
Abstract
Background
Stent occlusion by tumor ingrowth or overgrowth is the main cause of jaundice recurrence after metal stent insertion in patients with malignant obstructive jaundice (MOJ). The application of intraluminal brachytherapy (ILBT) in patients with MOJ results in local control of malignant tumors, which prolong stent patency.
Purpose
To evaluate the safety of ILBT in pig bile ducts using ribbons of iodine-125 (125I) seeds.
Material and Methods
Sixteen healthy pigs were randomly assigned to four groups of four pigs each. A 125I seed ribbon was implanted into the common bile duct of each animal through an incision in the duct wall, and was fixed by suturing. The four groups of animals were sacrificed at 15, 30, 60, and 120 days after ribbon implantation, respectively. Serum bilirubin concentrations, alanine aminotransferase concentrations, and white blood cell counts before and after implantation were compared within each group. Pathological changes to the bile duct wall were observed using a light microscope. Morphological changes in biliary epithelial cells and organelles were observed with electron microscopy.
Results
125I ribbons were successfully implanted in all animals without surgery-related death. We found no significant difference in pre- and post-implant serum bilirubin, alanine aminotransferase, or white blood cell counts. Light and electron microscopy showed that the most severe bile duct damage occurred in the 15-day group, which exhibited necrosis and detachment of numerous epithelial cells, and infiltration of inflammatory cells. Repair and proliferation of the bile duct epithelium began 30 days after implantation and was nearly complete at 60 days.
Conclusion
This study demonstrated the safety of ILBT using a 125I ribbon in the pig bile duct. 125I seed ribbons may be used in the treatment of MOJ in humans.
Biliary stent placement has the advantages over endoprosthesis of minimal invasion, efficient drainage, and a low displacement rate. It has become the primary treatment modality for unresectable malignant obstructive jaundice (MOJ) (1–5). However, stent blockage caused by tumor progression will result in recurrent jaundice (6), which reduces patient survival and quality of life. Therefore, a major concern following biliary stent placement is the prevention of blockage by tumor progression to delay jaundice recurrence and improve treatment outcomes.
Radiation therapy may have an effect on most tumors that cause MOJ. External radiation is widely used, but its results are limited by the tolerance of anatomical structures (liver, duodenum, stomach, and kidney) around the lesion, the lack of clear lesion definition, the poor clinical status of patients, and the interference of respiration with the radiation field. As a form of brachytherapy, intraluminal irradiation can be used to deliver high doses of radiation to nearby tumor tissue while sparing more distant normal tissues. Intraluminal brachytherapy (ILBT) is a form of con-formal radiotherapy, and because the radiation source can be applied directly to the tumor, unintentional absorption of radiation due to patient movement can be reduced (7). Studies have shown that the use of ILBT in MOJ treatment results in local control of the primary tumor, delayed stent obstruction, and improved patient survival (8, 9). A high-dose-rate (HDR) iridium-192 (192Ir) source is commonly used in ILBT for cholangiocarcinoma obstruction (10). The advantages of HDR-ILBT include: (i) short treatment time that is readily accepted by the patient; (ii) negligible radiation dose to staff due to a separate treatment room and control area; and (iii) precise computer-controlled source dwelling position that reduces the uncertainties of manual source placement. Improper HDR fractionation, however, may induce severe late radiation complications in normal tissues.
192Ir ILBT requires a dedicated HDR afterloading system and a shielded treatment room. This procedure also requires significant capital investment by medical institutions, well-trained medical physicists, and a stable supply of 192Ir. For these reasons, a limited number of HDR units are currently installed in China, restricting the application of HDR-ILBT. Compared with HDR, ILBT using iodine-125 (125I) seeds is a more feasible option for many Chinese hospitals.
