner 8-channel receive-only head-coil (Fig. 1) (18). This system's field of view is restricted to imaging of the head and upper neck area. The PET detectors were switched on throughout the data acquisition, in the case of the volunteers only recording random counts.
Image enlargement (ventral right part of the brain) of a parametrical ASL perfusion map showing typical region-of-interest (ROI) definitions for gray matter areas avoiding macroscopic vessels (yellow) and background noise (blue)
FAIR-TrueFISP imaging
For the volunteers participating in the study single-slice ASL blood flow images were acquired. The image plane was chosen to be parallel to the anterior commissure/posterior commissure (AC-PC) line and immediately cranial to the ventricles.
For the FAIR preparation, alternating global and slice-selective inversion pulses were applied. For the slice selective inversion, an adiabatic RF FOCI (frequency offset corrected inversion) pulse was used. Inversion time delay (TI) was set to 1.2 s, measured from the center of the pre-pulse for blood preparation to the first phase-encoding step. Four dummy preparation FAIR scans were applied before data acquisition in order to achieve a steady-state of tissue relaxation. Image slice thickness was 5 mm, the slice-selective inversion slab was 12.5 mm thick.
After FAIR spin preparation, image readout was performed with a true fast imaging (trueFISP) sequence with a repetition time (TR) of 4.0 ms, an echo time (TE) of 2.0 ms, and an acquisition bandwidth of 651 Hz/pixel. The time delay between subsequent TrueFISP image acquisitions was 5000 ms. Forty sets of FAIR images were acquired in 6:55 min. For the TrueFISP readout a filtered sinc RF pulse with duration of 1.0 ms, a bandwidth-time product of 5.11 and an excitation angle of 70° were used. An α/2 preparation prepulse and 12 prescans without data recording were performed. A centric-reordered k-space acquisition scheme was used for optimal blood flow contrast. The matrix sizes were 128 × 128 with an in-plane resolution of 2 × 2 mm and 192 × 192 with an in-plane resolution of 1.3 × 1.3 mm for a total field of view (FOV) of 256 × 256 mm. K-space filtering with a Hamming filter was employed to reduce Gibb's ringing. In addition, tissue equilibrium magnetization was measured with a conventional proton density weighted (PDw) TrueFISP sequence in order to measure tissue equilibrium magnetization for quantitative pixel-wise calculation of blood flow values.
Protocol for demonstrating feasibility of ASL in a clinical hybrid PET/MRI protocol
ASL images were acquired as described above to characterize the tumor in relation to presumed unaffected brain areas. Additional MR data-sets were recorded concurrently with the PET data acquisition as described earlier (17), comprising images for PET attenuation correction, fluid-attenuation inversion recovery (FLAIR) images, T2-weighted images and a magnetization-prepared rapid-acquisition gradient-echo (MPRAGE) image data-set. Contrast-enhanced imaging was precluded by the ethics approval.
Stand-alone MR imaging
Volunteers were imaged on a standard 3T MRI system (Magnetom Trio, Siemens AG, Erlangen, Germany) with the body-coil used for spin excitation and a 12-channel head-coil was used for signal reception. The ASL imaging parameters were transferred from the PET/MRI scanner to the stand-alone system immediately before scanning in order to ensure an identical parameter set between both scanners.
Data analysis
The quantitative blood flow maps were computed on a pixel-by-pixel basis according to the formula:

All images were visually inspected independently by two medical imaging experts in order to check for visible artifacts.
For the quantitative analysis of the grey matter blood flow and related image quality parameters, regions of interest (ROIs) were positioned on the calculated blood flow maps. Free-hand ROIs were drawn that covered 16–20 voxels of three representative grey matter (GM) areas per study, an additional ROI was placed on the image outside of the head for the measurement of background noise (Fig. 1). In addition to regional tissue blood flow several image quality parameters were computed: signal-to-noise ratio (SNR), defined as S/σnoise with S standing for the tissue signal intensity in the equilibrium magnetization images and σnoise standing for the standard deviation (SD) of the background signal; contrast-to-noise ratio (CNR), defined as (Ssel-Sgl)/σnoise, where Ssel and Sgl denote tissue signal intensities in the slices with slice-selective (sl) and global (gl) spin preparation, respectively; relative signal change was computed with δS = CNR/SNR. In the patient data an additional ROI was placed on the tumor with tumor borders estimated on morphological MR images.
