
Abstract
Background
Percutaneous coronary intervention (PCI) offers great benefit that could improve a patient's quality of life. However, numerous case reports of patient radiation injury resulting from PCI are being published, these reports likely represent a small fraction of the actual cases.
Purpose
To demonstrate the appropriate duration of patient follow-up after PCI to identify radiation effects.
Material and Methods
We evaluated 400 consecutive PCIs. The radiation dose (dose-area product, cumulative dose, maximum skin dose), number of cine runs, and fluoroscopic time were recorded for all patients. The skin on the patients’ backs was reviewed periodically after PCI.
Results
Radiation skin effects occurred in six patients from PCI of the right coronary artery in chronic total occlusion (CTO) patients (mild erythema; occurrence rate 1.5%). Skin injury in two patients appeared in cycles. In most cases, erythema was vividly seen at 4 weeks after PCI.
Conclusion
Careful observation for skin injury is needed. At a few days following PCI, early erythema can be detected through careful observation by well-trained staff. At 7-10 days after PCI, most erythematous pigmentation can be detected. At 4 weeks after PCI, most skin erythema appears clearly, however, some cases of skin erythema occur without back pain. After that, follow-up every 6 months is needed to detect the reappearance of erythema.
Percutaneous coronary intervention (PCI) offers great benefit that could improve a patient's quality of life. However, a major disadvantage of PCI is the patient radiation dose (1–15).
Although numerous case reports of patient radiation injury resulting from PCI are increasingly being published, these reports likely represent a small fraction of the actual cases. Radiation skin injury in PCI is overlooked clinically in many patients (16). Additionally, most reported cases do not include information on the patient's radiation dose (maximum skin dose, MSD) in PCI (2, 3, 6–10). We investigated 400 consecutive PCIs to evaluate the circumstances of patient skin injury.
The purpose of this study was to demonstrate the appropriate duration of patient follow-up after PCI to identify radiation effects.
Material and Methods
We evaluated 400 consecutive PCI procedures (315 men, 85 women); the patients averaged 67.9±10.5 years old (mean ± SD) and weighed 63.7±11.5 kg, including 56 for chronic total occlusion (CTO), conducted at Akita Medical Center (Japan) from December 2006 to November 2008 (Table 1).
Characteristics of our study
All data are mean ± SD, and minimum value – maximum value
CD, cumulative patient entrance dose (this X-ray system can evaluate DAP and CD); CTO, chronic total occlusion
PCI was performed using a digital cine X-ray system (Infinix Celeve-i, Toshiba, Japan) with 17-cm mode flat-panel detector (FPD), at an acquisition rate of 30 frames/s while applying pulsed fluoroscopy (15 pulses/s). Although the duration of the cine runs was inconsistent, a typical cine run lasted 3–4 s. A single-plane imaging system was used. The angles and views used while performing PCI were inconstant.
This X-ray system can evaluate the cumulative patient entrance dose (CD) and dose–area product (DAP) (17). The radiation dose (DAP, CD, and MSD), number of cine runs, and fluoroscopic time are recorded for all patients. The evaluation protocol for the MSD was described in detail in our previous study (17).
All patients undergoing PCI visited the outpatient care monthly for follow-up after the procedure. The physicians also examined the skin on the patients’ backs. If a patient had a symptom of radiation skin injury, topical ointments containing corticosteroids and antihistamines were used.
Specifically, betamethasone valerate 1%, gentamicin sulfate 0.1%, and diphenhydramine 1% were applied to the affected area twice daily. The three drugs were used for 2 weeks to alleviate the symptoms. However, if the patient continued to itch, diphenhydramine 1% was applied for approximately 1 month to treat the itching.
Furthermore, the relationships between patient skin effects and factors such as radiation dose were investigated. When a patient had a skin injury, we did not perform a biopsy to avoid further aggravation.
Results
Table 1 summarizes our results. For 400 PCIs, the incidence of CTO was 14%. No significant difference was detected between patients with and without CTO regarding age, height, and weight. The fluoroscopic time, number of cine frames, CD, and the DAP of patients with CTO were 2.5–3 times larger than those for non-CTO patients.