Since Whitmore (11) first performed retropubic 125I seed implant brachytherapy for prostate cancer treatment in the early 1970s, 125I seeds have been widely used in clinical tumor treatment and 125I brachytherapy has become the preferred method for local treatment (12). Permanent 125I seed implantation is currently the first-line therapy for selected patients with prostate cancer (13). Interstitial 125I seed brachytherapy has also been used to treat pancreatic cancer (14, 15), lung cancer (16, 17), and pediatric low-grade gliomas (18). This treatment modality has the following advantages over conventional external beam radiation therapy (19): (i) improved dose ratio between the target volume and normal tissue; (ii) continuous radiation to reduce tumor repopulation; (iii) reduced oxygen enhancement ratio and radioresistance of hypoxic tumor cells; and (iv) high dose conformity to treatment volume. The 59.6-day half-life of 125I allows convenient shipment and storage, the low-energy radiation is easily shielded with thin lead foil, and the 125I seed implant does not require a specialized loading facility.
In this study, we thus attempted to replace the HDR 192Ir source with a ribbon of 125I seeds in bile duct brachytherapy. We evaluated the safety of ILBT using a 125I seed ribbon in a pig bile duct, and collected data relevant to the clinical application of a 125I ribbon in patients with MOJ. We proposed that MOJ treatment could be performed by placing a ribbon of 125I seeds in the bile duct of a human subject through a drainage catheter. For this purpose, we developed a technique of loading and sealing 125I seeds in a catheter to form a linear ribbon that could serve as the brachytherapy source in the bile duct.
Material and Methods
Experimental animals
Sixteen healthy pigs (eight males, eight females), aged 4–6 months and weighing 40–50 kg, were provided by the Experimental Center of Zhongshan Hospital, Fudan University, Shanghai, China. The hospital issued an experimental animal permit (No. syxk(Hu)20080039) and maintained the animals in its facility.
Assembly of 125I ribbon
The 125I seeds (Model 6711; Junan Pharmaceutical Technology Co., Ltd., Ningbo, China) had cylindrical titanium alloy shells measuring 4.8 mm in length and 0.8 mm in diameter. 125I radiation consists of 35.5-keV gamma rays, 27.4-keV and 31.5-keV X-rays, with a half-value layer of 0.025 mm in lead and 20 mm in soft tissue. The initial apparent activity of a 125I seed is 25.9 MBq, with an initial dose rate of 8.89 mGy h–1. To make a 125I ribbon, five 125I seeds were loaded consecutively into a 4 Fr catheter (Boston Scientific Co., Ltd., Natick, MA, USA) with a sealed head end, and the tail end of the catheter was then sealed using thin strips of gelatin sponge to prevent seed displacement (Fig. 1).