Statistical analysis
Statistical analysis was performed using standard software (JMP 9; SAS Institute Inc., Cary, NC, USA). All mean values are given together with the standard deviation, unless stated otherwise. The ratios of the mean difference of paired measurements over their averages were calculated to test the agreement between the measurements with PET/MRI and stand-alone MRI according to Bland and Altman (20). The coefficient of variation (CV) between blood flow measurements on both systems (PET/MRI and stand-alone MRI) was calculated as the standard deviation of the differences divided by the mean blood flow of both measurements. The differences in blood flow, SNR, CNR, and δS were statistically evaluated using the Wilcoxon signed ranks test for paired data. P values below 0.05 were considered statistically significant. Bonferroni correction for multiple analyses was applied to the level of statistical significance in the case of SNR, CNR, and δS.
Results
Comparison between PET/MRI and stand-alone MRI
Visual inspection of the images of selective and global inversion using the FAIR spin labeling preparation and the calculated blood flow maps revealed no discernible artifacts in the PET/MRI derived images. An example of the obtained blood flow maps for both imaging systems from one male volunteer is shown in Fig. 2. Grey and white matter areas can be clearly distinguished in the blood flow maps, image quality of the PET/MRI system is comparable to that from the stand-alone system. Images for all volunteers (192 × 192 matrix size) are provided as electronic supplemental material (available at http://ar.rsmjournals.com/content/53/9/1066/suppl/DC1).