Six patients had radiation skin effects (mild erythema; occurrence rate 1.5%, Table 2). Figs. 1–3 show examples of radiation skin injuries (erythema) in our study. For these six patients, the mean ± SD CD, number of cine runs, and fluoroscopic time were 13.0 ± 0.64 mGy, 69.0 ± 16.4, and 149.2 ± 17.6 min, respectively. All cases of radiation skin injury in the present study arose from PCI of the right coronary artery (RCA) in patients with CTO and occurred on the right side of the back. The minimum value of the CD for skin injury in the current study was approximately 6 Gy.
Patient's back after PCI (68-year-old woman: body weight 66.4 kg, height 152 cm). (a) Main area of painful erythema at 6 weeks after PCI. (b, c) Painful erythema continued for 7–11 weeks after PCI. Recovery was gradual and the erythema continued to lessen
Patient's back after PCI (62-year-old woman: body weight 68.0 kg, height 162 cm). (a) At 3 days after PCI, early erythema (without pain) appeared. However, most medical staff could not point out the erythema because the skin changes were slight. (b) At 7 days after PCI, erythema continued and became worse. However, most medical staff could not point out the erythema. (c) At 10 days after PCI, mild erythema appeared. Most medical staff with careful observation could recognize the erythema. The main area of erythema with back pain and blistering was seen at 4 weeks after PCI (no photograph). Painful erythema continued for 5–10 weeks after PCI. (d) The erythematous pigmentation gradually became normal. (e) Erythema reappeared (with itching) at 11 months after PCI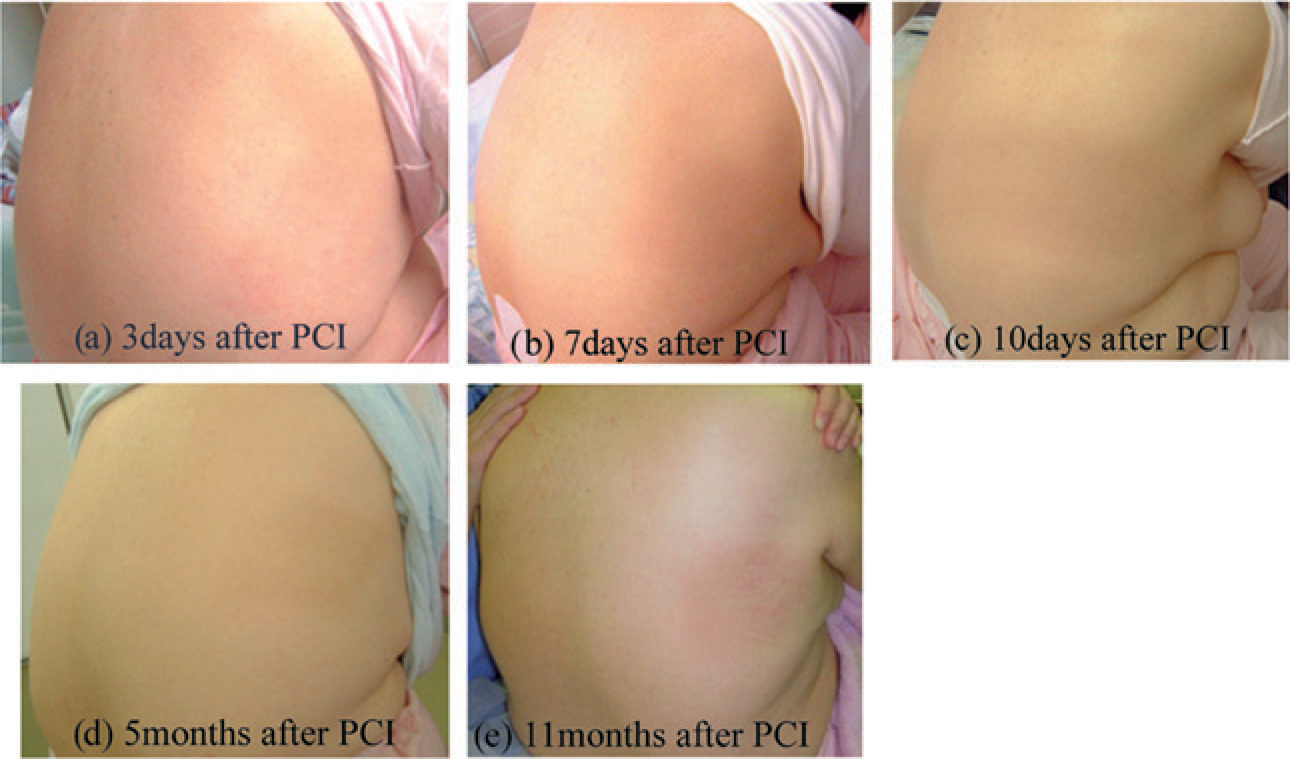