125I seeds (black arrow) were consecutively loaded in a 4 Fr catheter with the head end sealed. The tail end of the catheter was then sealed using gelatin sponge strips (black arrowhead)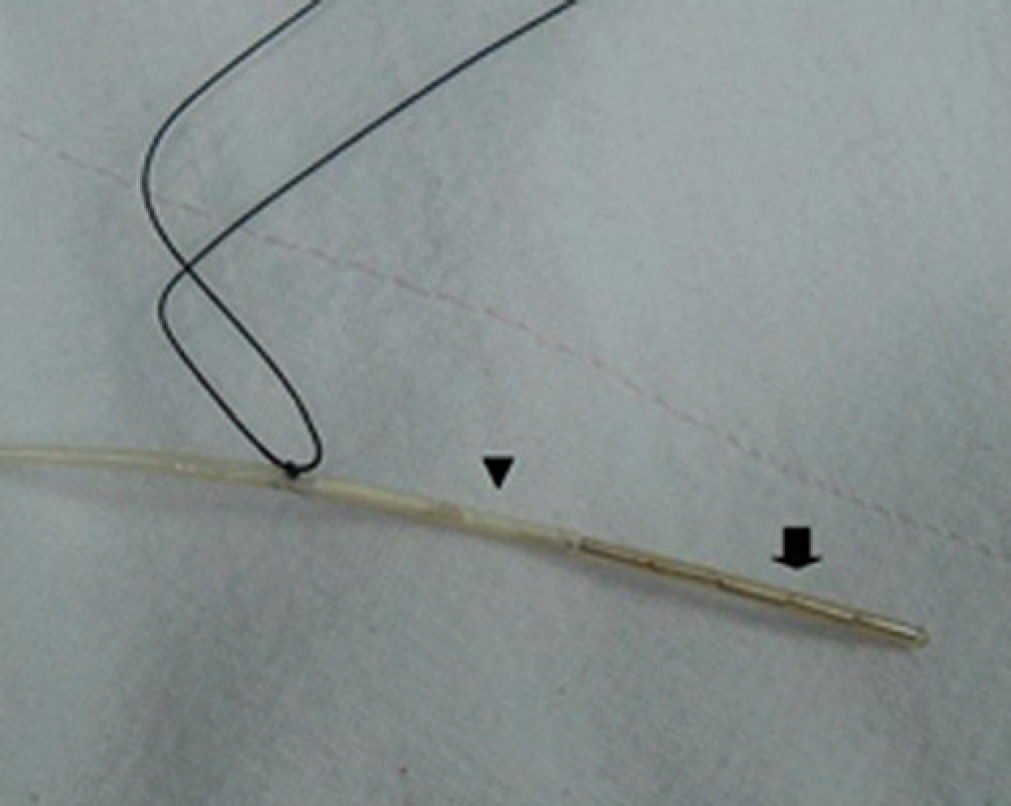
Implantation of 125I ribbon
The 16 experimental animals were randomly assigned to four groups of four animals. The animals fasted for 12 h and were weighed before surgery. Each animal was anesthetized with an intramuscular injection of diazepam (2 mg kg–1), ketamine (25 mg kg–1), and sumaxin (0.1 mL kg–1), and immobilized in a supine position on the operating table. The skin was disinfected using regular disinfection pads, and an indwelling peripheral venous catheter was placed. An incision was made through the wall of the right upper abdomen, the abdominal cavity was opened, and the hepatoduodenal ligament and upper common bile duct were exposed. An incision (1–2-mm width) was made on the common bile duct, and a 125I seed ribbon was advanced into the duct through the incision (Fig. 2). The 125I ribbon was fixed by suturing with silk thread. Anesthesia was maintained during surgery through the intravenous administration of diazepam (10 mg), ketamine (100 mg), and saline (20 mL).
An incision was made in the common bile duct (white arrow) of a pig to implant the 125I ribbon (white arrowhead)
After surgery, the animals fasted for 24 h before normal feeding was resumed under standard conditions. In the first 3 days following surgery, intramuscular injections of sodium penicillin (1.6 million units) were administered daily to prevent infection.
Sample collection
The four groups of animals were sacrificed at 15, 30, 60, and 120 days after 125I seed ribbon implantation, respectively. Each animal was weighed prior to the procedure, and venous blood samples were extracted for routine blood and liver function tests. After muscular anesthesia using diazepam, ketamine, and sumaxin, a 4 Fr catheter was inserted percutaneously into the gallbladder. Cholangiography was performed via the catheter to detect any displacement of the I ribbon (Fig. 3). The abdominal wall was incised layer by layer to expose the hepatoduodenal ligament and common bile duct. The portion of the bile duct treated with the I ribbon was excised and visually examined for ulceration, perforation, or stenosis of the bile duct lumen. Within 2 min of excision, a 1 × 1-mm sample was taken from the bile duct location corresponding to the midpoint of the 125I ribbon and fixed with 2.5% glutaraldehyde for electron microscopy. A 5-mm long sample was then taken from the bile duct location corresponding to the midpoint of the 125I ribbon and fixed with 4% formaldehyde solution for light microscope observation. After sample collection, the animal was immediately euthanized and the 125I seeds were stored in lead pigs.