Blood flow maps acquired in one male volunteer on the 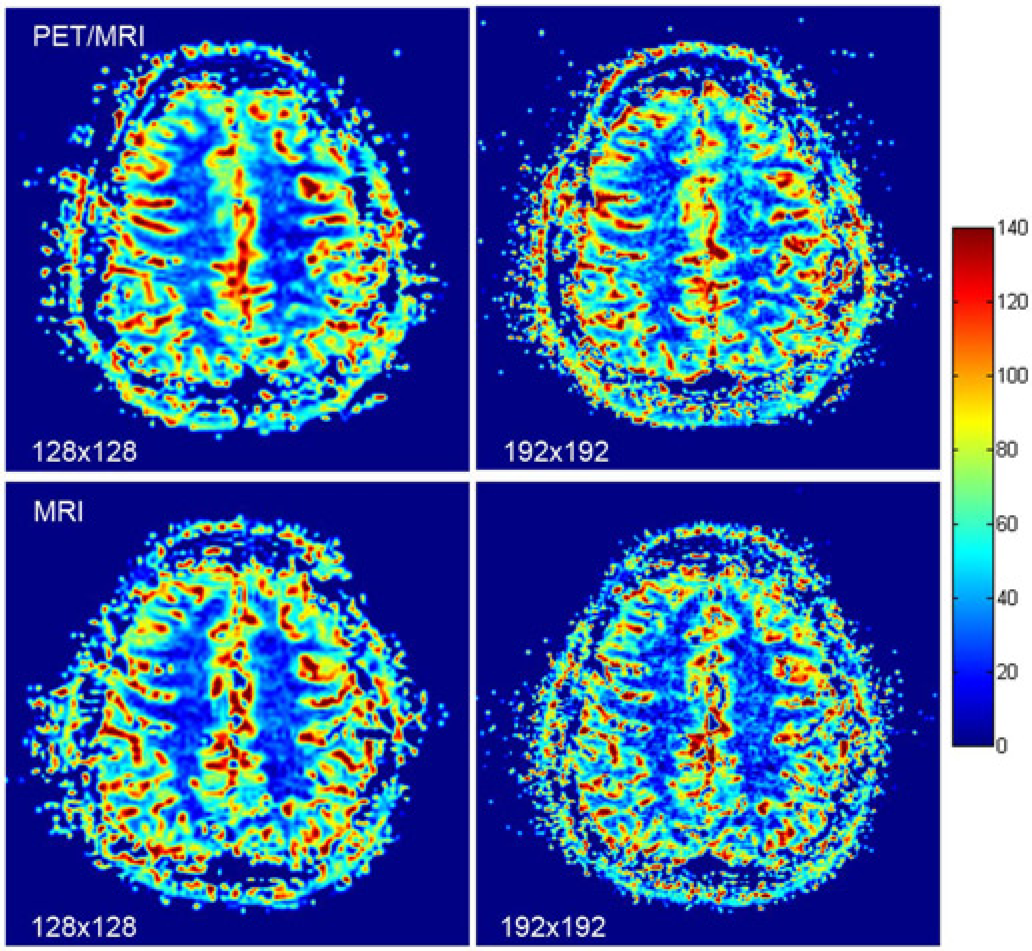
The mean blood flow for all eight volunteers on the PET/MR system was 51 ± 9 mL/100 g/min for the 128 × 128 matrix and 51 ± 7 mL/100 g/min for the 192 × 192 matrix. Corresponding values for the stand-alone MR system were 57 ± 2 mL/100 g/minute for the 128 × 128 matrix and 55 ± 5 mL/100 g/min for the 192 × 192 matrix. Mean values were lower for the PET/MR system for both matrix sizes; however, the differences were not significant (P = 0.15 and P = 0.11, respectively). In Fig. 3 scatter plots for the two blood flow measurements in the individual volunteers are shown; the differences in relation to their mean values are presented alongside. Upper and lower values of the 95% confidence interval were 13 and -1 mL/100 g/min for the 128 × 128 matrix and 9 and -1 mL/100 g/min for the 192 × 192 matrix size. The coefficients of variation (CV) were calculated as 16% and 12% for both matrix sizes.
Blood flow values in volunteers measured with the 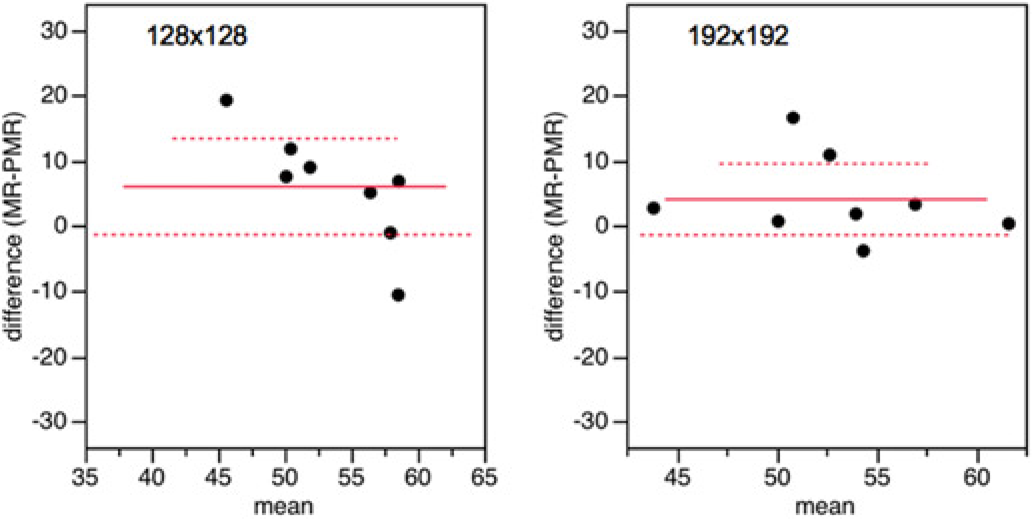
A comparison of the image quality measures SNR, CNR and δS for both systems is provided in Table 1). SNR was significantly higher in the PET/MRI data compared to the stand-alone MRI data for the 192 × 192 matrix size, even when the significance level was corrected for multiple analyses. A mild statistical trend towards higher CNR in the PET/MRI data was observed. The relative signal change δS was lower for the PET/MRI system, significance was reached only for the 192 × 192 matrix size.