Patient's back after PCI (64-year-old man: body weight 61.4 kg, height 164 cm). (a, b) Erythema continued for 11–14 weeks after PCI. Erythema was present at 4 weeks after PCI. The patient's wife identified the erythema when she wiped his back with a towel, but observed no radiation skin injury because PCI had been performed 4 weeks previously and the visible skin effects did not immediately appear. The patient was unaware of erythema after PCI because of no pain.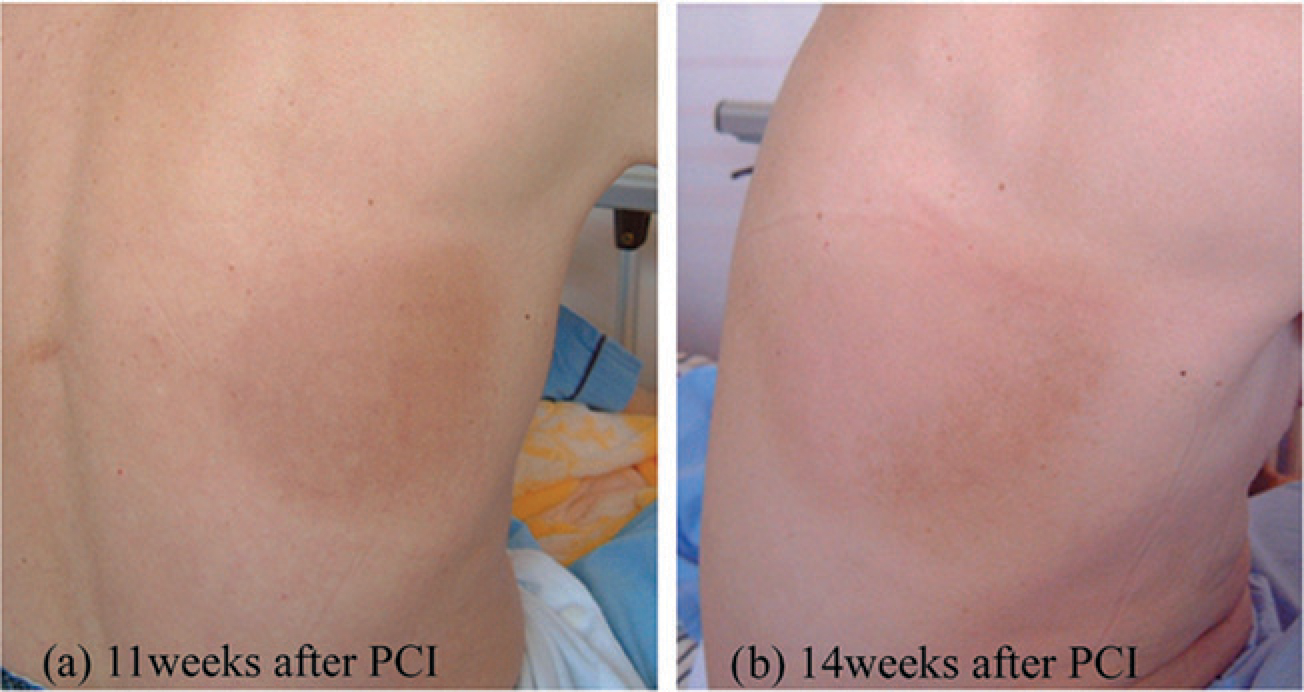
Summary of patient skin injury in this study (six cases of minor skin injuries)
Only one case (case 4) had undergone percutaneous coronary intervention in the same branch 3 months previously. At that time, the fluoroscopic time was 30 min and CD was 2.5 Gy
CD, cumulative dose; DAP, dose-area product; MSD, maximum skin dose; RCA-CTO, right coronary artery-chronic total occlusion
The progress of skin injury in six patients is summarized in Fig. 4. Skin injury in two patients (cases 2 and 5) appeared in cycles. Two patients (cases 4 and 6) experienced no pain. In most cases, erythema was observed at 4 weeks after PCI, but the patients were unaware of erythema during this time. Well-trained and experienced medical staff could detect early erythema at 3 days after PCI (case 5).