Percutaneous gallbladder cholangiography was performed before sample collection, showing the common bile duct (white arrow) and the 125I ribbon (white arrowhead)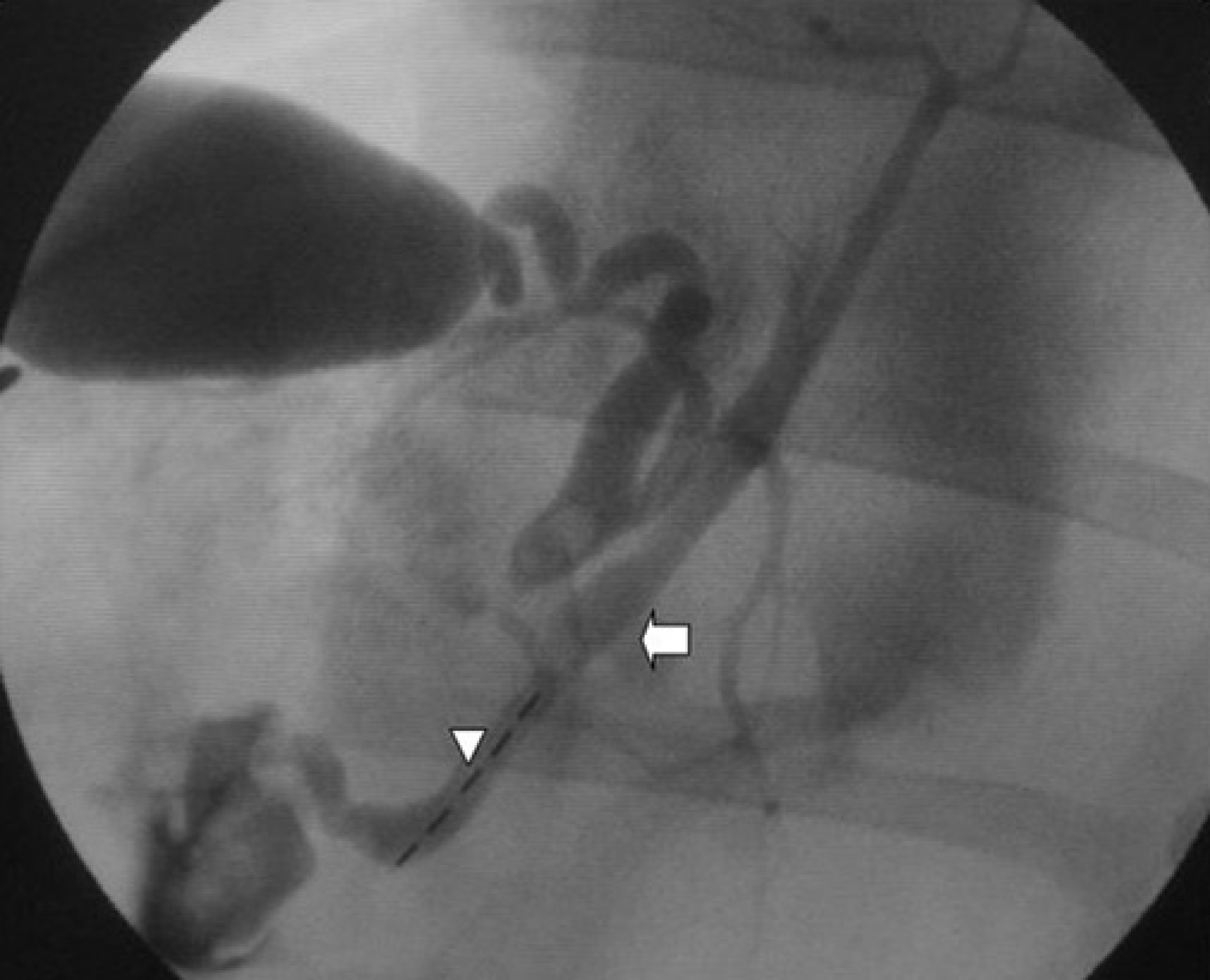
Absorbed dose calculation
The tissue absorbed dose of each subject group was calculated for a point 3 mm transverse from the midpoint of the 125I ribbon, corresponding to the radius of the pig bile duct. 125I Radiation Field Distribution Calculation software (version 0.1; Institute of Radiation Medicine, Fudan University) was used to calculate radiation doses.