Image quality measures:

P values are provided for PET/MRI vs. stand-alone MRI values
Demonstration of hybrid PET/MR imaging
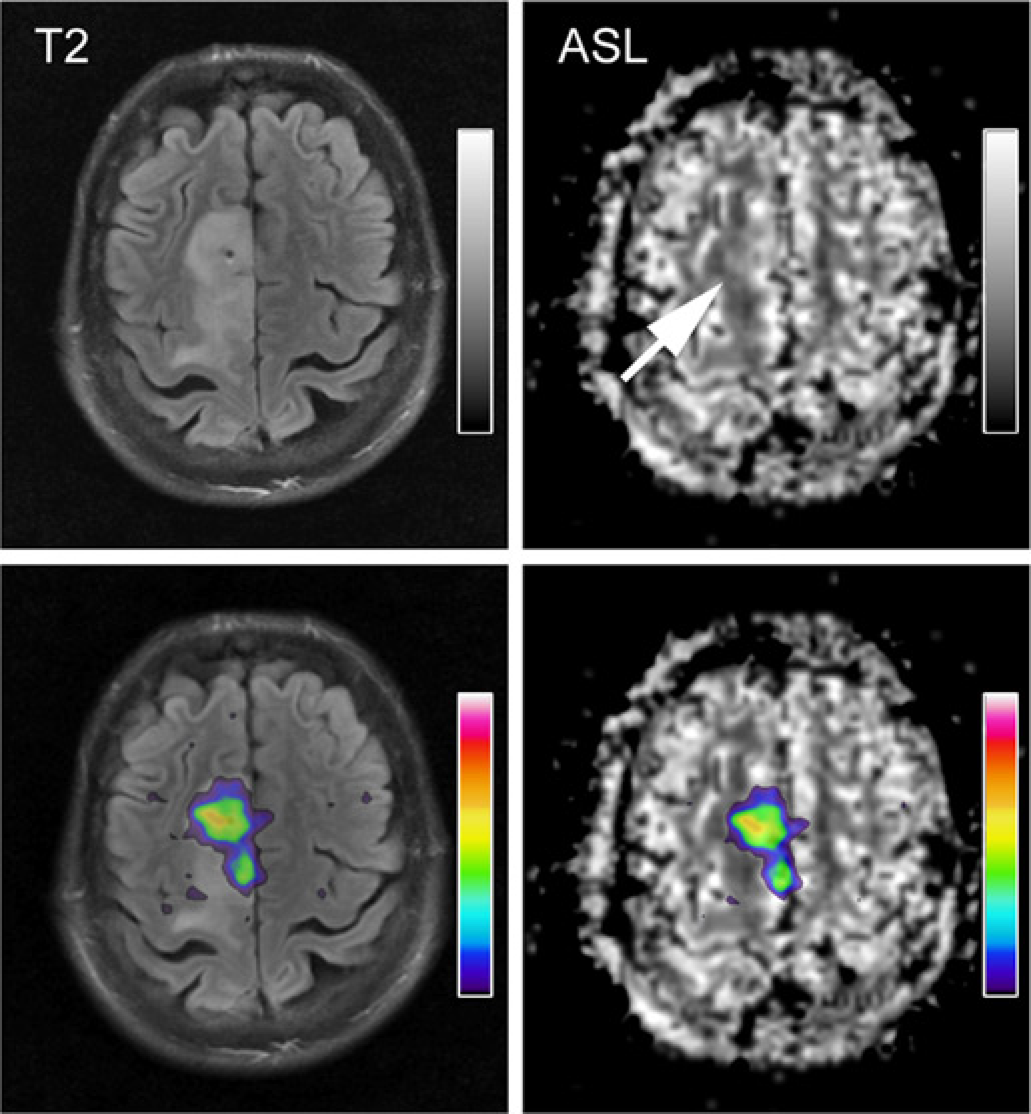
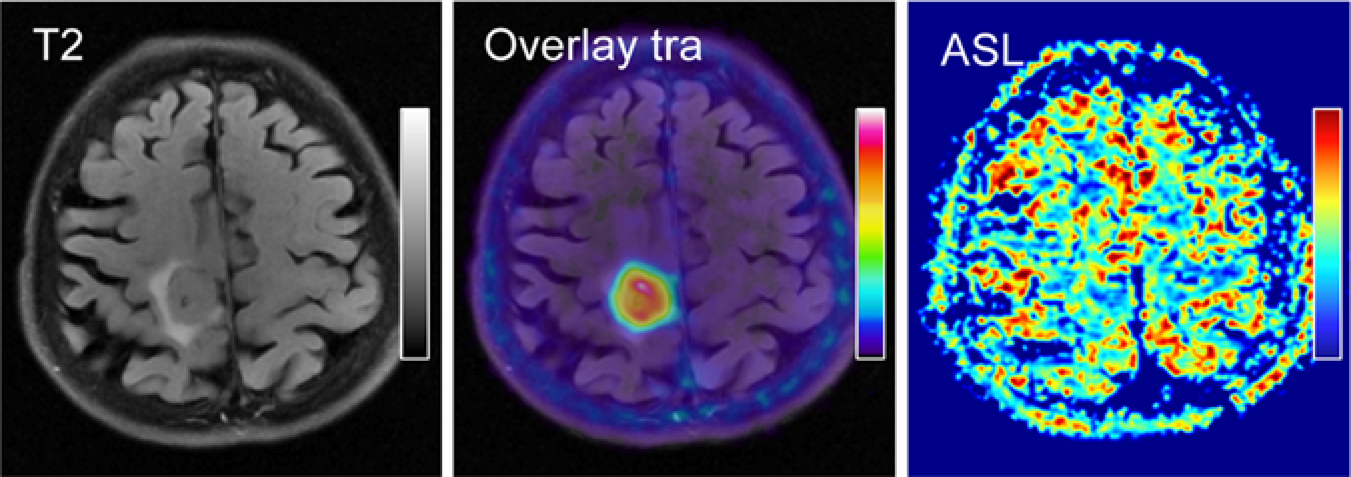
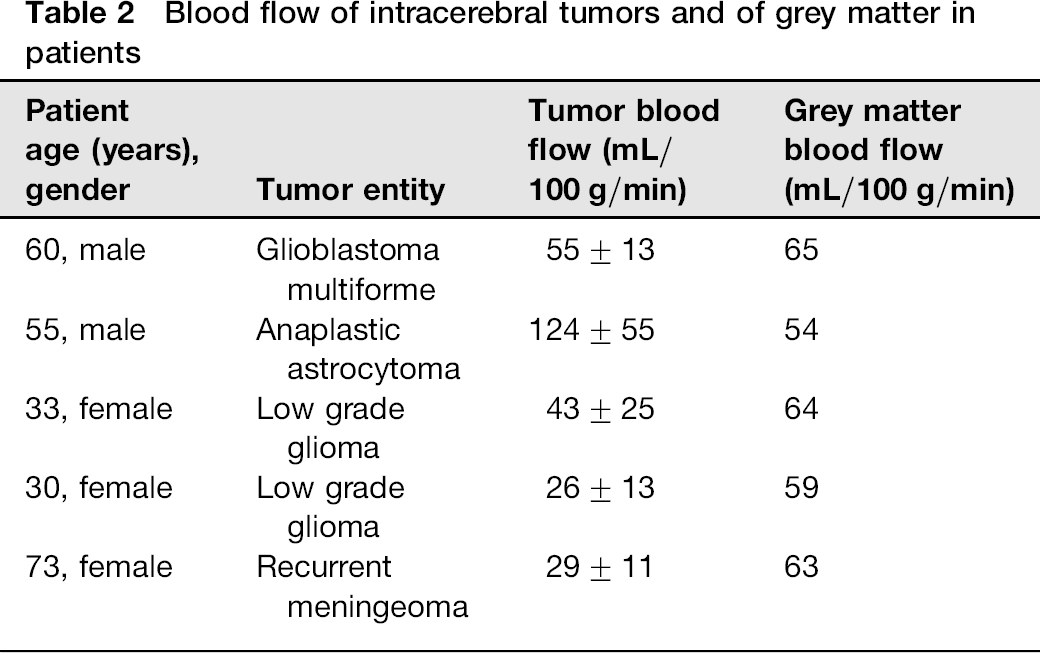
The tumor blood flow and the blood flow in presumed unaffected grey matter areas were successfully measured with ASL as part of a hybrid PET/MRI protocol with radiotracer uptake and morphological MR imaging in all patients (Table 2). In Fig. 4, images of a patient with glioblastoma multiforme are displayed. No obvious changes in the blood flow pattern obtained with ASL are visible in the areas with high methionine uptake. In Fig. 5, a patient with parafalxial meningioma is shown. The tumor exhibits high DOTATOC tracer uptake but a lower ASL-derived blood flow in comparison to grey matter areas.