Summary of the progress of skin injury in six patients. Skin injury in two patients appeared in cycles. Two patients experienced no pain. In most cases, erythema was seen at 4 weeks after PCI. However, the patients were unaware of the erythema during the 4 weeks after PCI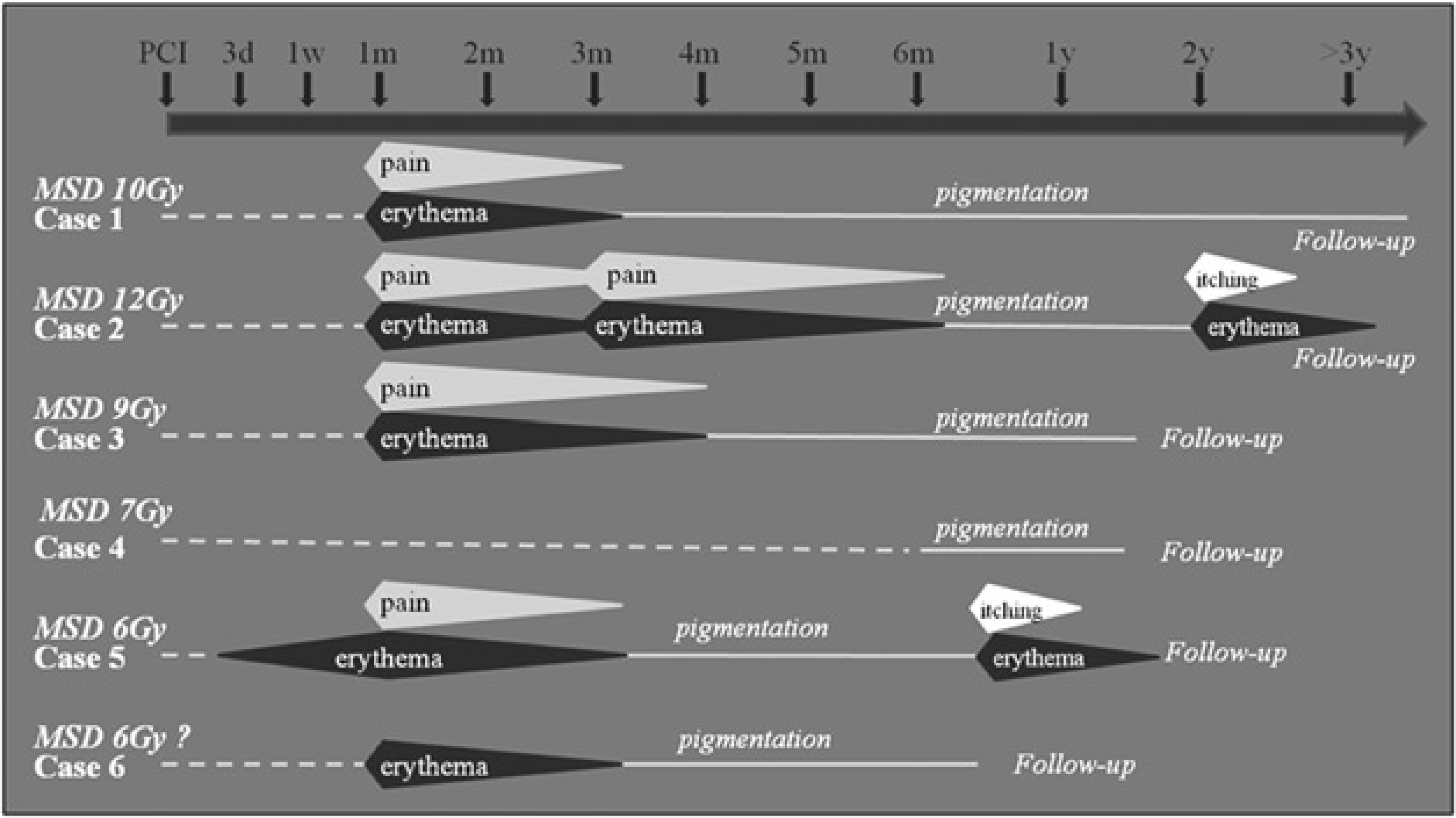
Discussion
Balter (18) reported that prompt reactions occur less than 2 weeks after irradiation, and stated that very few reports have described promptly developing symptoms following fluoroscopically guided interventional procedures. Thus, we investigated skin injury, including prompt reactions, in PCI.