Sample examination
Serum bilirubin concentrations, alanine aminotransferase concentrations, and white blood cell counts before 125I ribbon implantation and at the time of sample collection were compared. The bile duct samples were observed under a light microscope to assess epithelial necrosis or detachment, capillary dilatation and congestion in the lamina propria, infiltration of inflammatory cells, and fibroplasia. The samples were observed under an electron microscope to assess morphological changes in the epithelial cells, nuclei, and radiosensitive organelles (mitochondria, endoplasmic reticulum).
Statistical analysis
Statistical analyses were performed using SPSS® software (ver. 13.0; SPSS Inc., Chicago, IL, USA). Quantitative data were compared using paired-sample t-tests and are presented as means ± standard errors. P values <0.05 were considered statistically significant.
Results
Absorbed dose
The absorbed doses in tissue 3 mm from the midpoint of the longitudinal axis of the 125I ribbon were 51.5 Gy in the 15-day group, 94.8 Gy in the 30-day group, 161.7 Gy in the 60-day group, and 242.3 Gy in the 120-day group.
General animal conditions
The 125I ribbons were successfully implanted in all animals with no surgery-related death. No vomiting, diarrhea, or melena was observed after surgery. The surgical incisions healed without infection or necrosis. No death occurred between surgery and sample collection, and the weight of the animals increased by varying degrees.
Peripheral hemogram and liver function
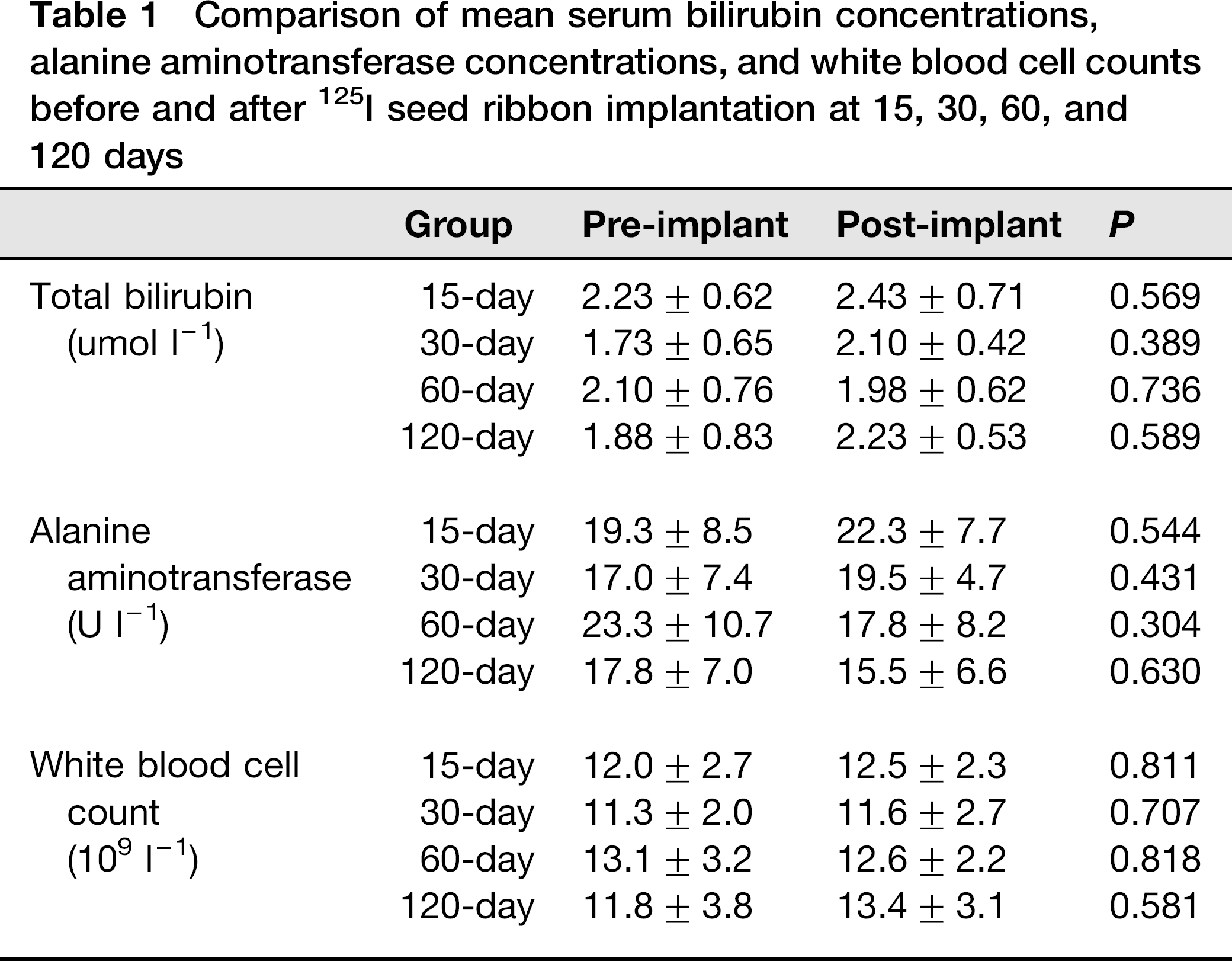
We found no significant intragroup difference in mean serum bilirubin concentration, alanine aminotransferase concentration, or white blood cell count before and after 125I seed ribbon implantation (Table1).