Blood flow of intracerebral tumors and of grey matter in patients
Discussion
The results of the volunteer study comparing ASL with the PET/MRI and the stand-alone MR system show that cerebral blood flow analysis with ASL is indeed possible with the hybrid PET/MRI prototype without degradation in accuracy of blood flow quantification or signal yield. The feasibility of performing cerebral blood flow measurements with ASL is an important building block in establishing PET/MRI as a valuable tool for comprehensive molecular, anatomical and functional imaging of the brain.
No additional image artifacts were noticed on the PET/MRI-derived ASL images related to the additional hardware of the PET insert. The blood flow values recorded for the volunteers with the PET/MRI system were within the physiological range reported in previous publications on stand-alone systems, e.g. in Ref. 13. The grey matter blood flow values showed a trend towards higher values when measured with the stand-alone MR for both matrix sizes without being significant. The variation of blood flow values was within the range expected for test-retest settings in stand-alone MRI systems (21,22). Quantitative values obtained with this methodology for signal-to-noise and contrast-to-noise ratios compared favorably with the data from the stand-alone system. The cause for this improvement is likely to be found in the different receive coil setups in the two systems and not caused by the inserted PET system. The combination of an outer send/receive coil with an inner eight-channel receive coil has been chosen for the PET/MRI system because of the fact that the body-coils could not be used with concurrent PET imaging. As a side-effect this may have lead to improved reception in comparison to the 12 channel coil used in the stand-alone system. In order to separate the effect of the coil setup from the effect of the integration of a PET system, albeit not within the scope of this feasibility study, it would be possible to convert the hybrid PET/MRI system into a stand-alone MRI system by removing the PET component from the magnet and by using the built-in body-coil for transmission. This is avoided in our imaging laboratory in order to optimize the long-term stability and co-registration accuracy of the PET/MRI system.
We refrained from the measurement of T1 maps to avoid additional noise contribution but used literature values for the T1 of gray matter. This was previously introduced for stand-alone 3T MR systems and was not modified for use with the PET/MRI system.
The study was based on a hybrid PET/MRI prototype suitable for brain, head, and upper neck imaging and was currently limited to single-slice ASL using a FAIR-trueFISP sequence. This sequence type is known to be relatively robust regarding magnetic field inhomogeneities and eddy current induced artifacts (16), e.g. relevant when imaging near metallic implants. Several multi-slice approaches have been implemented, allowing coverage of a larger part of the head and upper neck area. This would be of benefit in the case of tumor heterogeneity or when dealing with brain pathologies with possible manifestations in different areas of the brain. However, such sequence types typically apply an echo-planar data readout strategy, which is more susceptible to imaging artifacts and is inferior regarding in-plane spatial resolution. It is likely that the FAIR-trueFISP ASL technique is less affected than methods using echo-planar imaging by interference with electronic PET components inside the MR magnet (e.g. increased eddy-currents during fast gradient-switching can lead to small image distortions as was previously shown for diffusion tensor imaging); the scale of this effect for ASL remains to be seen.
The FAIR ASL method uses alternating slice-selective and global spin inversion in order to calculate blood flow. Ideally, global spin inversion should cover a large area of the body in order to prevent non-inverted spins to reach the imaging plane between spin inversion and image acquisition. The restricted excitation range of the head coil used also for excitation in the PET/MRI system may adversely affect global spin inversion and may therefore reduce measured blood flow values. The results of this study, however, show that this effect is small enough.