Radiation skin injury does not become apparent for hours to days following exposure. Injuries (burns and other skin effects) tend to appear in cycles, depending on the radiation dose. Early treatment is important, and the use of medication (antihistamines and antipruritics) might prevent or attenuate initiation of the cycle (19). Therefore, early diagnosis (detection) is required, although it is currently difficult.
Even for mild prompt reactions, the risk of future carcinogenesis should be considered, particularly in patients likely to undergo repeated procedures. Thus, identification of prompt skin reactions after PCI is important.
Padovani (20) reported that the frequency of skin injuries in patients undergoing a cardiac procedure was 0.03%. Although mild erythema occurred, we observed six cases (1.5%) of radiation skin injury in 400 consecutive PCIs. The occurrence rate of skin injury in our study was higher than previously reported. One cause may be that our study had many CTO cases (associated with difficulty in advancing the catheter and guide wire). Hence, the fluoroscopic time of PCI for CTO tended to be longer, consequently prolonging irradiation, which can result in absorbed radiation doses that exceed the safe threshold for skin. Another cause for our higher rate may be that previous studies overlooked radiation skin injury in many patients.
Some cases of skin injury occur without back pain. Detecting early erythema is difficult because the skin changes are slight. Erythema is not observed for hours to days following PCI. Most skin changes appear clearly at about 4 weeks after PCI, and the connection with PCI is not made or the pathology is initially attributed to other factors. Moreover, self-recognition of changes to the back skin is difficult.
Follow-up of skin injury is necessary because patients may face an increased risk of future cancer. The minimum value of the CD for skin injury in the present study was about 6 Gy. Careful observation for skin injury is thus needed, particularly when the CD exceeds 6 Gy.
At a few days following PCI, early erythema can be detected through careful observation by well-trained staff (case 5). At 7–10 days after PCI, most erythematous pigmentation can be detected. At 4 weeks after PCI, most skin erythema appears clearly. After that, follow-up every 6 months is needed to detect the reappearance of erythema (in cycles).
When PCI is repeated, re-irradiation of the skin may significantly increase the probability of radiation effects, although the dose administered in any one PCI session might be insufficient to cause such effects. Therefore, physicians should seek to establish whether a patient has had previous PCI, together with the entrance site and estimated skin dose.
To reduce radiation skin injury, quality control of X-ray equipment, particularly the radiation dose, must be managed (21,22). Furthermore, different projections should be used to avoid exposure to one skin area throughout the whole procedure, and the irradiated area should be kept as small as possible (1). This indicates that collimation can reduce the accumulated dose to the skin by eliminating the overlap of fields when different beam angles are used.
Additionally, taking practical steps to reduce the radiation dose, such as using a lower dose mode, lower recording speed, and additional spectral beam filter, is necessary.
In conclusion, the rate of patient skin injury in PCI was higher than that described in many published reports. Therefore, radiation skin injury in PCI is overlooked clinically in many patients. Early medication for skin injury might prevent or attenuate initiation of the cycle that leads to the manifestation of skin injury, and early diagnosis is important. The minimum CD value for skin injury in the present study was about 6 Gy. Careful observation for skin injury is thus needed, particularly when the CD exceeds 6 Gy, in which case all patients can use topical ointments containing corticosteroids and antihistamines.
Footnotes
Acknowledgments
The authors thank Kyouhei Yoshida, Fumiaki Sasaki, and Masafumi Sasaki from the Department of Medical Technology, Akita Medical Center, for helpful advice regarding the technical analysis.