Comparison of mean serum bilirubin concentrations, alanine aminotransferase concentrations, and white blood cell counts before and after 125I seed ribbon implantation at 15, 30, 60, and 120 days
Visual examination
No displacement of the 125I ribbons or dislodgement of the 125I seeds was observed during sample collection. No thickening, ulceration, or perforation of the bile duct wall or stenosis of the bile duct cavity was observed.
Light microscope observation
The following conditions were found in tissue samples from the 15-day group: incomplete epithelium, detachment of numerous epithelial cells, irregular residual epithelial cells with unclear cytoplasm, epithelial cell atrophy (Fig. 4a), and abundant inflammatory cell infiltration. No obvious capillary dilatation or congestion was observed in the lamina propria. Samples from the 30-day group exhibited moderate epithelial cell loss, columnar cells with mucilage in the epithelium, and, as in the 15-day group, abundant inflammatory cell infiltration but no obvious capillary dilatation or congestion in the lamina propria (Fig. 4b). The following were observed in samples from the 60-day group: obvious proliferation of disordered epithelial cells, increased cell volume with columnar shape, large amount of mucus in the cytoplasm (Fig. 4c), and reduced inflammatory cell infiltration in the lamina propria relative to the 30-day group. Samples from the 120-day group exhibited obvious regeneration of the epithelium (in part due to papillary hyper-plasia), epithelial cells that had recovered their cuboidal shape, no obvious inflammatory cell infiltration, and a small amount of fibroplasia in the lamina propria (Fig. 4d).
Observation of bile duct wall samples from (a) the 15-day group, (b) the 30-day group, (c) the 60-day group, and (d) the 120-day group under a light microscope (100 ×)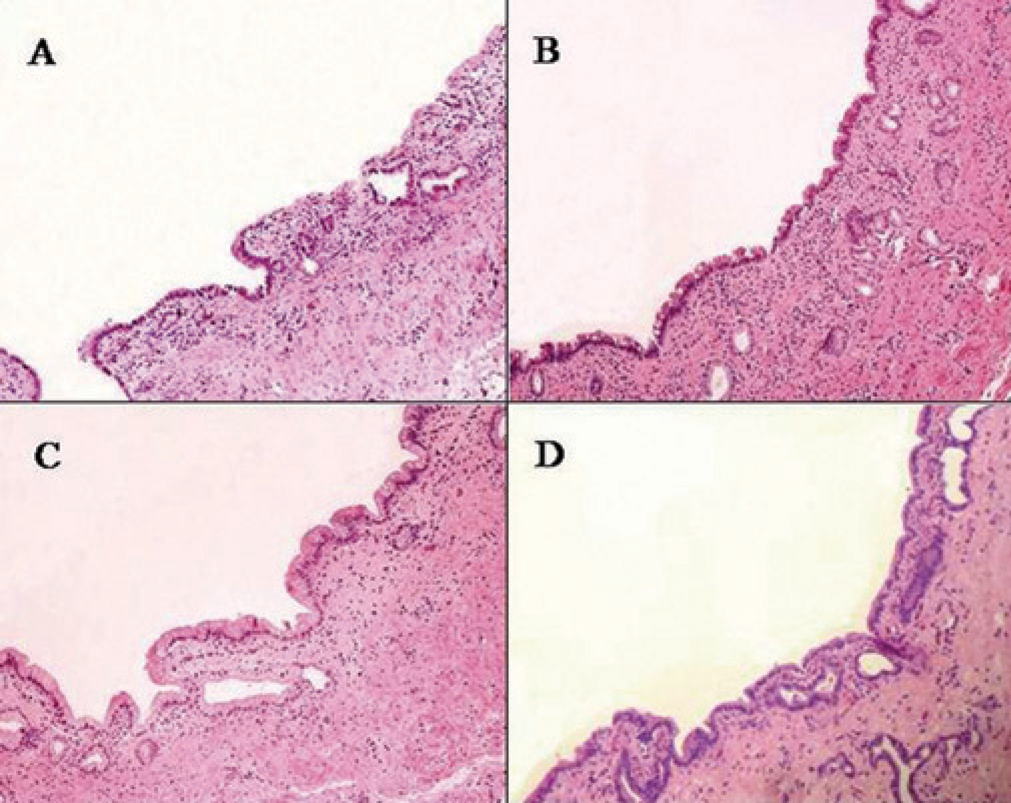
Electron microscope observation