With a hybrid PET/MRI system different methods for the evaluation of cerebral blood flow are feasible (23). Alternatively to ASL imaging using the blood as an endogenous, freely diffusible blood-flow tracer, MR imaging with exogenous tracers is possible, e.g. dynamic susceptibility-weighted MRI (DSC). This technique is a first-pass technique using gadolinium chelates as contrast agent, which allows for a fast determination of cerebral blood flow and blood volume, mean transit time, and vessel permeability. The need for contrast agent administration makes the technique more invasive and difficult to conduct in patients with renal impairment. Contrast material in larger vessels in the field of view can interfere with blood-flow imaging, whereas the effect is small for ASL. When using the PET component of the hybrid device for blood-flow imaging, water labeled with the positron emitter oxygen-15 can be used as a freely diffusible PET tracer. It allows for visual analysis of the cerebral blood-flow pattern and for exact quantification of cerebral blood flow and blood volume using biokinetic modeling. Instead of directly injecting radiolabeled water into the blood, C15O2 may be inhaled, which transfers the labeled oxygen to water once inside the blood. These PET techniques require, however, a cyclotron on stand-by in the proximity of the PET/MRI scanner to produce the oxygen-15 with a half-life of 2 min immediately before tracer administration and image acquisition; not a given for all imaging centers. Quantification involves determination of the arterial input function, an invasive procedure. Also dynamic PET imaging is needed. Imaging of slower biochemical processes with PET and the use of radiotracers with a longer half-life require dynamic PET imaging over a longer time period, which cannot be conducted at the same time as blood-flow imaging without interruption. Using the MRI instead of the PET component for blood-flow analysis may be more time efficient in a hybrid imaging set-up and in imaging protocols using other PET tracers.
The demonstration of a hybrid PET/MRI protocol in patients with intracranial tumors was intended to put ASL imaging into the wider context of hybrid PET/MR imaging. ASL complements molecular PET and morphological MRI in this setting and provides additional information about the tumor. The use of advanced MR techniques such as ASL but also diffusion tensor imaging (18) make the novel PET/MRI technique even more interesting for applications in the fields of clinical imaging and clinical research. Quantitative values for tumor and unaffected gray matter blood-flow obtained in these patients were in the range of previously reported results (24,25), noting a large heterogeneity of values in patients with the same tumor entity. In a first step it would be interesting to cross-calibrate PET-based and MRI-based methods for blood flow quantification. With simultaneous PET and MR data acquisition, the results from both modalities can be very well compared. In more advanced pathophysiological studies, the change of blood flow (measured with MRI) may be compared to changes in glucose or amino acid metabolism or in neurotransmitter/-receptor systems (measured with PET) for example.
In conclusion, quantification of cerebral blood flow with FAIR-TrueFISP arterial spin labeling MRI is feasible with hybrid PET/MRI devices. The possibility to use advanced MRI techniques concurrently with PET image acquisition makes the hybrid PET/MRI technology very interesting for many questions in basic research and clinical imaging of the brain.
Footnotes
Acknowledgements
We thank the staff of the cyclotron and radiochemistry facility of the University of Tübingen for provision of the radiopharmaceuticals. We cordially thank our colleagues Salvador Castaneda, Jonathan Cotton, Anna-Maria Rolle, and Christian Wenning for participation in the volunteer study. We also wish to express our gratitude to the other members of the PET/MRI research group, namely Matthias Reimold, Frederic Mantlic, Matthias Hofmann, Ulrike Ernemann, Thomas Nägele, and Heinz-Peter Schlemmer, for collaboration and scientific exchange. Financial research support was provided through the Deutsche Forschungsgemeinschaft (grants PI771/1-1 and PI771/5-1, and SFB 656 Münster, projects C6 and PM3) and the Swiss Werner Siemens-Foundation. Part of this work was supported by the Herzzentrum Münster e.V. (travel grant).