Epithelial cell swelling, considerable loss of microvilli, and sparse nuclear chromatin were observed in tissue samples from the 15-day group. These samples also revealed mitochondrial swelling, blurred cristae, and swelling and vacuolization of the endoplasmic reticulum (Fig. 5). Samples from the 30-day group showed partial loss of microvilli and less mitochondrial swelling and endoplasmic reticulum expansion than in the 15-day group. Complete microvilli with clear forms, mild mitochondrial swelling and endoplasmic reticulum expansion, and large quantities of secretory granules in the cytoplasm were observed in samples from the 60-day group. Samples from the 120-day group showed complete microvilli with clear forms, no abnormality in the nuclei, mitochondria, or endoplasmic reticulum, and no secretory granules in the cytoplasm.
A sample from the 15-day group under an electron microscope (11,000×)
Discussion
Given the small dimensions and volume of 125I seeds, the key to successful treatment is proper fixation in the treatment area after implantation in the lumen without dislodgement or displacement. Some investigators have implanted 125I seeds in the lumen by loading them onto a metal stent or endoprosthesis, which prevents the operator from conducting brachytherapy while opening the obstructed duct. Guo et al. (20) used a self-expandable stent loaded with 125I seeds to treat advanced esophageal cancer. After 2 months of 125I treatment, the patients showed significant improvement in swallowing function and significantly increased median survival times, relative to those who received stent placement without brachytherapy. Because the diameters of the esophagus and esophageal stent are considerably larger than those of the bile duct and biliary stent, it would be technically infeasible to fabricate a biliary stent loaded with 125I seeds. Such a stent would also increase the required diameter for the stent release system, thereby increasing tract puncture injury. Liu et al. (21) implanted 125I-seed–loaded endoprosthesis in the pancreatic and common bile ducts of patients with cholangio-carcinoma, pancreatic cancer, or ampullary carcinoma, and observed a median survival time of 150 days. However, the use of an endoprosthesis is associated with a short patency period and a high rate of jaundice recurrence. We performed ILBT using a 125I seed ribbon through a drainage catheter after stent insertion in patients with MOJ. The catheter containing the 125I seed ribbon could be fixed to the drainage catheter by a Y-configuration port to avoid dislocation.
The absorbed dose of 125I radiation obeys the inverse square law, i.e. the radiation dose at a given point is inversely proportional to the square of the distance from the source to this point. Because tissue adjacent to 125I seeds receives a high dose of radiation, the clinical safety of these seeds must be evaluated. Investigators have studied the safety of 125I seed ILBT in the esophagus and pancreatic duct. Guo et al. (22) placed metal stents loaded with 125I seeds in the esophagi of rabbits euthanized after 2, 4, and 8 weeks. They observed submucosal inflammation and slight epithelial hyperplasia, which peaked at 8 weeks after implantation. Liu et al. (23) endoscopically placed 125I-seed–loaded endoprosthesis in normal pig pancreatic ducts, and euthanized the animals at 14, 30, and 60 days after stent placement. They found necrosis of the pancreatic duct lining with angiogenesis and blood vessel congestion in their 14-day samples; the pancreatic duct gradually regenerated and recovered in animals that received lengthier treatments.
Radiation damage is similar in all mammals. Among animals currently available for experimentation, pig bodies and organs are closest in size to those of humans (e.g. human and pig common bile duct diameters are 6–8 mm and 4–6 mm, respectively). Thus, we chose to use pigs in the present study. The animals in this study experienced no vomiting or diarrhea after 125I ribbon placement. They gained various amounts of weight before sample collection, suggesting that 125I ribbon ILBT in the bile duct caused no obvious whole-body complication. White blood cell counts did not differ before and after implantation, indicating that ILBT did not involve the bone marrow. Although placement of the 125I ribbon reduced the effective volume of the common bile duct, the similarity in serum total bilirubin concentrations before and after implantation indicated that 125I ribbon ILBT did not affect bile drainage. Because the upper common bile duct is adjacent to the liver, radioactive seeds implanted in the bile duct will also irradiate the liver. However, we found no significant difference in serum aminotransferase concentrations before and after implantation, indicating that 125I ribbon ILBT caused no liver function damage.
The 125I ribbon ILBT caused some damage to the bile duct wall. The major findings of this study were epithelial cell loss and morphological changes, and inflammatory cell infiltration in the lamina propria. The damage was most severe in the 15-day group, samples from which also exhibited epithelial cell swelling, considerable loss of microvilli, and radiation damage to radiosensitive organelles. The epithelium had begun to heal at 30 days after implantation, and healing was nearly complete at 60 days. The epithelial cells had resumed their cuboidal shape by 120 days after implantation. The damage to the pig bile duct caused by 125I ribbon ILBT was thus repairable.
Eight weeks after implantation, Guo et al. (22) found absorbed doses of 16.2 Gy and 2.02 Gy at points 10 mm and 20 mm from the 125I seeds, respectively. Liu et al. (23) found absorbed doses of 50–200 Gy at points 5 mm from the seeds. In the above studies, the 125I seeds were arranged on the stent surface, off the axis of the stent or lumen. When a 125I-seed–loaded stent is placed in a lumen, the 125I seeds are in direct contact with the duct wall. According to the inverse square law, the absorbed dose at the duct wall contacting the 125I seeds should be much higher than at the reference points mentioned above. In addition, the dose distribution in the duct is highly asymmetric. Therefore, the absorbed dose at those reference points does not accurately reflect that in the section of duct wall under investigation. In the current study, the tissue absorbed dose at 3 mm (corresponding to the radius of the pig bile duct) from the midpoint of the 125I ribbon was taken to represent the absorbed dose at the bile duct. These absorbed doses authentically reflected the association between the radiation dose and the damage to the bile duct lining.
This study has a limitation in that we did not examine the effects of implanting 125I ribbon at the hilar bile duct. There are some technical problems in placing 125I seed ribbon the hilar bile duct of the pigs: (i) It is almost impossible to puncture a non-dilated intrahepatic bile duct for anterograde 125I seed ribbon placement in the hilar bile duct; (ii) because the hilar or intrahepatic bile duct is much thinner than the common bile duct, retrograde insertion of an 125I seed ribbon from the common bile duct to the hilar bile duct may injure the bile duct epithelium. We hope we can find a new method to examine the radiobiological effects of 125I ribbon on the hilar bile duct in the future.
In conclusion, this study demonstrated the safety of ILBT using a 125I ribbon in the pig bile duct. This technique may be applied to the treatment of the human bile duct. Future research should study the feasibility and clinical outcomes of MOJ treatment using a 125I ribbon.